
Research Article | DOI: https://doi.org/10.31579/2694-0248/050
1 Assistant professor of Orthopedics and Traumatology, Faculty of Medicine, Al-Azhar University, Egypt.
2 Professor of Orthopedics and Traumatology, Faculty of Medicine, Mansoura University, Egypt.
3 Professor of Orthopedics and Traumatology, Faculty of Medicine, Al-Azhar University, Egypt.
4 Assistant lecturer of Orthopedics and Traumatology, Faculty of Medicine- Al-Azhar University, Egypt.
5 Lecturer of Orthopedics and Traumatology, Faculty of Medicine- Al-Azhar University, Egypt.
*Corresponding Author: Barakat El-Alfy, Professor of Orthopedics and Traumatology, Faculty of Medicine, Mansoura University, Egypt
Citation: Ibrahim E. Abuomira, Barakat El-Alfy, Mahmoud Seddik, Khamis M. Ahmed, Sayed Khashaba, et al, (2023), A Modified Angled Plate for Fixation of Proximal Femoral Varus Osteotomy in Paralytic Hip Dislocation, J. Clinical Orthopedics and Trauma Care, 5(1); DOI:10.31579/2694-0248/050
Copyright: © 2023, Barakat El-Alfy. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 September 2022 | Accepted: 26 December 2022 | Published: 07 January 2023
Keywords: proximal femoral osteotomy; cannulated interlocking blade plate; modified angled blade plate; paralytic hip dysplasia
Objectives: Femoral osteotomy is an important step in the management of paralytic hip dysplasia. Fixation by the angled plate is demanding and carries the risk of many complications. In this study, we made certain modifications for the angled plate, and we aim to assess the results of the modified plate for fixation of proximal femoral varus osteotomy in paralytic hip dysplasia.
Method: Twenty patients with paralytic hip dislocation were included in this study. The ages ranged from 5 to 15 years with an average of 9 years. There were 12 boys and 8 girls. Seventeen patients had cerebral palsy and 3 had meningocele disease. Pre-operative radiographs were done, and the migration percentage (MP), acetabular index (AI), and neck-shaft angle (NSA) were measured. All patients were treated by open reduction, pelvic osteotomy, and proximal femoral varus osteotomy. The femoral osteotomy was fixed by the modified angled plate in all cases.
Results: The osteotomy sites united in all patients and the average time of union was 3 months. The acetabular index, migration percentage, and neck-shaft angle were reduced postoperatively. This reduction was statistically significant. The hips remained stable throughout the period of follow-up in all patients. No cases were complicated by nonunion or implant failure.
Conclusion:
The modified angled plate (canulated interlocking blade plate 90°) is a good method for the fixation of proximal femoral varus osteotomy in the management of paralytic hip dislocation. The modifications have made it easier for application and stable for fixation.
Hip affection in children with cerebral palsy (CP), Myelomeningocele, and other neuromuscular disorders range from the hip at risk to frank dislocation with significant affection for the patient quality of life [1-3].
Early surgical management of paralytic hip dislocation brings benefits to patients, by reducing their pain, improving their sitting position, and facilitating their hygienic measures. The goal of surgical treatment is to ensure that the femoral head is located perfectly in its anatomical position, without risk of dislocation. This is usually done by soft tissue release, open reduction, and proximal femoral varus osteotomy with or without pelvic osteotomy [4-6]. The pelvic osteotomy technique described by Dega that corrects anterior, lateral, and posterior acetabular deficiencies is widely accepted for the treatment of paralytic hip dysplasia [7].
The bone quality in such patients is usually poor and fixation of the proximal femoral osteotomy by the conventional angled plate is difficult and carries the risk of mal tracking, loosening, and implant failure [8, 9].
In this study, we introduced certain modifications for the cannulated angled plate, and we hypothesized that this new system would offer significant advantages over the existing systems in terms of easy application and stable fixation.
The aim of this study is to assess the results of the new modified plate for fixation of proximal femoral varus osteotomy in paralytic hip dislocation.
In this prospective study, 20 cases with paralytic hip dislocation were treated in our institution in the period between May 2016 and August 2020. The ages ranged from 5 to 15 with an average of 9 years. There were 12 boys and 8 girls. The mean weight of the patients was 21.9 kg (range 14–31.5 kg). The pathology was cerebral palsy in 17 cases and myelomeningocele in three cases.
Patients were evaluated clinically for the range of movement, leg length discrepancy, muscle power, and unilateral or bilateral affection. Plain radiographs were done for both hips and the acetabular index (AI), migration percentage (MP), and neck-shaft angle (NSA) were measured (Figure. 1) [10].
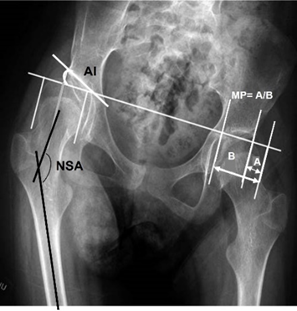
Figure 1: Theacetabular index (AI), migration percentage (MP), and neck-shaft angle (NSA) are measured.
Preoperative planning for hip reduction and femoral osteotomy with or without pelvic osteotomy was done.
The cannulated angled plate was modified in certain ways to be more stable for fixation (Figure. 2).

Figure 2-a: The profile of the plate was decreased from 4.5 to 3.5 and the 2nd angle of the plate was reduced from 42.5° to 20°.

Figure 2-b: An inter-fragmentary 3.5 locked screw was designed from the shaft of the plate to the blade in an oblique direction by 30°.
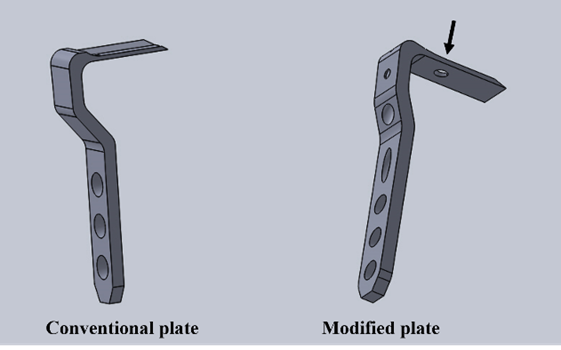
Figure 2-c: A hole was made in the blade to receive the tip of the oblique screw.
The modified plate was made of grade 4 pure titanium designed for medical application. We call it the cannulated interlocking angled plate.
All patients were treated by open reduction of the dysplastic hip, proximal femoral varus osteotomy, and pelvic osteotomy. The varus osteotomy was fixed by the modified plate in all patients. Informed consent was obtained from the patients and their relatives before surgery. The study was app39roved by the institutional review board (IRB).
Surgical technique
The patient was put supine on a radiolucent operative table. After preparation of the affected limb, a bikini incision was used to approach the affected hip. The interval between the iliopsoas and sartorius was developed. The lateral cutaneous nerve of the femur was identified and retracted laterally. The iliopsoas tendon was released. The reflected head of the rectus femoris was disinserted and retracted laterally to expose the anterior part of the capsule, and then a T-shaped incision was made in the capsule to expose the head. The acetabulum was cleaned from its fibrofatty tissue, and the transverse ligament of the acetabulum was incised. The head was then reduced and a capsulorrhaphy was performed. [11, 12] The proximal femur was exposed through a separate incision. A suitable point for entry of the guidewire was marked over the lateral aspect of the proximal femur. The guidewire was inserted through this point into the center of the femoral neck and confirmed on both AP and lateral radiographic projections (Fig. 3-a). Another two wires were inserted at the lesser trochanter level, making an angle equal to the angle of correction (Fig. 3-b). The cannulated seating chisel was used to cut a track for the blade plate by gentle hammering of the chisel over the guidewire (Fig. 3-c). The varus proximal femoral osteotomy was then performed by an oscillating saw along the second and third wires. The wedge of bone with its base medially was removed and the osteotomy surfaces were coopted to correct the deformity. The plate was inserted over the guidewire after removal of the seating chisel (Fig. 3-d). The osteotomy was reduced, and the plate was fixed to the femoral shaft. First, a nonlocking screw was used to produce compression at the site of the osteotomy. Then fixation was completed by the locking screws.
The interfragmentary 3.5-locked screw was taken from the shaft of the plate to the blade in an oblique direction at 30° to give more stability for the plate and prevent backing out of the blade from the neck.
Both anteroposterior and lateral fluoroscopic projections were taken to check the plate position. The stability of fixation was tested by putting the hip in different ranges of movements. Dega pelvic osteotomy was done to correct the acetabular insufficiency (Fig. 3-e). The wound was closed in layers. The average hospital stay was 5 days. Sequential radiographs were obtained postoperatively at 6 weeks, 3 months, 6 months then every year. At the final follow-up, the acetabular index, the neck-shaft angle, and the migration percentages were measured.
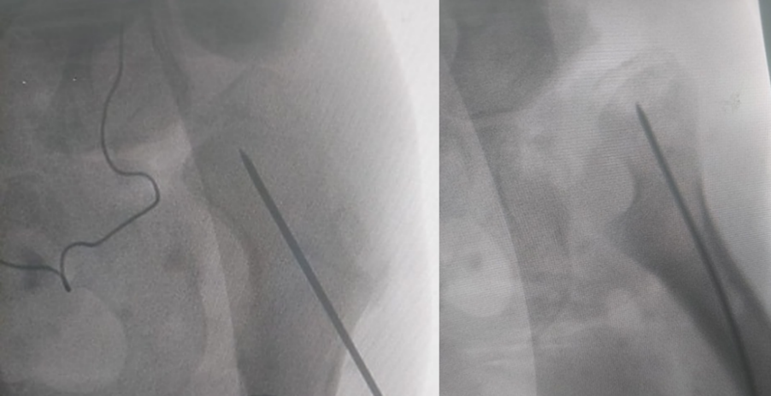
Figure 3-a: The guidewire is inserted in the center of the femoral neck and confirmed on both AP and lateral radiographic projections.

Figure 3-b: Another two wires are inserted at the lesser trochanter level, making an angle equal to the amount of correction.
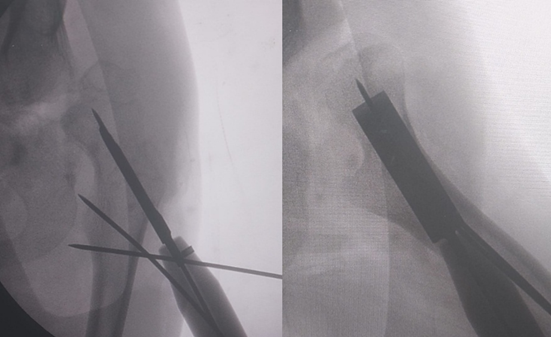
Figure 3-c: The cannulated seating chisel is used to cut a track for the blade plate by the gentle hammering of the chisel over the guidewire.
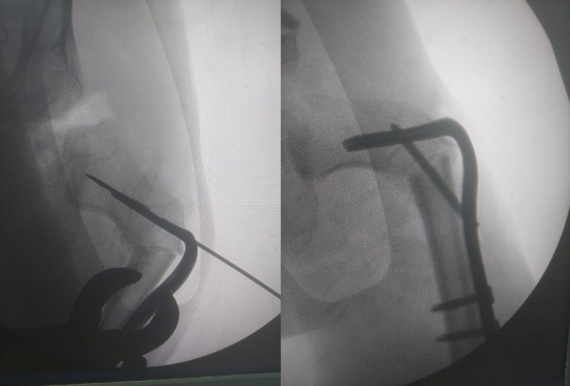
Figure 3-d: The blade plate is inserted over the guidewire and fixed to the shaft. The interfragmentary 3.5 locked screw is taken from the shaft of the plate to the blade in an oblique direction of 30°.
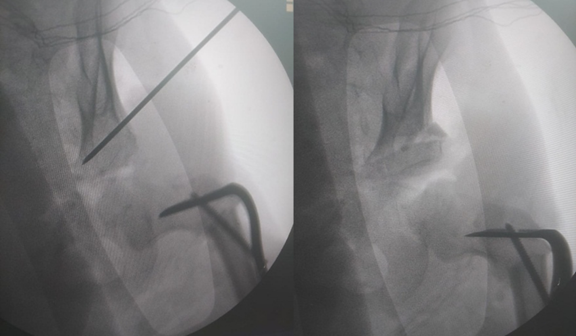
Figure 3-e: Dega pelvic osteotomy is done to correct the acetabular insufficiency.
The operative time ranged from 70 to 120 minutes with an average of 90 minutes. The average follow-up period was 19 months (range, 13 to 42 months). The time of union ranged from 1.5 to 5 months with an average of 3 months (Fig. 4). The mean preoperative NSA was 155.6° and the mean postoperative was 110.6°, with an average reduction of 35.1°.

Figure 4-a: 4-year-old male patient with CP presented with paralytic dislocation of the right hip.
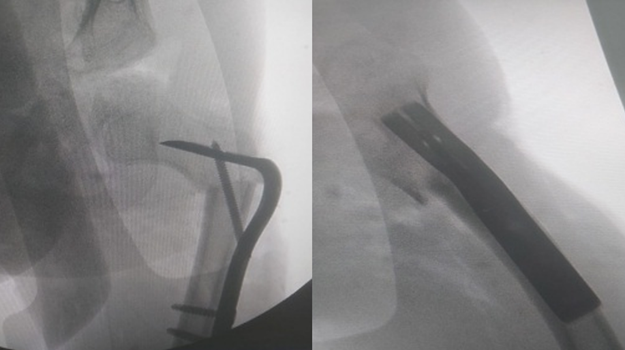
Figure 4-b: He was treated with open reduction, femoral osteotomy, and fixation by the modified plate.

Figure 4-c: The radiographs 3 months after surgery with complete healing of the osteotomy site.
Regarding the AI, the mean reduction was 14.38°, with pre and postoperative means of 38.03° and 23.65° respectively. Also, the MP presented a mean reduction of 79%, with pre and postoperative means of 90% and 11%. respectively. A significant difference was observed between pre and postoperative NSA and AI (p < 0>p < 0>Parameters Preoperative mean Postoperative mean Mean Of reduction P value NSA 155.6° 110.6° 35.1° < 0> AI 38.03° 23.65° 14.38° < 0> MP 90% 11% 79% < 0>
NSA: neck shaft angle, AI: acetabular index, MP: migration percentage.
Table 1: Summary of radiographic indices pre and postoperative with P value.
The gait improved in the ambulant patients. The families reported improvement in the seating position and personal hygiene in all patients. Two cases were complicated by superficial wound infection, and they were treated by local wound care and systemic antibiotics. No cases were complicated by delayed unions, nonunion, skin irritation from the plate, or loss of fixation. There were no revision procedures due to implant-related complications.
The prevalence of paralytic hip dislocation in patients with spastic CP is directly proportional to the degree of functional impairment. Failure to identify this dislocation early may lead to significant pain, pelvic tilt, and spine deformity with severe limitations on the patients’ quality of life. The population-based surveillance program was established in certain countries and resulted in a significant reduction in the incidence of hip dislocation in children with cerebral palsy [13-16].
Early surgical interference will reduce the patient's pain, improve function, and prevent further deterioration of the hip condition. Osteotomy of the proximal femur is an important step in the reconstruction of the dysplastic hip in patients with paralytic disorders [4-6]. The internal fixation device is specially adapted to the osteoporotic bone in patients with neurological diseases. Three systems of fixation are in common use for correction of proximal femoral osteotomy: AO angled blade plate, AO anterior plate, and the LCP (locked compression plate). Each one has its advantages and disadvantages [17-19].
Several studies have supported the use of fixed angle plate in the fixation of the proximal femoral osteotomy [8, 20].
Although good, many complications had been reported with the conventional fixed-angle blade plates. These complications may be early as wrong direction or loosening of the blade within the neck of the femur or late such as delayed union, nonunion, avascular necrosis, backing out of the plate, fractures under the plate, and periarticular osteophytes. These ossifications may result in bone bridges which may cause severe stiffness and deformities [8, 9].
Mal-tracking of the blade in the neck femur is a common complication with the conventional plate. Grant and colleagues described the cannulated blade plate in 1990 to avoid this complication. The guidewire must be inserted properly, and the seating Chesil and the plate will follow it without mal tracking [21, 22].
In this study, we introduced certain modifications for the cannulated angled blade plate to increase its stability for fixation (Table 2).
| Items | Conventional | Modified |
| Profile | 4.5mm | 3.5mm |
| Interfragmentary screw | absent | present |
| 1st angle | 90° | 90° |
| 2nd angle | 42.5° | 20° |
| Screw | 4.5mm | 3.5mm |
| Length of blade | 35, 40, 45, 50mm | 35, 45, 50mm |
| Length of shaft | 73.85mm | 81.82mm |
Table 2: Comparison between conventional and modified angled plate.
The modified plate was used for fixation of proximal femoral varus osteotomy in the surgical management of paralytic hip dislocation in 20 patients. The osteotomy site united in all patients and the average time of union was 3 months. There was a significant reduction in the radiological parameters in all cases postoperatively. The hip joint remained stable throughout the period of follow-up without further dislocation or subluxation (Fig. 5). No cases were complicated by nonunion, backing out of the blade, or implant failure which reflect the stability of the construct. No skin irritation was observed in the trochanteric region from the plate.
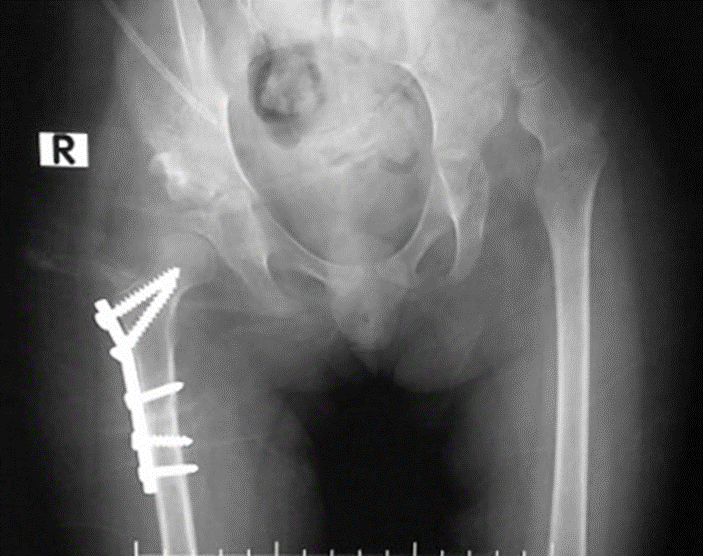
Figure 5-a: 5-year-old girl with myelomeningocele presented by bilateral hip dislocations. The right side was treated surgically before.
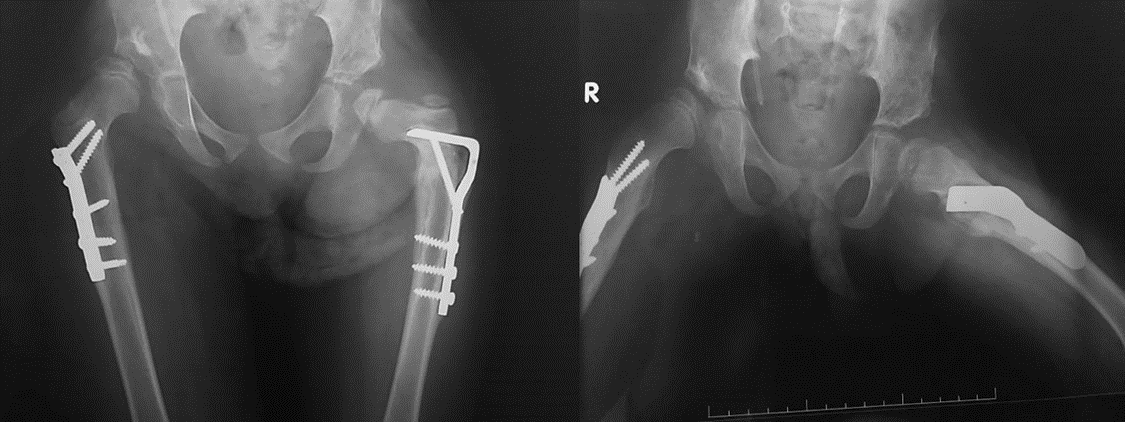
Figure 5-b: The radiographs 6 months after surgical treatment of the left side by pelvic osteotomy, femoral osteotomy, and fixation by the modified angled plate.
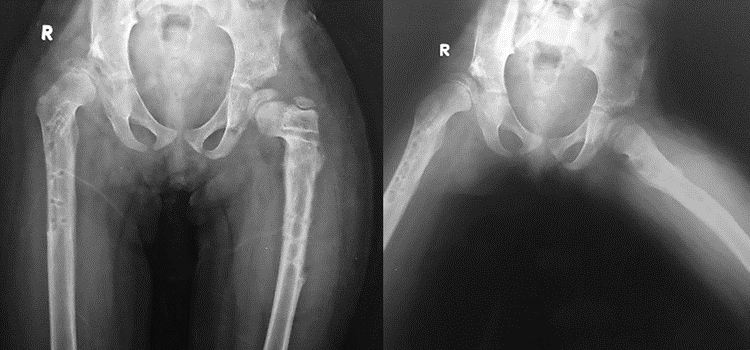
Figure 5-c: The radiographs after removal of the implant 3 years after surgery. The left hip is still reduced and stable.
Because of the poor nutrition state and poor walking ability of children with the paralytic disorder, the bone is usually osteoporotic and the problem of implant failure especially backing out of the plate is common. Several trials were done to increase the degree of fixation stability in those patients. Some authors used the locking plate and others take an interfragmentary screw from proximal to distal fragments outside the plate after proximal femoral varus osteotomy. [8, 19] In this study we designed an interfragmentary 3.5 locked screw from the shaft of the plate to its blade in an oblique direction of 30°. This screw has many advantages as it fixes both the proximal and distal bone fragments to each other and the plate blade. It prevents backing out of the plate. Also, it supports the blade and prevents further varus collapse.
Reduction of the second angle of the plate from 42.5 degrees to 20 degrees decreases the prominence of the plate under the skin and still produces medialization of the distal fragment which is required in such cases.
The new angled plat (cannulated interlocking blade plate 90°) offers great advantages over the conventional plate in terms of easy application, high stability, short operative time, and decreased prominence under the skin. This study's clinical and radiological results favor using this plate in the fixation of proximal femoral osteotomy in paralytic hip dislocation.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
