
Research Article | DOI: https://doi.org/10.31579/2690-4861/122
1 Petz Aladár University Teaching Hospital 9023 Győr, Vasvári Pál u. 2-4. HUNGARY.
2 Széchenyi István University, Győr 9026 Győr, Egyetem tér 1.
*Corresponding Author: Mihály Fücsek, 9022 Győr, Árpád u. 77 / B. 2nd em. Door 4. HUNGARY.
Citation: Fücsek M, Molnárka GY. (2022). A Mathematical Model of Middle Ear Ventilation. Controlled Valvular Tympanostomy Tube. J. Biomedical Research and Clinical Reviews. 7(1); DOI:10.31579/2690-4861/122
Copyright: © 2022 Mihály Fücsek, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 May 2022 | Accepted: 06 June 2022 | Published: 15 June 2022
Keywords: middle ear ventilation; mathematical model; gas diffusion; valvular tympanostomy tube; tympanostomy tube
BAKGROUND
The middle ear (tympanic cavity and mastoid process) is a closed cavity. It is filled with a special gas mixture and at the same pressure as atmospheric air, the composition of the gas is similar to the surrounding tissues. Its change in pressure is compensated by the occasional opening of the Eustachian tube. If the tube does not open, a persistently high negative pressure develops in the middle ear, the clinical consequences of which are well known. The negative pressure is eliminated by a tympanostomy tube implanted in the tympanic membrane. Inserting the tube instead of one abnormal condition (permanently closed middle ear) creates another abnormal condition (permanently open middle ear). Prolonged insertion of the tube may cause irreversible damage. / eardrum atrophy, tympanosclerosis, permanent perforation, auditory bone damage, cholesteatoma /.
AIM
We are looking for a solution that is similar to the original, i.e. the middle ear should be closed and open from time to time.
METHOD
We studied middle ear ventilation based on literature data, our own research, and our computer model.
RESULTS
We concluded that the original function can be restored with the valve tube. In our case, the opening and closing of the valve is controlled by a change in volume caused /diethyl ether/ by a change in body temperature.
CONCLUSION A more advanced solution would be a nanotechnology valve controlled by a change in total pressure, a partial pressure change in oxygen or carbon dioxide. However, a valve that can be opened at different intervals or even individually adjusted is conceivable.
The middle ear /ME/ is a closed, special gas mixture filled cavity.[1-6] Closing is passive. The pressure changes of the ME are compensated by the actively opening Eustachian tube /ET/.
Otitis media is a common disease in childhood. Permanently decreased in middle ear pressure caused by ET dysfunction is one of the fundamental factors in the pathology of otitis media.
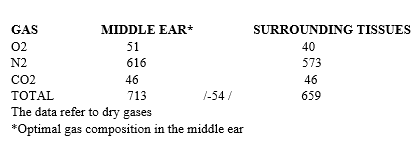
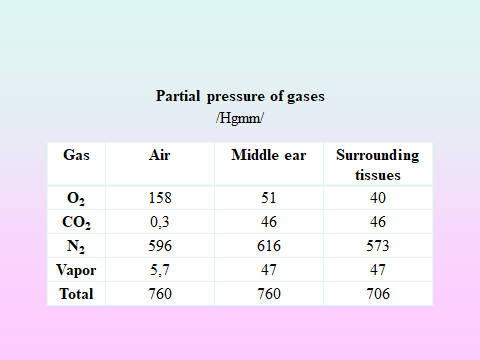
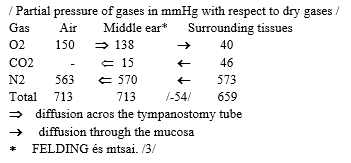
The ME / tympanic cavity and mastoid process / pressure is provided by gas diffusion and ET function. Gas diffusion between the surrounding tissues /ST/ and the ME takes place in accordance with the laws of physics (bidirectional gas exchange), so the pressure from the diffusion in the ME, can be a maximum of 706 mmHg. (Table 1) That is, 92% of the ME pressure is provided by the gas diffusion, and 8% by the ET (Table 2).
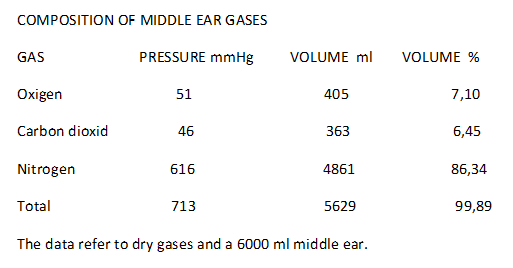
The pressure and gas composition are provided by complex active and passive mechanisms operating in harmony with each other, including the nasopharyngeal biphasic pressure wave, the mastoid process volume and the tension and elasticity of the eardrum. ME volume is an important pathological factor. Diffusion of the same quantity of gas (O2, N2, CO2) causes a greater pressure change in a smaller volume middle ear.
If the ET does not open, the partial pressures of the gases / O2, N2/ are equalized between the ME and ST and negative pressure develops in the middle ear with well-known clinical consequences.
The importance of negative ME pressure in pathology is demonstrated by many millions of measurements / tympanometry / daily around the world.
The pathological process attempts are made to prevent by inserting a tympanostomy tube.
The long-term effects of tube insertion have been analyzed in several studies [7-10].
The consequences of tube insertion
After tube insertion, the pressure in the ME is restored but the gas composition of the ME changes[11-13]. The gas composition of the ME will be more similar to air than to the gas composition of the ST. The larger lumen of the tube, the more the gas composition of ME resembles air rather than the gas composition of ST (Table 5).
Intermittent pressure equalization, which under intact conditions is the result of a dynamic process and intermittent, will be continuous and passive. This passivity can lead to structural damage.
The partial pressure of oxygen in the ME is too high, therefore the absorption of oxygen into the ST increases / hyperoxia /.
Strong, continuous diffusion of carbon dioxide begins from the surrounding tissues into the cavity of the ME, causing the ST to lose large amounts of CO2.
The ME loses water vapor / 100% humidity in the intact middle ear / thus the mucous membrane dries out and is damaged.
Inserting the ventilation tube instead of one abnormal condition (permanently closed middle ear), does another (permanently open middle ear).
So we did not restore the original condition by inserting the tube. The ear may compensate for our therapy in the short term, but with repeated or prolonged tube insertion, side effects may occur (atrophy, scarring, tympanosclerosis, perforation of the eardrum, damage to the auditory ossicles, cholesteatoma, and hearing loss).
We are looking for a solution that creates conditions similar to intact ventilation, i.e. the middle ear should be closed and open from time to time. We examined the ventilation of the middle ear based on known literature data and our own research. Intact middle ear ventilation was analyzed using a mathematical model.
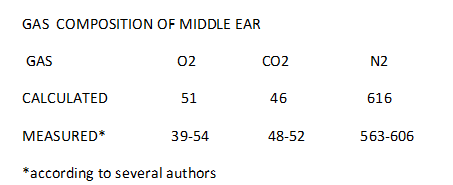
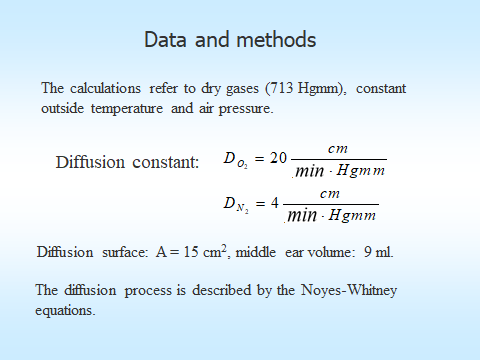
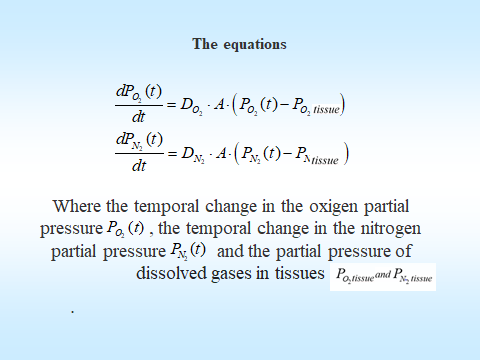
Our calculations refer to dry gases (713 mmHg), constant outside temperature and air pressure. The diffusion constants are shown in the Table 6. Diffusion surface: A = 15 cm, middle ear volume: 9 ml. Diffusion processes are described by the Noyes-Whitney equations. Table 7. The ET performs pressure equalization every minute.
Basic physical concepts: The gases flow across the ET according to their percentage composition from the higher pressure point to the lower pressure point.
The gases diffuse across the mucosa according to their partial pressure difference.
The process was analyzed for O2 and N2 gases only.
The diffusion of gases at constant atmospheric pressure shows Table 8.
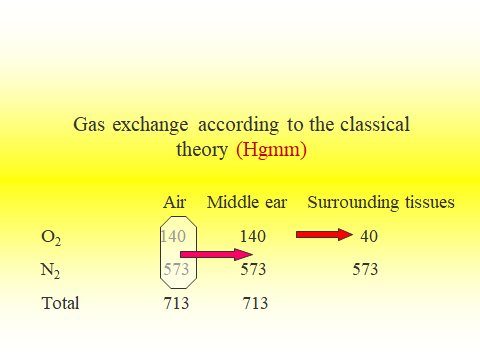
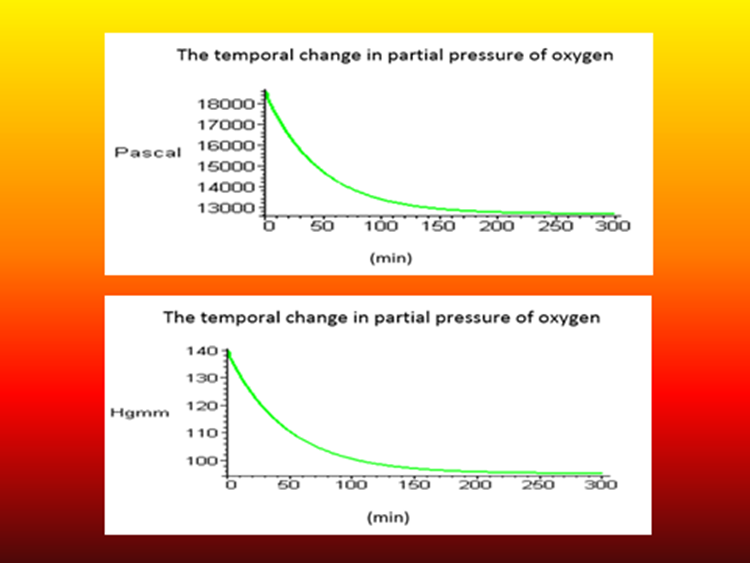
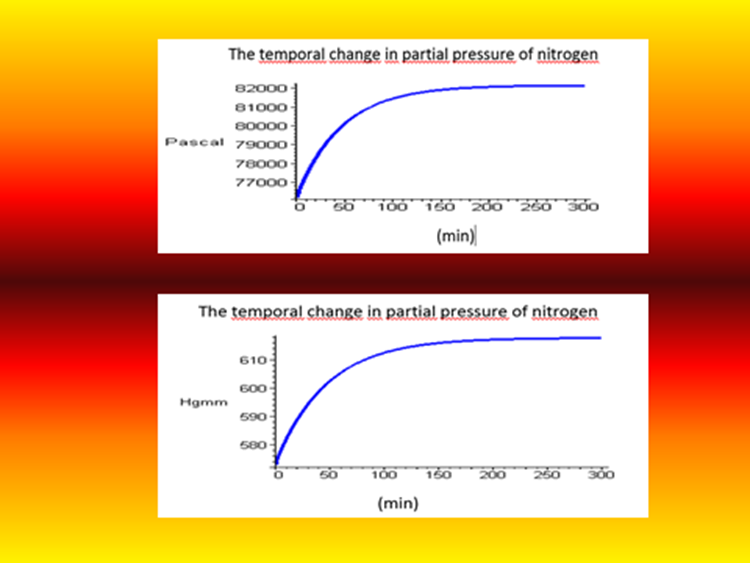
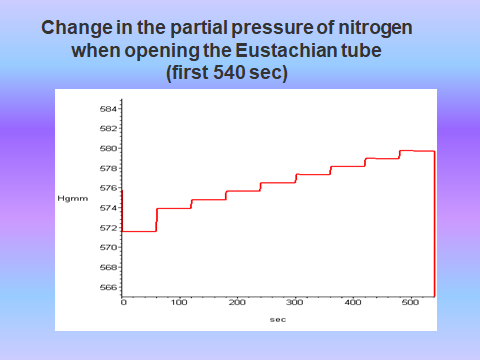
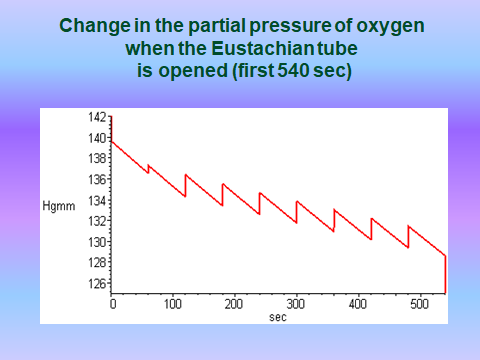
This is actually the classic theory. The middle ear is filled with air / 21% oxygen, 79% nitrogen /. Oxygen diffuses in the ST according to its pressure gradient, the pressure in the ME cavity decreases. The ET opens and compensates for the pressure decrease with air (21% oxygen, 79%
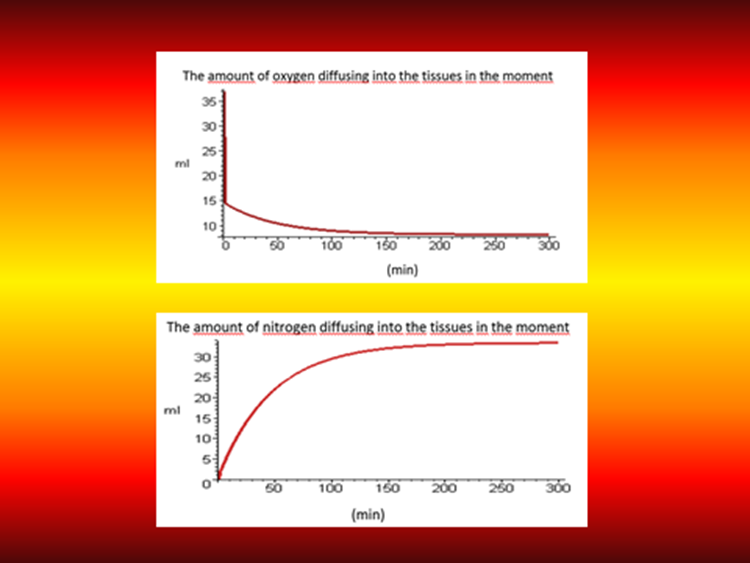
nitrogen). Therefore, the partial pressure of oxygen decreases and that of nitrogen increases in the ME (Figure 1,2.) As a result, at one point, more and more nitrogen diffuses into the surrounding tissues (Figure 3).
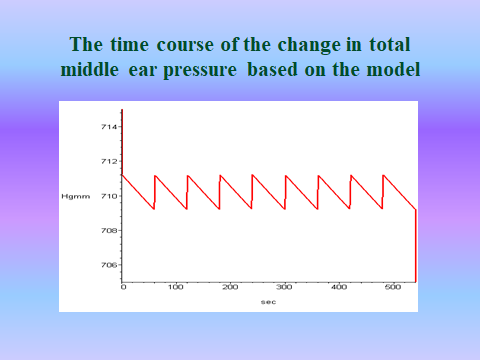
If nitrogen is replaced by air, the process is reversed. The partial pressure of oxygen increases and that of nitrogen decreases. The two processes take place in parallel, then process stabilizes when the ratio of nitrogen to oxygen absorption is 21:79 as it is replaced or the same amount of gas is absorbed from oxygen and nitrogen. /Supporting information/ The partial pressure changes of O2 and N2 and total pressure are shown figures 4-6. Gas exchange takes place in a similar way, starting from the optimal gas composition, only the equilibrium state is reached earlier in time. (Table 2,3).
A similar process takes place with increasing air pressure. When the ET opens, air flows into the middle ear. The partial pressures of O2 and N2 increase by 21:79, the absorption of O2 and N2 increases, absorption ratio changes slightly and then returns to 21:79. With constant and increasing air pressure, the partial pressure of carbon dioxide is essentially unchanged, which corresponds to the surrounding tissues.
The steady state lasts until the air pressure changes.
As the air pressure decreases, if the ET opens the gases flow outwardly through the ET according to their percentage composition and reduce the partial pressures of oxygen, carbon dioxide, and nitrogen in the ME. In the normal state, the partial pressure difference of O2 and N2 between the middle ear and the surrounding tissues is around 50-60 mmHg /Supporting information/. This pressure difference is sufficient to compensate for the athmospheric pressure decrease. As the diffusion coefficient of carbon dioxide is the best (20 times better than oxygen /, a slight, transient pressure increase may occur in the middle ear.
In the event of a sudden drop in air pressure greater than 50-60 mmHg, if the partial pressures of O2, N2, and CO2 in the ME fall below the level of the surrounding tissues, O2, N2, and CO2 may diffuse into the middle ear. This can cause a transient, two-peak pressure rise in the ME. / CO2 faster and bigger wave, O2 and N2 slow, elongated curve./
Compensating for a sudden drop in air pressure is the most difficult task in middle ear ventilation.
With increasing and constant air pressure, the Eustachian tube equalizes towards the middle ear cavity, with decreasing air pressure, it equalizes towards the outside world, in which case the direction of diffusion may change according to the partial pressures differences in the middle ear.
Because diffusion and flow through the ET is a passive process, the ME ventilation is controlled by the active ET opening.
The ET creates, the gas diffusion equalizes for the partial pressure differences between the middle ear and the surrounding tissues.
THE MIDDLE EAR VENTILATION CHARACTERISTICS.
Gas flow across the ET and gas diffusion between ME and ST is a two-way process.
The ME pressure decrease is always equalized with air (21% O2, 79%N2)
The pressure decrease is caused by the absorption of O2 and N2 in the middle ear.
A pressure equalizes /air flow/ and the gas diffusion passive process
The gas diffusion continuous, the pressure equalization intermittent.
Diffusion of a certain amount of gas (O2, N2, CO2) causes a greater pressure decrease in a smaller volume in the ME.
In the ME the pressure decrease due to nitrogen or oxygen absorption is always compensated by air /21% Oxygen, 79% Nitrogen/. When the absorbed oxygen or nitrogen is replaced by air, it changes the partial pressure of oxygen and nitrogen in the ME in the opposite direction.
Ventilation of the ME is the result of a complex, dynamic process controlled by the active ET opening. The ME is a closed cavity, which is opened time to time. This is the most important statement of ME ventilation.
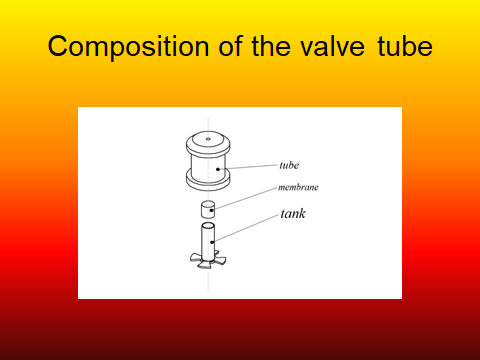
We designed a valve tube that is closed and opens intermittently.
Accordingly, we designed a tympanostomy tube that performs this task.
VALVULAR TYMPANOSTOMY TUBE
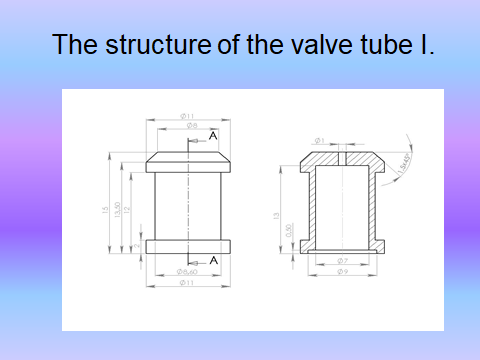
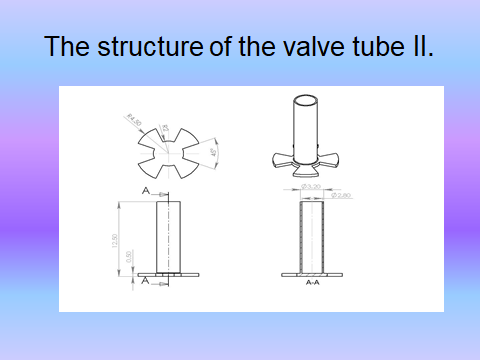
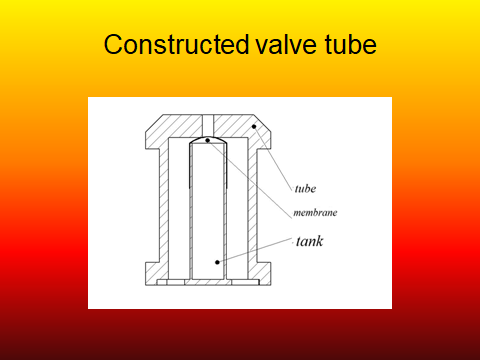
The following figures 7-10 show the structure of valve tube
The temperature of the human body can vary widely. It is known that in muscle work, body temperature can be as high as 40 degrees Celsius.
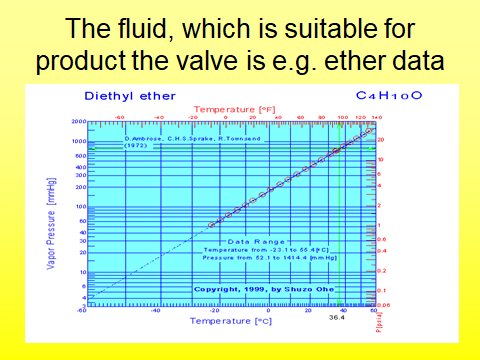
The valve container should be filled with a fluid boiling point around body temperature to move the valve diaphragm. The membrane material is flexible or flexible plastic. During physical activity, the body temperature rises and the liquid enclosed in the tank boils, expands, which closes the valve. At rest, the body's temperature decreases, the fluid cools, its volume decreases, thus opening the valve. Diethyl ether (C4H10O) has a boiling point of 36.4 ° C and may be suitable for valve operation (Figure 11).
Our valve tube is regulated by the volume change due to the change in body temperature, its preparation is a technical task.
The operation of the valve can be controlled by the full pressure difference, the partial pressure differences, the pulses of the chemo-mechanoreceptors. By setting the opening time, changes due to the surface / volume ratio can also be compensated and monitored. The idea can probably be solved with nanotechnology.
Abbreviations
ET :Eustachian tube
ME :middle ear
ST :surrounding tissues
PP :partial pressure
PPD :partial pressure difference
Competing Interests
The authors declare that they have no competing interests.
Acknowledgements
The authors are grateful to Dóra Gurabi MD, for correcting the manuscript in English.
Funding information
The 2006 check INKOND- TUBEDRFM 47-43 / 2006 supported the research on the computer model and the valve tube.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
