
Editorial Note | DOI: https://doi.org/10.31579/2637-8892/026
Bluegreen-technologies, Heelsum, The Netherlands.
*Corresponding Author: Vincent J.T van Ginneken, Bluegreen-technologies, Heelsum, The Netherlands
Citation: Vincent J.T van Ginneken, (2018) A Greedy Man in a Hungry World”: does hunger lead to depression and anxiety?, J Psychology and Mental Health Care. 2(2); DOI: 10.31579/2637-8892/026
Copyright: © Vincent J.T van Ginneken. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 13 April 2018 | Accepted: 19 April 2018 | Published: 26 April 2018
Keywords: depression; anxiety; emotionally
We live in a divided world with reasoning for depression and anxiety (Figure 1). I say something rude -because it touches me emotionally- while on the other side of the world in the US children are doing suicide because they are obese (BMI> 30).
We live in a divided world with reasoning for depression and anxiety (Figure 1). I say something rude -because it touches me emotionally- while on the other side of the world in the US children are doing suicide because they are obese (BMI> 30) [1], at the same time, a huge number of children are dying - mainly in East Africa in the sub-Saharan region as a result of hunger in combination with war. These scientific facts support my perception that we live in a divided, torn "Hunger-Obesity" world, and although the phenomenon of hunger has been less common since the 1990s, it seems as if people in developed countries have become emotionally insensitive to this phenomenon because this phenomenon is far away from the Industrialized Western World or Developed countries. In 1991, only a select number of developing countries had undernourishment levels <5>


Figure 1: The present Hunger-Obesity paradox, we live in a divided World.
Presently East Africa, Yemen and north-east Nigeria are in the grip of an unprecedented and devastating food crisis [3]. Famine has been declared in South Sudan and is already likely happening in parts of in northern Nigeria, while Yemen and Somalia are on the brink. This is the largest hunger emergency in the world with about these regions, about 30 million people are experiencing alarming hunger, surviving only on what they can find to eat [3] According to UNICEF, 27 million people lack safe water, increasing the threat of cholera and spreading other water-borne diseases such as diarrhoea. Malnutrition is having a disastrous impact and as ever, children are among the worst affected. If these crises are left unresolved, malnutrition and deaths will increase exponentially in a catastrophic deterioration. United Nations warned as many as 1.4 million children could die of starvation in the coming months [4]. While at this time for the victims of this famine food supply is a top priority, I raise in this editorial the scientific question: “whether hunger distress is accompanied with depression and anxiety and whether at all biomarkers for human starvation/hunger stress exist”. These issues are important to answer in order to help traumatized victims during the famine, not solely with food, but with mental support or afterwards during their nutritional recovery period. If we see figure 2 which is a global map for “national happiness rankings” (a rough indicator for the parameters depression & anxiety) how this “emotion” is distributed on our planet, it seems that relatively most unhappy people live at the African continent which is stroke by famine and war. Brutal conflicts in South Sudan, Yemen and Nigeria have driven millions of people from their homes and left millions more in need of emergency food. [3].
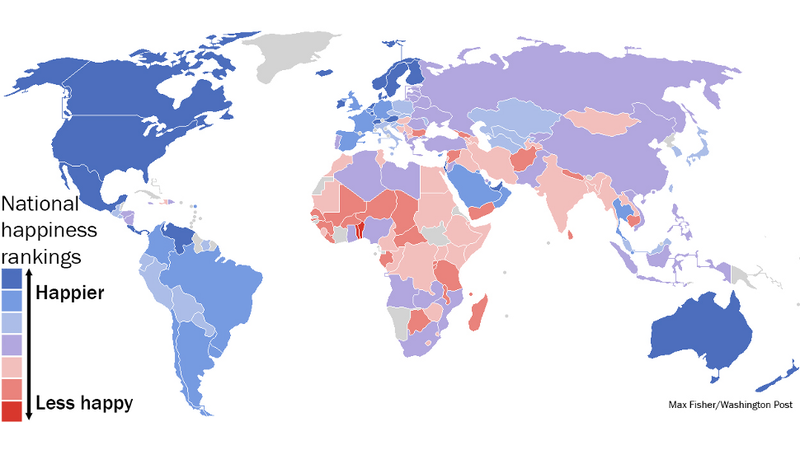
Figure 2: Global map of “National happiness rankings” per country (Courtesy: Max Fisher).
Because this topic of hunger in the world was reviewed at an earlier time, mainly from a physiological and biochemical point of view [5], we also found a lipid hunger biomarker in a C57bl6 mouse model after 48 hours of hunger [6]. In my view, this is an unexplored field of research because we live in a divided world and there is actually no interest in this subject.
But the most important question we raise is: “Does hunger results in major depression or anxiety prior to a hunger death?” will remain unanswered. This remains an undissolved question, probably because the question blends many research areas like philosophy, psychology & neuroscience. What we hope to achieve -and is the major mission of blue-green technologies foundation (www.bluegreentechnologies.nl)- that from moral, ethical and empathy for every human citizen on our globe we will not accept towards the 10 billion people at A.D. 2050,[7] hunger has been there and always will be there.
Since at present A.D. 2018 around one billion people are exposed to hunger (<200>
In our earlier review [5] we outlined the classical but as later considered grueling study of Ancel Keys (1950), in the so called “Minnesota Starvation Experiment” which delivered a standard work “The Biology of Human Starvation” [9]. The "volunteers", received 3 months 3200 kcal / caput / day followed by 6 months or "semi-starvation" at 1800 kcal / caput / day. During this semi-starvation period most of the participants lost> 25% of their body weight. The final three months were a nutritional rehabilitation period [10].
In 1950, Ancel Keys and his colleagues published the results of the Minnesota Starvation Experiment in a two-volume, 1,385 page text entitled The Biology of Human Starvation (University of Minnesota Press). Here is a summary of what they found [9].
These are all symptoms of anxiety and mood disorders as well as symptoms of eating disorders. These results
indicate that the brain’s functioning is highly compromised when the body is being starved of food and nutrients [9]. In general, this starvation period or “Hunger experience” was considered by most “volunteers” as psychologically traumatic with a tremendous impact during the rest of their lives. I quote an interview one of the volunteers released: food became an obsession.
"I don't know many other things in my life that I looked forward to being over with any more than this experiment. And it wasn't so much ….because of the physical discomfort, but because it made food the most important thing in one's life-…..food became the one central and only thing really in one's life. And life is pretty dull if that's the only thing. I mean, if you went to a movie, you weren't particularly interested in the love scenes, but you noticed every time they ate and what they ate". [5, 10].
Because of the results of the experiment of [9], it is now generally acknowledged that starvation alters personality and that nutrition directly and predictably affects mind as well as body [10]. Disturbances in food pattern like food- deprivation, anorexia nervosa, bulimia nervosa, cachexia and obesity are nowadays considered as "diseases" affecting cognitive and social functioning of the patient [5, 10].
In fact, as described in the review of van [5] an acute chronic hunger death, lasting at maximal 10 days due to acute chronic starvation (≈0 kcal/caput/day), is the most terrifying death a human can dye. It is so genially organized via clear physiological and biochemical pathways with the liver as central operator (Figure 3).
In this way, these mechanisms provide the human brain of a starving person continuously and instantaneously of fuel like glucose, ketone bodies, until the last amino acid are burned. This will result that the Body Mass Index (BMI) -an antropometric parameter which is a global index to define underweight, overweight or obese- dwindles. This is an index of a person’s weight in relation to height; determined by dividing the weight (in kilograms) by the square of the height (in meters) and will drop below some standard of acceptable weight during starvation (< 200>can assume it will be accompanied with depression and anxiety because starvation and famine are probably one of the most extreme stressors in nature [12]. To our knowledge the effects of these physiological processes on depression and anxiety have hardly been investigated and there are no clear direct medical indications of the impact of hunger on mental suffering, even though signs of pain in cachexia patients are dampened by morphine in the developed countries [13].

Figure 3: Overall scheme of starvation fuel metabolism. Liver derives its major energy by partial oxidation of FFA to β-hydroxybutarate and acetoacetate; muscle and kidney by complete oxidation of FFA to CO2 and H2O. Brain utilizes both β-hydroxybutarate and acetoacetate and glucose. FFA, free fatty acids; RBCs, red blood cells [Source: 3].
We talked about children in the US who do suicide because they are obese: "The Bell Jar of Obesity" [1]. In contrast, the phenomenon of suicide due to hunger in the medical literature is rare [14]. From this we can conclude that death by hunger is not a choice of its own. But what lessons can we learn about the disease anorexia nervosa, an obvious contender of obesity and an extreme form of self-hunger, to which a relatively large amount of research has been done [15; 16]. Based on the mental health situation of anorexia nervosa patients, we can possibly get an impression of whether this is associated with depression and anxiety. Anorexia nervosa eating disorders frequently co-occur with other psychiatric disorders, such as depression, substance abuse, anxiety disorders, and borderline personality disorder [15]. In addition, neurological information of the brain is available of anorexia nervosa patients related to ghrelin. Ghrelin which was found in 1999, is a peptide hormone produced and secreted in the stomach [17]. Leptin and ghrelin are two hormones associated with multiple physiological functions, especially energy balance. Leptin is an adipocyte-secreted hormone discovered in humans in 1995 [18]. In addition, probably one of the most important genes that play an important role in heredity obesity is the gene for production of ghrelin [19]. The equilibrium between insulin, leptin and ghrelin are responsible for normal appetite and normal body weight. [20, figure 4]. Leptin gives us a feeling of satisfaction. While ghrelin enhances appetite, leptin acts as a satiety signal to diminish it. Yet, it's not that simple. There are multiple receptors in fat cells. These produce other hormones, which can interfere in our response to food intake. A balance exists between your fat cells and your appetite (figure 4).

Figure 4: The equilibrium between insulin, leptin and ghrelin are responsible for normal appetite and normal body weight [20].
In anorexia nervosa, some of the symptoms classically described might be due to a resistance or insensitivity to ghrelin effect [16]. So whatever the cause may be for anoreaxia nervosa, one may come to the conclusion of a complete mental derailed system and again which is a nearly unexplored research area [21].
Mood disorders are affecting a major amount of the world population [22]. In this editorial I would therefore emphasize on these recent findings which raise a potential link between the hormone ghrelin and these disorders of mood [23]. The secretion of ghrelin is altered in several psychiatric disorders (e.g. anorexia) as well as in metabolic disorders (starvation vs. obesity) and in animal models in response to emotional triggers (psychological stress like starvation) but the relationship between these modifications and the physiopathology of psychiatric disorders remains unclear [23]. Recently, a large amount of literature showed that this key metabolic/endocrine regulator is involved in stress and reward-oriented behaviors and regulates anxiety and mood. In conclusion, ghrelin and its prohormone preproghrelin and other ghrelin-derived peptides are in my opinion interesting candidates for biomarkers for mood disorders like during long-term starvation and acute chronic hunger stress [24].
So, in comparison coming back to the central theme of this editorial: Do humans during starvation or an episode of hunger experience depression & anxiety? The following provoked statement from the utilitarian philosopher Jeremy Bentham (I warn it is shocking but it directly stipulates the core of our criteria of empathy). He states: “A full grown horse or a dog is beyond comparison a more rational, as well as a more conversible animal than an infant of a day, or a week or even a month old. But suppose they were otherwise, what would it avail? The question is not, can they reason? Can they talk? But also, can they suffer?” [25]. The reasons for this statement are implicit in the theory of consciousness [26] has developed. Suffering is not a matter of being visited by some ineffable but intrinsically awful state, but of having one life hopes, life plans, thwarting one’s intentions –whatever they are. It follows that the capacity to suffer is a function of the capacity to have articulated, wide-ranging, highly discriminative desires, expectations, and other mental states. According to this definition hunger and starvation are accompanied by depression and anxiety the higher the mental organization grade of the organism [26].
With respect to the topic biomarkers, at present an epidemiological registration system is applied in the developing countries which is atypical for specific risk regions in a country without any individual resilience. A credible method is needed for generating valid estimates for predicting the distribution of under-five deaths by cause in the developing countries [27].
Since the compelling and urgent research work of [27], with their “cry” for a vital under-five deaths prediction system situation has improved in 2012 and 2015 by sponsored work of the Bill & Melinda Gates Foundation. Information about the distribution of causes of and time trends for child mortality should be periodically updated. A team of researchers reported recently [28] the latest estimates of causes of child mortality in 2010 with time trends since 2000. Of ≈7,95 million deaths in children younger than 5 years in 2010, 64·0% (4,879 million) were attributable to infectious causes and 40·3% (3,072 million) occurred in neonates. Child survival strategies should direct resources toward the leading causes of child mortality, with attention focusing on infectious and neonatal causes [28]. More rapid decreases from 2010-15 will need accelerated reduction for the most common causes of death, notably pneumonia and preterm birth complications. Continued efforts to gather high-quality data and enhance estimation methods are essential for the improvement of future estimates. Recent work out of 2015 also funded by the Bill & Melinda Gates Foundation gave similar figures [29]. [29] estimated the distributions of causes of child mortality separately for neonates and children aged 1-59 months. To generate cause-specific mortality fractions, the researchers included new vital registration and verbal autopsy data. These mortality data of around 6-7 million “totters” < 5>
With this editorial I hope that this message “cry for help” will reach the general public via the scientific community. Man is originally from empathic - evidenced by "mirror neurons" research [34] - and the fact that we live in a divided Hunger-Obesity world has to do with the fact that we hardly realize what the image is of a starving dying child (or adult), such as seeing is in figure 1 in reality. One billion obese and nearly one billion acute hungry and everybody has the right for food (Millennium goal one). These are the facts. A simpler message cannot be given via the mass media [35,36].
Furthermore, it can be stated the mental health of individuals should be monitored by including mental health indicators in health information and reporting systems in regions of famine or in recovering regions. The indices should include both the numbers of individuals with mental disorders and the quality of their care, as well as some more general measures of the mental health of communities. Physically and mentally healthy and strong individuals determine the quality of life of communities through inter-social interactions (Figure 5).

Figure 5: An effective “personalized medical treatment” of the individual by e.g. mental-specific biomarkers for depression & anxiety will ultimately be beneficial for the whole society in this way reducing the costs of the National Health-Care System.
Monitoring at individual but also at community level (Figure 5) is necessary to assess the effectiveness of mental health prevention and treatment programs, and it also strengthens arguments for the provision of more resources. New indicators for the mental health of communities are necessary. Presently, scientists are beginning to unravel the intimate relationship between hunger hormones, emotions, stress and energy levels in the hope of developing a treatment for stress-related anxiety and depression caused by acute chronic hunger stress.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
