
E-Book | DOI: https://doi.org/10.31579/2692-9406/067
1 World Academy of Medical Sciences, Netherlands, Republic of Moldova.
2 State University of Medicine and Pharmacy "Nicolae Testemitanu" Republic of Moldova.
3 State Institute for Postgraduate Advanced Training of Doctors, Saint Petersburg, Russia.
4 Scientific Research Institute of Transplantology and Artificial Organs, Moscow, Russia.
5 Institute of Mother and Child of the Republic of Moldova.
*Corresponding Author: Ilie Vasiliev, MD, Academy Professor World Academy of Medical Sciences, Professor at the World Academy of Medical Sciences. First Superior Executor Vice- President of the World Academy of Medical Sciences. Chairman of the World Council of the Academy WAMS
Citation: V Ilie, V Maria, V Irina. (2021) Forty Years Success of No Maternal Mortality in Critical Obstetrics on the Operating Table. A decrease in the increased marker of tissue hypoxia pCO2> (AV-gap) in microcirculatory-mitochondrial distress syndrome in critical obstetrics is achieved by complex methods of recruiting microcirculatory-mitochondrial distress syndrome. Biomedical Research and Clinical Reviews. 4(1); DOI: 10.31579/2692-9406/067
Copyright: © 2021 Ilie Vasiliev, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 May 2021 | Accepted: 26 May 2021 | Published: 28 May 2021
Keywords: microcirculatory mitochondrial distress syndrome; microcirculatory - mitochondrial recruitment; acute multiple organ dysfunction syndromes; systemic perfusion pressure; pressure capillary resistance; vascular compliance; marker of tissue hypoxia pco2
Background
A retrospective analysis of the 40-year absence of maternal mortality in critical obstetric, in different countries, was due to the timely decentralization of macro-circulation through the recruitment of the microcirculatory-mitochondrial, in the space: capillaries - cell - mitochondria; detoxification; and adequate analgesia.
Recruitment of microcirculatory – mitochondrial reduces, microcirculatory-mitochondrial distress syndrome (MMDs) and syndrome of multi-organ dysfunction (MODs), by decentralizing macro-circulation, as a result, systemic perfusion pressure (SPP), is stabilized representing the difference between mean arterial pressure (MAP), and capillary resistance pressure, CRP, which adequately perfused the microcirculatory space of capillary ↔ cell ↔ mitochondria, thanks to adequate vascular compliance ∆VP with an accelerated speed of delivery and return of blood flow, which directly leads to a decrease in tissue hypoxia marker pCO2 (AV gap ) and, respectively, decrease MMDs, MODs and many other endogenous toxic substances. Optimization of SPP by RMM at MMDs, simultaneously reducing pCO 2 (AV gap), also reduces anion gap & urinary anion gap.
In cases of pulmonary/extrapulmonary damage with ↑ pCO2 and ↓ PaO2 / FiO2, ↓ 300 with the development of acute respiratory distress syndrome, ARDs, according to the 2012 Berlin Classification, MMDs are also aggravated at ↑ the pCO2 AV gap. With the development of mitochondrial collapse, MMP also needs additional support of multiple organ therapies - Multi-organ Supportive Therapy, MOST: 1) Alveolar recruitment with respiratory support in special modes of ventilation, mainly Airway Pressure Release Ventilation, APRV (P - high, T - high, P low, T - low), with permissive hypercapnia at normal pH, using inhaled pulmonary vasodilators; 2) RMM; 3) MOST - Extracorporeal life support organization - ELSO; 4) Modelling of the index of extravascular lung fluid, EVLWI; 5) Th4 - Th5 thoracic epidural block; 6) Active detoxification methods.
The absence of decreasing of the pCO2 tissue hypoxia marker at the pCO2 AV gap ↓ 5,0 mm Hg after RMM, rejects the necrosis/apoptosis, hypo- (an)-ergic cell and proves the mitochondrial euenergetic metabolic remodeling with the elimination of the hypo-(an)-ergic mitochondria performed by lysosomal clearance (mitophagy), argues stops membrane destruction, swelling of plasma, lysosomes, mitochondria, karyorrhexis, DNA destruction and karyolysis. Thus, demonstrating eu-ergic mitochondria with the normalization of mitochondrial Ca++ uniporter - channel and mitochondrial permeability pore transition, which productively inactivate the toxic forms of oxygen, Reactive oxygen species, ROS and Reactive nitrogen species, RNS.
Considering maternal mortality in state-of-the-art clinics and sophisticated methods of treatment and diagnosis, the human factor of the doctor and the available methods of treatment and diagnosis remained a priority in reducing and even eliminating obstetric mortality. The of success since the last century as in this century of which we described in this work, as in many other previously published works, and represented at international congresses in the Republic of Moldova, Romania, Spain, the Netherlands, Russia and others, where decrease in the increased marker of tissue hypoxia pCO2> (AV-gap) in microcirculatory-mitochondrial distress syndrome in critical obstetrics is achieved by complex methods of recruiting microcirculatory-mitochondrial distress syndrome, contributed to the absence of maternal mortality over 40 years of work in critical obstetrics is presented as a brilliant proof of an affordable model in any medical institution that finds itself next to a dying woman in labor.
Obstetric mortality was absent, for more than 40 years of emergency anaesthesiology and resuscitation in Moldova, Central Asia and Russia, and on-air ambulance, with critical [1-4] situations in obstetrics. Massive haemorrhagic shock; disseminated intravascular coagulation syndrome (DICs); syndrome [H](Haemolysis) [EL](Elevated liver enzymes) [LP](Low platelet count)], HELLP; eclampsia; rupture of cerebral aneurysm; coma; swelling (anasarca); systemic inflammatory response syndrome, SIRs; Compensatory Anti-inflammatory Response Syndrome, CARs; Persistent Inflammation, Immunosuppression, Catabolism Syndrome, PICs, septic shock; MODs; pulmonary embolism. For those times, it was especially heroic urgent caesarean in former medical rural health facilities under general anesthesia and respiratory support. Including with replacement of blood transfusions of new-borns during hyper-bilirubin group conflict, through the catheterized umbilical vein, otherwise jugular or subclavian. What was special was and the successful extraction of a live fetus of a pregnant woman with 3rd defects of cardiac valves in the mother - failure and stenosis: aortic, tricuspid and mitral.
Recruitment of microcirculatory – mitochondrial (RMM) had the goal of optimizing vascular volume pressure compliance (∆VP) of microcirculatory perfusion of space: capillary ↔ cell ↔ mitochondria, with accelerated venous return and elimination of CO2 and other endogenous toxic substances (ETS) with energy-resuscitation of mitochondrial collapse (MC) [5-7].
In shock cells, with the development of the syndrome Maria and Irina Vasilieva [13] mitochondria become targets, and in a vicious circle, the respiratory coefficient, the oxygen-glucose index as an indicator of energy metabolism, deteriorates even more. In mitochondria, the electric potential of which is ~ 180 mV, generating the electrochemical potential ΔμH +, is a necessary but insufficient condition for the synthesis of ATP, which, in turn, leads to destabilization of the mitochondrial membrane potential ΔΨm, which is lacking and regulates the generation of ROS / RNS by mitochondria. Intact channels Ca ++ - uniporter (a powerful regulator of mitochondrial bioenergetics), interrupt the automatism of irregular batmotropic networks P - myocardial pacemaker. Mitochondria and their energy come in as a non-invasive automatic mitochondrial switch and protect heart damage [8, 9]. MMD occurs due to the accumulation of pCO2> 6 mm Hg in the tissue space of the AV-gap. Which is considered a reliable marker of tissue hypoxia, provoked by a decrease in SPP, which increases with a low ejection fraction of the heart. Disorders of venous return and accumulation of cellular catabolites, further aggravating MK. In this case, the equilibrium is disturbed: iso-osmotic; - oncotic; - ionic; - electric; - tonic, - acid-base; as well as homeostasis - rheology, immuno - nutritional, energetic, with impaired microcirculatory compliance ∆VP and exacerbation of secondary ones → hypoxia - ischemia → acidosis → cell necrosis (destruction of membranes, swelling of plasma, lysosomes, mitochondria, karyorexis, DNA destruction, karyolysis). Programmed cell death (apoptosis) increases the effect on the mitochondrial potential of the Ca ++ - Uniporter channel, which opens the damaged pores of the transition of the mitochondrial permeable pore and loses the ability to inactivate ROS and RNS. RMM reduces not only oxidative stress, but also RNS, nitrohalogen stress. A decrease in ROS is carried out through the activation of the prooxidant/antioxidant ratio (GSH, ascorbate, retinols, tocopherols, urates, carotenes, bilirubin) and the ΔμH + mechanism [9] and the optimal use of O2 in the respiratory chain, thereby reducing ROS and O2. Thus, by activating the antioxidant system AS and the anti-nitrooxidant system ANOS, the balance between [ROS / AS] / [RNS / ANOS] is restored. The predominance of RNS> ANOS activates intracellular p53 protein synthesis, which induces the expression of apoptogenic proteins Bcl-2, Bax, Fas, p53AIP (Apoptosis - Inducing Protein). Along with the destruction of membrane proteins, DNA and RNA, lipid peroxidation (LPO) of cell membranes occurs. In such cases, necrosis> apoptosis is clearly exceeded, since the predominant system ROS> AS also reduces the transmembrane potential on the inner mitochondrial membrane, provoking Maria and Irina Vasilieva syndrome (electro-ionic membrane syndrome) [10-13], disrupting the opening/closing of the mitochondrial permeability transition, the pore-dependent Ca uniporter, the mPT pore [14-16], a conjugated process reflecting the homeostasis of the lysosomal clearance of mitochondrial autophagy (mitophagy). Microcirculatory-mitochondrial distress syndrome, MMD with an increase in pCO2 (AV gap)> 6 mm Hg is formed. Art., As a reliable marker of tissue hypoxia. Extreme / abnormal myelopoiesis exacerbates immunocompromised dissonance (IC) CHAOS - [C] ardiovascular Compromise: shock; [H] homeostasis; [A] poptosis; [O] rgan dysfunction; [S] suppression of the immune system, mediates MOD and causes extreme genomic, transcriptomic, proteomic, metabolic and phenomenal functional and structural disorders [8,9,17-24]
At the same time, the immune compromise contributes to the generalization of local infection, local inflammatory response syndrome, LIR through SIR - a cascade of proinflammatory cytokines (IL-1, 6, 8, TNF, IFNγ) or CAR cytokines (IL 4, 10, 13), the predominant provoking PIC [3,4, 17-19].
Materials and methods
Detoxification and adequate analgesia [3-7] enhance the strategic management of RMM to decentralize macro-circulation and restore blood flow in the microcirculatory - mitochondrial space to ensure cellular metabolism. Improving the delivery of oxygen and nutrients into the cell, and the elimination of CO2 and other catabolites from the cell, is carried out by RMM by stabilizing the vascular microcirculatory compliance ∆VP, maintained by the SPP (the norm is ~ 70 mm Hg), equal to the difference of the MAP ( ~ 90 mm Hg) – CRP (~ 20 mm Hg). MAP defines the monitor, and in its absence is determined according to the formulas. According to Maria Vasilieva study [25,26], a tear can be used as a diagnostic test for various diseases, and CRP in the practice of the doctor on duty can be compared with intraocular pressure, by the Kalmakov method, with the exception of oculist glaucoma, consultation of which is important and for examining the fundus in these patients.
Calculated examples: in patients with hypertension who have high blood pressure, BP, numbers, SPP will be higher and the extracellular fluid will shift in the intracellular space, and vice versa, with low blood pressure, the SPP ↓ 70 mmHg will decrease, and the liquid, on the contrary, will go from the extracellular sector to the vascular one. From which it follows that modifying vascular compliance ΔVP can also enhance detoxification. Successful RMM requires the comparison of the MAP with the locally-regional characteristics of the blood circulation by functional organs.
The constancy of ∆VP compliance of the brain is ensured, according to the Monroe Kelly doctrine, a balance between: cerebral blood flow, cerebrospinal fluid and mass of the brain. Cerebral perfusion pressure, not less than 100 mm Hg, designed to provide a metabolic rate in gray matter at 75 ml / 100 g / min, in white 30 ml / 100 g / min, and an average of 55 ml / 100 g / min. In situations of falling blood flow up to 25 ml / 100 g / min, there is a diffuse decrease in the electrical neural activity of the cerebral cortex. And when the blood flows: ~ 15 ml / 100 g / min., There is a slowdown/disappearance of the bioelectric nervous activity of the cerebral cortex; <10 ml / 100 g / min. irreversible, hypoxic and ischemic cerebral lesions are observed; stopped for 8-10 seconds - the consciousness is lost.
SPP modelling is possible due to manoeuvring: 1) cardiovascular compliance ∆VP: heart pump and BP; a) ino-vasoconstrictive effects to maintain the cardiac fraction with ↑ systolic BP, ↑ diastolic BP and ↑ total peripheral vascular resistance, TPVR, and b) ino-vasodilation - to maintain the cardiac fraction ↑ systolic BP, but with ↓ TPVR, thanks to vasodilation, with ↓diastolic BP; 2) effective circulating blood volume, ECBV [8,27] by means of volemic resuscitation; oncotic pressure; correction of anaemia; ; rheologic-resuscitation; equilibration of processes of coagulation - anticoagulation - fibrinolysis (thrombus mass, leukomas, fresh frozen plasma, rFVIIa, aprotinin, antithrombotic, thrombolytic, heparin, including with low molecular masses of 3000-9000); oncotic pressure (proteins, albumin); osmotic pressure; and colloid osmotic; pharmacological removal of excess fluid by sequestering, translocation and reduction of venous return - spinal / epidural block, blockade ganglion- N - nicotine receptor - ganglion blockers, diuretics; 3) CRP is modified by actions points 1 and 2 and pharmacological selective actions [ 28 ] at the α1-2, β1-2-3, γ-D1-5, ɑ, β, С, Dopamine adrenoreceptor levels - localized pre-, post-synaptic and ganglion- N - nicotine receptor - ganglion blockers. Nicotine-sensitive cholinergic receptors (N-cholinergic receptors) of autonomic nerve ganglia are blocked by ganglion blockers, as a result of which, blood pressure decreases, the flow of vasoconstrictive impulses to blood vessels decreases, and the peripheral vascular bed, primarily arterioles, expand. Modification by points 1,2 and 3 modulates the macrocirculation into microcirculation, where blood from the AV shunt - anastomosis is recruited directly into the paralyzed metabolic capillary, thus activating it, and to reduce the capillary leakage syndrome, where 5% albumin plays a special role.
Pharmacologically, taking into account M. Berenbaum, drug interactions (zero - additional; supraadititive — potentiation, synergism; infraaditive — mistakenly perceived as antagonistic), the function of the heart pump and blood vessels, blood pressure is modified: a) cardiac - inotropic; - chronotropic; - dromotropic; - bathmotropic and lusitropic; b) vascular support BP - with the help of vasoconstrictor and vasodilator agents. Reduce bradycardia and ↑ BP → β and - α - dopamine - dependent adrenomimetics, and with tachycardia and ↓ BP → α-vasopressors (norepinephrine), in which the adrenomimetics vasoconstrictive effect prevails ↑ BP and causes compensatory bradycardia. Are successfully used at NO-dependent hypotension and Moldovan preparations [29], derivatives of isothiourea, isoturon and difeture (raviten) with vasoconstrictive myotropic action, have a hypertensive effect by blocking nitroxide synthetase, an enzyme responsible for the synthesis of NO, endothelial relaxing factor. In bradycardia with a low cardiac output and high compensatory hypertension due to ↑ TPVR → Dobutamine is optimal with an inotropic β1-mimetic effect, which ↑ systolic BP, inotropic way, but due to simultaneous vasodilation, preload is optimized, which improves venous return, and reduces pulmonary hypertension, preventing pulmonary edema, as a result, post-load is also improved, creating an almost perfect SPP. Close to Dobutamine, there is Levosimendan is another ino-myo vasorelaxant, - (ino - cardio protector, vasodilator), but unlike Dobutamine, acts as a calcium desensitizer, by increasing the sensitivity of contractile proteins to existing Ca ++ ions, since Ca + + enters the cell through the mitochondrial Ca ++ - uniporter channel, and thereby increases the cardiac contraction force - inotropes, without increasing myocardial consumption in O2. As well for these purposes, cardio-inotropic effect is used, with vasodilation of pulmonary and peripheral arterial vessels, without ↑ heart rhythm, HR, but with ↓ post- and preload, phosphodiesterase IIIa inhibitors (ino-myo vasorelaxant), which are superior to combining the use of dobutamine with selective β-blockers (carvedilol). In the presence of a normal HR, hyper- and normovolemia (↑ECBV, ↑ BP) with an increased pre- and post-load, selectively justified themselves, nitrates and α-β-adreno blockers (Labetalol), which by establishing peripheral vasodilation with in arterioles and venules anti-hypertensive effects, have a beneficial effect on the cardiac output fraction and HR. In this direction proved that the combined use of α-vasopressor on the background of the N-cholinergic ganglion blockade, ganglion blockade without hypotension is established, at which a different pharmacological effect occurs, a new, not present in their isolated application, since post-capillary venules increase their susceptibility to the vasopressor and thereby support the macrocirculation, while decentralizing it, which optimizes vascular SPP ∆VP in which the microcirculation improves, mainly, increased susceptibility to adrenomimetic - pre, postsynaptic, etc, metabolic capillary sphincters, close the shunting through capillary anastomoses.
Optimization of SPP by RMM at MMDs, simultaneously reducing pCO 2 (AV gap), also reduces anion gap & urinary anion gap.
When optimizing SPP, besides autonomous brain pressure, and other loco-regional, for example, pressure and in the pulmonary perfusion system are taken into account, since an increased pressure in the left atrium causes pulmonary hypertension, due to a spasm of the pulmonary arteries resulting in a decrease in minute blood volume, MBV, Kitaev's reflex, as well as in response to an obstruction in non-ventilated lung areas, pressure in the pulmonary arteries also increases, at which reflex pulmonary hypertension occurs as described by in mechanism von Euler-Liljestrand. These cases are solved by RMM when optimizing vascular compliance ∆VP SPP and reducing pulmonary hypertension, at the level of CRP, by maintaining autonomous perfusion pressure (pulmonary artery wedge pressure ~ 12 mmHg), which is important for the ratio of ventilation and perfusion - VA / Q. The corresponding modification of vascular compliance ∆VP SPP extends and to autonomous abdominal pressure during abdominal compartment syndrome with simultaneous surgical correction.
With MODs, with an increase in ↑ pCO2, caused by pulmonary / extrapulmonary acute respiratory distress syndrome, ARDs [30-33] and confirmed by the fall in the oxygenation index ↓ PaO2 / FiO2 ↓ 300 in the context of the Berlin 2012 classification, violations of pathologies of gas exchange are also taken into account: 1) Lung gas exchange: a) acute respiratory failure - FetCO2 ↓, SaO2 ↓, PaO2 ↓, FiO2 ↓; b) parenchymal (endothelial-epithelial damage to alveolar and vascular tissue) - FetCO2 ↓ / or normal, SaO2 ↓, PaO2 ↓; 2) transportation of gas in the blood (minute volume) ↓, Hb ↓, SvO2 ↓, PvO2 ↓, avSO2, avPO2; 3) Gas exchange in tissues - SvO2 ↑, BE ↑, PvO2 ↑, avSO2 ↓, avPO2 ↓; lactate / pyruvate ↑.
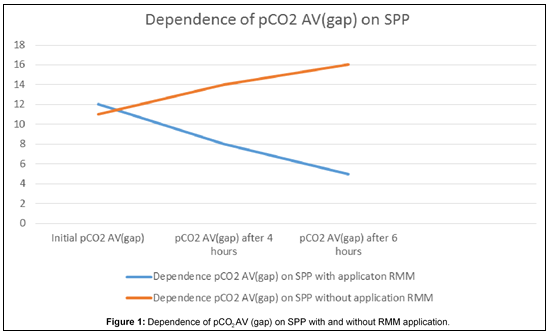
At the same time, the pressure / volume loop of the trachea is also considered, which are presented in 4 types (cucumber, pod, pear, tomato), which means that the more the loop surface is expanded, the more the respiratory pattern, as well as the definition of the dynamic ( Cdyn.) and statistical (Cst.) compliance confirming damage to the respiratory organs aggravating MC MMDs and RMM in such cases are supplemented with MOST therapy in the Extracorporeal Life Support Organization, ELSO with active detoxification methods: 1) Alveolar recruitment with respiratory support in special modes of ventilation, mainly APRV, with permissive hypercapnia at normal pH; 2) Recruitment of microcirculatory – mitochondrial, RMM, with support for optimal SPP. Figure 1.
3) MOST - Extracorporeal life support organization - ELSO: extracorporeal oxygenation - ECMO prototype and CO2 elimination by type ECCO2R [30]. 4) Active detoxification methods intra - and extracorporeal - electrochemical; ultraviolet (laser) photo modulation of auto blood; ultra-diafiltrating; continuous - intermittent filtering; haemodialysis; bio-immuno-activation and biodetoxification through the use of extracorporeal bio-xeno-perfusion (myelo-timo-spleen); enter sorption; volnersorption; plasma sorption; plasma exchange; lymph sorption; liquor sorption; peritoneal dialysis; oxygenation of the liver through the bougienage umbilical vein, hypothermia, and others, [31,34-38]; 5) Modelling of the index of extravascular pulmonary fluid, EVLWI [5,31,39]. Figure 2.
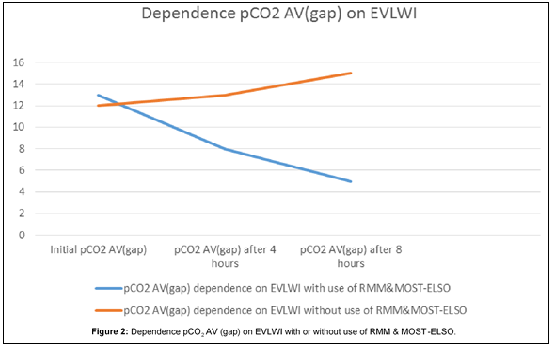
If EVLWI is <10 ml / kg, this indicates alveolar atelectasis, which requires volemic resuscitation, bronchoscopy, alveolar recruitment and surfactant therapy. In situations where EVLWI is> 10 ml /kg, is a threat to pulmonary edema, which requires a reduction in volemic resustation and the inclusion of diuretics, ultrafiltration and MOST - ELSO, inotropic therapy and invasive monitoring; 6) Th4 - Th5 thoracic epidural block. The level of catheterization of the epidural space should be Th4-Th5 (thoracic epidural block) in hyper-eukinetic patients, especially with hypertension and hypervolemia (EVLWI> 10 ml / kg), but without hypo coagulation coagulopathy. Epidural analgesia at the level of the chest is favourable because: it expands spastic coronary arterioles (cardio-coronary dilatation); increases the delivery of O2 to the myocardium; reduces myocardial oxygen consumption; reduces the risk of myocardial infarction and ischemia; improves lung function and contributes to the functioning of lung gas exchange; reduces pulmonary hypertension; accelerates intestinal motility; promotes bowel movement and conforms to the multimodal analgesia protocol. Permanent infusion of local anaesthetics (0.2% Ropivacaine / 0.125% Marcaine) in combination with opioid analgesics (fentanyl 2-4 μg / ml). After bolus 4 ml. follows, be a constant infusion of 5.0 - 7.0 ml / h according to clinical indications. The patient-controlled epidural anaesthesia is 0.2% Ropivacaine / 0.125% Marcaine in combination with opioid analgesics (Fentanyl 2-4 μg / ml). For one bolus of 4 ml of the mixture is followed by a constant infusion of 3.5-6.0 ml / h with a lockout interval of 20-30 minutes. The dose should be 1.0 to 2.0 ml, so the patient can enter it himself. In the case persistent of pain, a multimodal anaesthesia protocol follows. Paracetamol significantly increased the effect of analgesia, which could be compared with opioid analgesia or nonsteroidal anti-inflammatory drugs.
Thus, decentralization, anti-shock therapy, detoxification and analgesia in the RMM control strategy, supplemented by MOST-ELSO (ECMO and CO2 elimination ECCO2R, etc.) and in combination with antibacterial /antifungal [42] / antiviral treatment and surgical correction, counteracts the MMDs mitochondrial collapse, and regression MODs [2-5,40,41]. Respiratory [4-6,8,14,30,31,51,54], cardiac [8,16] and cerebral [55-64] support, has justified itself not only in critical-terminal obstetrics, but also in oncological MODs [ 43-48], with massive injuries and bleeding [49,50] and even with coronavirus infection SARS-Cov2 / COVID19 [9, 51-53,67], where Maria and Irina Vasilieva syndrome is significant [65,67].
1. The microcirculatory-mitochondrial distress syndrome is confirmed by the marker of tissue hypoxia, pCO2 AV-gap> 6 mm Hg, which increases with the destabilization of the systemic perfusion pressure, SPP, responsible for the macro circulation - microcirculation balance.
2. Recruitment of microcirculatory – mitochondrial, RMM, restoring systemic perfusion pressure, thereby decentralizes the macrocirculation and improves the microcirculatory space, at the level of the capillary ↔ cell ↔ mitochondria, in the metabolic space, and suspends the functioning of the direct anastomosis AV through the establishment of microcirculation through the metabolic capillary, thus remodeling the cell energy metabolism rate due to generating the electrochemical potential ΔμH + and of the mitochondrial membrane potential ΔΨm.
3. Recruitment of microcirculatory – mitochondrial drains into the macrocirculation accumulated in the microcirculatory space catabolites and endogenous toxic substances, with impaired venous return, creating translocation macro circulatory hipertoxemia, which argues the effectiveness of treatment of the microcirculatory-mitochondrial distress syndrome.
4. The absence of a continuous decrease in the pCO2 marker of tissue hypoxia AV gap <5 mmHg proves the suspension of the continuation of cell necrosis/apoptosis, hypo- (a) energy and confirms mitochondrial euenergetic metabolic remodeling with the elimination of mitochondrial hypo (an) energy, active lysosomal clearance (mitophagy), thus supporting the presence of euenergetic mitochondria with the normalization of mitochondrial Ca ++ - channel uniporter and cyclosporine-sensitive mitochondrial pore (mitochondrial permeability pore transition), with beneficial productively inactivate Reactive oxygen species, ROS and Active forms of nitrogen, RNS.
5. Systemic perfusion pressure can be modeled by modifying: a heart pump, effective circulating blood volume, and a capillary resistance pressure.
6. Reduction of the pCO2 A-V gap and suspending the development of the syndrome of multi-organ dysfunction is achieved by applying the recruitment of microcirculatory – mitochondrial in the complex associated Multi-organ Supportive Therapy - Extracorporeal life support organization (ECMO and CO2 elimination ECCO2R, etc.).
7. Optimization of systemic perfusion pressure by recruitment of microcirculatory – mitochondrial at microcirculatory-mitochondrial distress syndrome, simultaneously reducing pCO 2 (AV gap), also reduces anion gap & urinary anion gap.
8. The effectiveness of recruitment of microcirculatory – mitochondrial, as a strategic management, is also approved by a clinical examination of the patient: warming and restoring skin tone and turgor; regression of white spot syndrome with a slight pressure on the nail: stabilization of homeostasis.
9. The absence of decreasing of the pCO2 tissue hypoxia marker at the pCO2 AV gap ↓ 5,0 mm Hg after RMM, rejects the necrosis / apoptosis, hypo- (an)-ergic cell and proves the mitochondrial eu-energetic metabolic remodeling with the elimination of the hypo-(an)-ergic mitochondria performed by lysosomal clearance (mitophagy), argues stops membrane destruction, swelling of plasma, lysosomes, mitochondria, karyorrhexis, DNA destruction and karyolysis. Thus, demonstrating euergic mitochondria with the normalization of mitochondrial Ca++ uniporter - channel and mitochondrial permeability pore transition, a powerful regulator of mitochondrial bioenergetics simultaneously productively inactivates Reactive oxygen species, ROS and reactive nitrogen species, RNS.
10. The described respiratory, cardiac and cerebral support has justified itself in complex treatment anti-shock therapy, detoxification and analgesia in the RMM control strategy, supplemented by MOST-ELSO (ECMO and CO2 elimination ECCO2R, etc.) and in combination with antibacterial/antifungal/antiviral treatment and surgical correction, counteracts the MMDs mitochondrial collapse, and regression MODs, not only in critical-terminal obstetrics but also in oncological modifications, with massive injuries and bleeding and even with coronavirus infection SARS-Cov2 / COVID19 , where Maria and Irina Vasilieva syndrome is significant.
11. Despite the fact that we have not observed obstetric mortality due to the use of applying the recruitment of microcirculatory – mitochondrial associated Multi-organ Supportive Therapy - Extracorporeal life support organization for more than 40 years, with sufficiently multiple critical obstetric cases, we recognize that the ideal therapy for achieving regression of the microcirculatory-mitochondrial distress and of the syndrome of multi-organ dysfunction, with resuscitation of "no - fluid resuscitation "or" low - volume resuscitation "we are still very far away.
12. The studies presented on the clinical success of the absence of maternal mortality, forty years ago in critical - terminal obstetrics on the basis of fundamental biology, biochemistry, pathophysiology, pharmacology will be of interest to international congresses, including the 33rd World Congress on Pharmacology Conference.
This scientific material has been cumulated over 40 years retrospectively in the Republic of Moldova, the Russia, Middle Asia, including in sanitary aviation (Mobile Emergency, Reanimation and Download Service), as well as from all over the world. And was presented and published at the Obstetric Gynaecological Congresses in the Republic of Moldova, Romania, as well as a Global Summit on Medicine, Pharmacology & Cancer Research with WAMS in Barcelona (Spain) and in Amsterdam (Netherlands) at the International Conference on Biotechnology, Biomarkers & Systems Biology.
Thank, for supporting the scientific success of 40 years of absent maternal mortality in emergency critical obstetrics:
Gheorghe Ghidirim. Academician Professor of the Academy of Sciences of the Republic of Moldova, Former Minister of Health of the Republic of Moldova.
Professor Emil Ceban - Rector of the State University of Medicine and Pharmacy "Nicolae Testemitanu"
Victor Cojocaru, Gheorghe Paladi, Stanislav Groppa, Victor Gicavîi. Academicians Professors of the Academy of Sciences of the Republic of Moldova, State University of Medicine and Pharmacy "Nicolae Testemitanu" Republic of Moldova.
Stanislav Poliuhov, Vasile Grosu ( Republic of Moldova and Romania), Vladimir Cazacu, Nicolae Bacinschi, Eugen Diug, Anatolie Visnevschi ( Republic of Moldova and World Academy of Medical Sciences) , Olga Cernetchi, Sergiu Gladun, Valentin Friptu, Valentina Diug, Larisa Spinei (Republic of Moldova and World Academy of Medical Sciences), Elena and Pavel Globa. Professors of the State University of Medicine and Pharmacy "Nicolae Testemitanu" Republic of Moldova.
D'Ambra Mirta. Professor of the World Academy of Medical Sciences. Medicine University of Buenos Aires. Argentina.
Vladimir Vartanov. Professor of the World Academy of Medical Sciences. State Medical University of Samara. Russia.
Stavrou Ioannis. Professor of the World Academy of Medical Sciences. University Hospital Aretaieion, Athens Medical School, National and Kapodistrian University of Athens, Greece.
Oleg Tarabrin. Professor of the Odesa National Medicine University. Ukraine.
George Litarczek. Academician Professor of the Academy of Sciences of the Romania. Fundeni Institute Bucharest. Romania.
The distinguished G.Litarczek Patriarch of the scientific Anaesthesia - Therapy Care of Romania (born in Boston, USA), he died on 14 March 2019. Academician name G.Litarczek please circle in the mourning frame
Ilie Vasiliev. Tenaga National University, Kajang • REASERCH11.Our cientific publications was reflected found in Sciencegate https://www.sciencegate.app/keyword/776773 in Scientific Journals https://daten-quadrat.de/index.php?mod=3&nextp=18 at Simon Fraser University The PKP Index is an initiative of the Public Knowledge Project. https://index.pkp.sfu.ca/index.php/browse/index/4988 or Tenaga National University https://www.coursehero.com/file/83665824/SARS-COV-2COVID19InduceKawasaki-LikeDiseasepdf/.
Ilie Vasiliev. Tenaga National University, Kajang • REASERCH11. as well as the Harvard Library HOLLIS and many many more.
Professor MD Ilie Vasiliev thanks the US Embassy for the humanitarian assistance provided by artificial lung ventilators against COVID to the Republic of Moldova.























A great friend, associate and dedicated colleague, the Academy's top executive, Professor Vasiliev is a culminating champion of the World Academy of Medical Sciences (WAMS) whose virtue, vision and passion for work goes beyond measures. Having him as a true member of the WAMS Family, a genuine Brother, I am immensely proud of him and illimitably happy to be working with him sharing our dedication to continue together to fulfill our vision and duties for the good of the peoples of the World.
- M. M. Karindas, MD FWAMS
President, WAMS, the World Academy of Medical Sciences, Academy Professor of Oncology, Clinical and Molecular Oncologist.
Dr. Vasiliev is an incomparable eminence in medical science, having recognition by governmental, private, and academic organizations with international competence. Excelling in a diversity of disciplines, Dr. Vasiliev has demonstrated enormous passion for positive social impact in medicine and has engaged in innovative initiatives that accompany his vision of a brighter, safer future. It is my honor to take part in his endeavours to take medicine to new extended horizons.
- Alejandro De La Parra-Solomon
Co-Founder | Neuroscience - Mental Health - Education - Post COVID-19 solutions at Quantum Brain Research Institute | VPDS at Mass Media Division | Ambassador to Mexico at Give Nation
I think Ilie Vasiliev is a highly qualified specialist in his field. Punctual, pragmatic, purposeful, able to value his time, and - others. At the same time, he is an intelligent, tolerant, sympathetic person.
- Best regards, Andrey Gerasimenko - Kiev

Interview with Dr. Ilie Vasiliev, First Vice President - President of the World Academy of Medical Sciences.
Motto: "Medicine is science in the curable patient and art is in the incurable patient."
“My mentor in Romania is Academician Professor Dr. George Litarczek. Patriarch ATI (Intensive Care Anaesthesia) of Romania, born in Boston. " *
Dr. Ilie Vasiliev is a leading figure in medicine. He is one of those Romanian specialists from whom Dr. George Emil Palade, Dr. Constantin Dulcan and Dr. Nicolae Paulescu came.
Interview by Gabriel Gherasim
http://gabrielgherasim.com/index.html
Correspondence made by Gabriel Teodor Gherasim, from New York
The article was published in Romania, USA and Canada.
Correspondence made by Gabriel Teodor Gherasim, from New York
Romania
Independent National Weekly Journal
Health Patria Romana Editorial Office - September 6, 2020, Interview with Dr. Ilie Vasiliev.
USA
The US Journal "Romanian Journal".
USA Romanian - American Community Newspaper Romanian Journal pg 16 New York
Canada
Canadian Journal of the Observatory

Professional Biography
Professor MD, FWAMS, Ilie Vasiliev. Academy Professor of Medicine, the First Senior Vice-President of the World Academy of Medical Sciences. The Chairman of the General Council of the World Academy of Medical Sciences (World Medical Council). The Chairman of the WAMS National Council of Moldova, WAMS Coronavirus Safety Committee. The Fellow of the Academy, the Member of the WAMS Executive Council. The Member of the WAMS International Scientific Council. The Member of the WAMS Education and Training Board. Senior Executive Board Member of the World Academy of Medical Sciences. Senior Fellow of the World Academy of Medical Sciences, Senior Member of the Academy Faculty. Executive Senior Board Member of the WAMS. International Medical Research Council. Chief Executive Officer Research Port. Session Chair International Conference on Biotechnology, Biomarkers, Systems Biology, 2019. Amsterdam, with the presentation of the keynote information and the Global Summit on Medicine, Pharmacology, Cancer Research with WAMS Barcelona, Spain 2018, as well as many other relevant presentations of biomedical sciences at conferences in UE, Russia, Ukraine, Moldova, Romania, Central Asia and others.
Thank you very much! With special respect and best wishes! -Ilie Vasiliev
Professional Biography you can find in profile Ilie Vasiliev:
Whose transparency is available to ever.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
