
Review Article | DOI: https://doi.org/10.31579/2692-9759/006
1 Department of Cardiothoracic Surgery, Erasmus University Medical Centre, Rotterdam, the Netherlands
2 Department of Cardiology, Erasmus University Medical Centre, Rotterdam, the Netherlands
*Corresponding Author: Christiaan F.J. Antonides, Erasmus University Medical Centre Department of Cardiothoracic Surgery Dr. Molewaterplein 40, 3015GD, Rotterdam, the Netherla
Citation: Christiaan F.J. Antonides, Daniel J.F.M. Thuijs, Edris A.F. Mahtab1 Mattie J. Lenzen, A. Pieter Kappetein, (2020) A Critical Appraisal of a Decade of Left-Main Revascularization Meta-Analyses. J Cardiology Research and Reports 2(1): Doi: 10.31579/2692-9759/006
Copyright: © 2020, Christiaan F.J. Antonides, Daniel J.F.M. Thuijs. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 July 2020 | Accepted: 25 July 2020 | Published: 30 July 2020
Keywords: coronary artery bypass, percutaneous coronary intervention, left main, meta-analyses, MACCE, all-cause mortality
Background: Determining the optimal revascularization strategy for patients with left main coronary artery disease (LMCAD) is a compelling topic. After the publication of two new trials, numerous meta-analyses on percutaneous coronary intervention (PCI) versus coronary artery bypass grafting (CABG) appeared in the literature. This study set out to review the extent of published meta-analyses on PCI versus CABG in LMCAD, and stipulates the need for “quality over quantity”.
Methods: A systematic search in Embase, Medline Ovid and Cochrane databases was performed to identify meta-analyses on PCI versus CABG in LMCAD. Meta-analyses that reported associations between revascularization and clinical outcomes were included. Study outcomes were reported according to descriptive statistics, without pooling study outcomes.
Results: Fifty-one meta-analyses were included. Of those, 33 became available after EXCEL and NOBLE trial publication. The composite of major adverse cardiac (and cerebrovascular) events were reported in 41, and 49 reported all-cause mortality. Results varied among meta-analyses, depending on (i) randomized versus observational data, or a combination of both, (ii) methodology and effect-measures to report treatment-differences, (iii) varying sample sizes, and (iv) the year of publication.
Conclusions: The number of meta-analyses on PCI versus CABG in patients with LMCAD, is disproportionate and urges the need for quality over quantity. To ensure future high-quality publications, we call on all authors, editors and reviewers to appraise the evidence already available and join forces to conduct individual patient data pooled analyses instead.
Meta-analyses are systematic reviews that pool study-outcomes to increase statistical power and provide a higher level of evidence than is often possible with single studies. Therefore, meta-analyses are frequently consulted by healthcare professionals and inform medical guidelines [1].
The number of meta-analyses increased substantially in the field of cardiovascular medicine and determining the optimal strategy for patients with left main coronary artery disease (LMCAD) remains a fiercely debated subject. Over the past decades, numerous randomized studies assessed clinical outcomes after percutaneous coronary intervention (PCI) versus coronary artery bypass grafting (CABG) in patients with LMCAD.2-6 Two randomized controlled trials (RCTs) that contributed considerably to the evidence are the EXCEL (Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization) and NOBLE (Nordic Baltic British left main revascularization) trials [7,8]. Additionally, several non-randomized observational studies have reported results of CABG versus PCI. Pooling of observational data with randomized studies may lead to inter-study variability related to study design, sample size, baseline characteristics and outcomes, making it challenging to adequately appraise all scientific evidence available.
A meta-analysis, if performed correctly, can be helpful. However, an excess of meta-analyses, as was noticed over the recent decade, could lead to overlapping and redundant outcomes [9]. Therefore, this study critically appraised the extent of potential overlap and shortcomings by systematically reviewing the contemporaneous published meta-analyses on PCI versus CABG in LMCAD, with a special focus on those published after the EXCEL and NOBLE publications.
Search strategy. On November 7th, 2018, a systematic literature search, according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guideline [10]. (Supplementary Appendix), was performed in Embase, Medline Ovid and Cochrane databases to identify meta-analyses on PCI versus CABG in LMCAD. The search contained the following key words or synonyms: “left main coronary artery disease”, “percutaneous coronary intervention”, “coronary artery bypass grafting” and “meta-analysis”. A detailed search strategy is reported in the Supplementary Appendix.
Meta-analyses comparing revascularization strategies for LMCAD, by PCI with any stent(s) versus CABG, and reported clinical outcomes were included. Titles and abstracts were first screened for inclusion. When eligible, full-text English articles were subsequently reviewed independently by two authors (CA and DT). Predefined exclusion criteria were: (i) conference abstracts, (ii) absence of a LMCAD population, (iii) subgroups of patients with LMCAD, (iv) absence of effect estimates, (vi) individual patient pooled analyses or (vii) systematic reviews. Incongruities were resolved by agreement between two authors (CA and DT).
Data extraction. The following study details were extracted: year of publication, authors, journal, number of patients (total, CABG, and PCI) and the number of included individual randomized controlled trials (RCTs) and observational studies. Postoperative outcomes with an effect estimate (hazard, odds, risk ratios or incidence rate ratios) were extracted, along with the model used for analysis (fixed or random effects model). “Combined long-term follow-up” is defined as meta-analyses reporting a pooled event-rate at follow-up with varying durations (e.g. combination of 1, 3 and 5-year follow-up data).
Clinical outcomes that were extracted included major adverse cardiac (and cerebrovascular) events (MAC(C)E), according to the definitions used by the individual included meta-analyses, such as (i) death, stroke or myocardial infarction (MI) or as (ii) death, stroke, MI or any form of repeat revascularization (for example; target-vessel revascularization or ischemia-driven revascularization). All-cause mortality rates were also extracted.
Study outcomes. The primary endpoint consisted of a summary of MAC(C)E and all-cause mortality outcomes at combined long-term follow-up reported by meta-analyses published after EXCEL and NOBLE. Additionally, a summary of MAC(C)E and all-cause mortality outcomes at 1-year and combined long-term follow-up was provided for all included meta-analyses. The present report had no intention to determine which revascularization strategy would be preferable for patients with LMCAD and rather focused on providing an overview of the currently available literature. Therefore, pooled outcomes of treatment effects are not provided.
Statistical analyses. Results are reported according to descriptive methods. All risk estimates reported, reflect a “PCI versus CABG” comparison. When an included meta-analysis reported “CABG versus PCI” risk estimates, these were recalculated to represent “PCI versus CABG” comparisons. Forest plots were used to visualize the spread of varying study outcomes for MAC(C)E and all-cause mortality. Plots were constructed with Prism 8 (GraphPad Software, San Diego, CA, USA).
Study selection. The systematic search resulted in 402 articles. After excluding duplicates, screening titles and abstracts, 128 articles remained for full text reading (Figure 1).
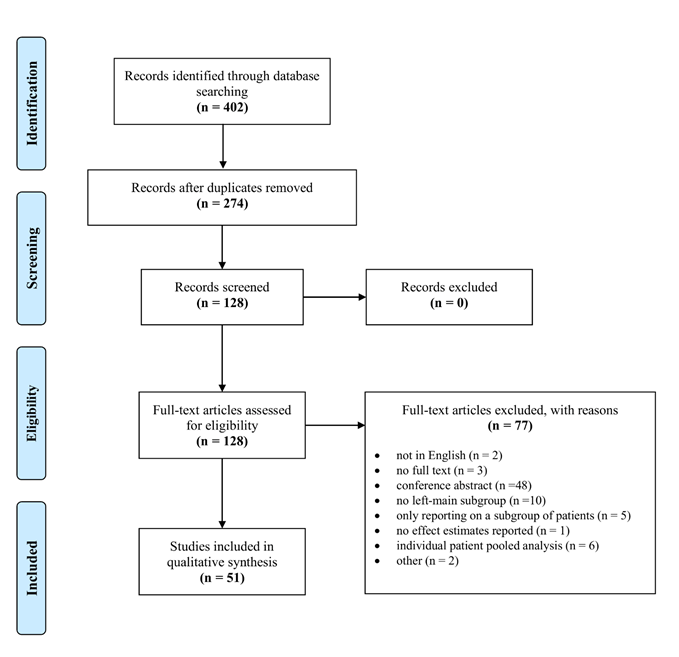
Abbreviations used: CABG; coronary artery bypass grafting, PCI; percutaneous coronary intervention, LMCAD: left main coronary artery disease.Of these, 77 were excluded based on the pre-specified criteria. Finally, 51 meta-analyses were included in the present study, of which 33 were published after EXCEL and NOBLE (Table 1 and Supplementary Appendix Table S1) [11.61].
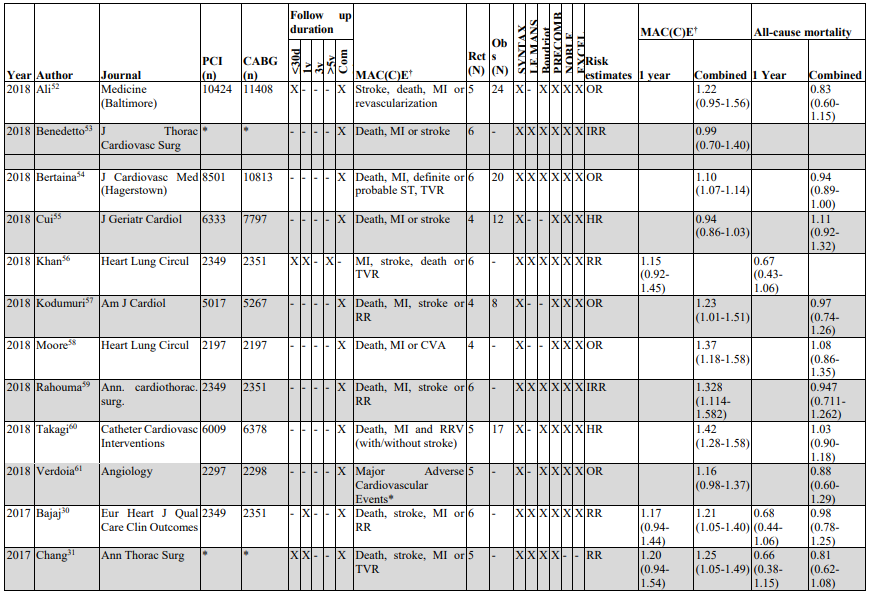

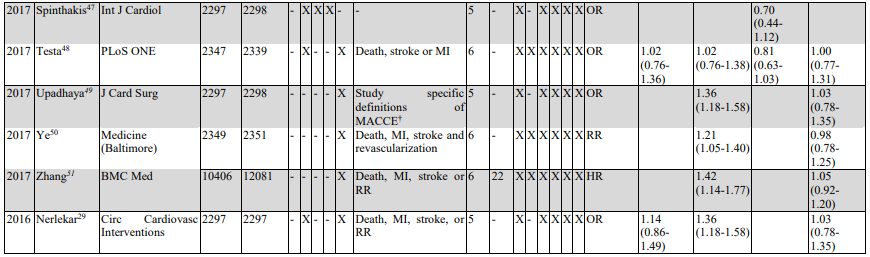
Risk estimates representing CABG versus PCI, provided by included meta-analyses, were recalculated to represent PCI versus CABG risk estimates. X = YES , - = NO. *this specific outcome was not specified in this meta-analysis. †MAC(C)E was defined according to the study-specific definition used by the included meta-analysis. #the correct reference was missing in the original meta-analysis.
Abbreviations used: CABG: coronary artery bypass grafting, CVA: cerebrovascular accident, PCI: percutaneous coronary intervention, LMCAD: left main coronary artery disease, RCTs: randomized controlled trials, Obs.: Observational, Ref.: reference, LA: longest available follow-up, MI; myocardial revascularization, RR/RRV; repeat revascularization, TVR: target vessel revascularization, ST; stent thrombosis, OR: odds ratio, HR: hazard ratio, RR: risk ratio, IRR: incidence rate ratio, UR: unplanned revascularization.
Published meta-analyses. The number of published meta-analyses increased over the past decade, especially after the publication of the randomized EXCEL and NOBLE trials (Figure 2) [7, 8].
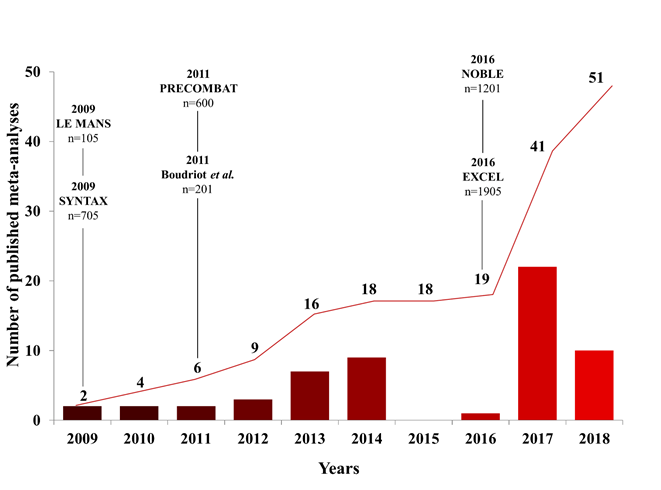
The red bars represent the amount of published meta-analyses per year. The red curve represents the cumulative amount of published meta-analyses over the past decade. The main randomized studies that published data on PCI versus CABG in LMCAD are indicated by black lines and names with the intention-to-treat sample sizes.
Several journals published more than one meta-analysis, with one journal publishing 10 meta-analyses on PCI versus CABG for LMCAD. Meta-analyses predominantly reported risk estimates according to odds, risk or hazard ratios.
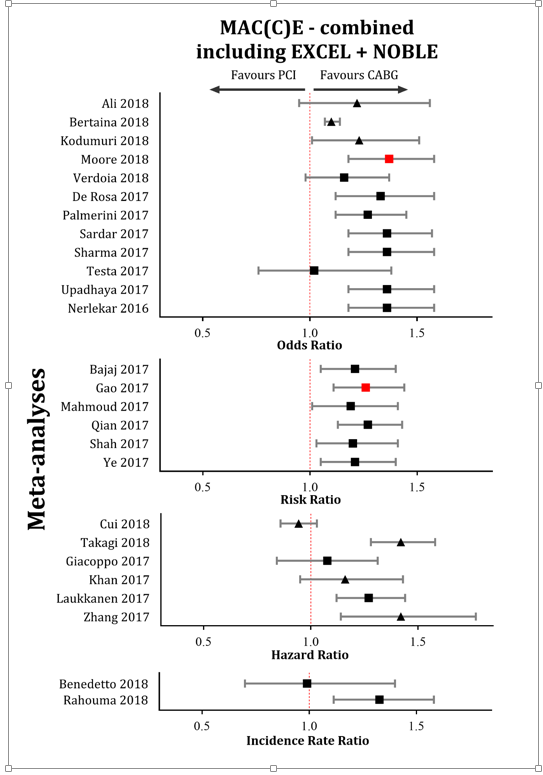
Meta-analyses after EXCEL and NOBLE. Thirty-three meta-analyses were published after EXCEL and NOBLE. Of these, 32 included EXCEL and NOBLE in addition to results from 3 or 4 other RCTs in their analysis. MAC(C) E outcomes, at combined long-term follow-up, were reported by 26 studies (Table 1, Figure 3),
Risk estimates represent PCI versus CABG comparisons and were categorized according to: odds, risk, hazard and incidence rate ratios. MAC(C) E was defined according to the study-specific definition used by the included meta-analysis. Legend of shapes used: square: only randomized controlled trials, triangle: randomized controlled trials plus observational studies. Size of a shape does not represent the study sample size nor the weight of a specific study. Black represents random-effect meta-analyses, red fixed-effect meta-analyses. Abbreviations used: CABG; coronary artery bypass grafting, PCI; percutaneous coronary intervention.
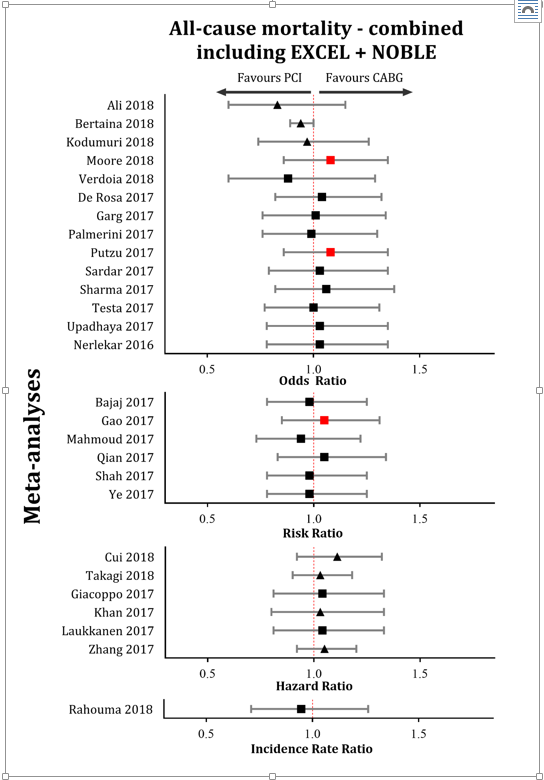
While 27 meta-analyses reported all-cause mortality at combined long-term follow-up (Table 1, Figure 4).
Risk estimates represent PCI versus CABG comparisons and were categorized according to: odds, risk, hazard and incidence rate ratios. Legend of shapes used: square: only randomized controlled trials, triangle: randomized controlled trials plus observational studies. Size of a shape does not represent the study sample size nor the weight of a specific study. Black represents random-effect meta-analyses, red fixed-effect meta-analyses. Abbreviations used: CABG; coronary artery bypass grafting, PCI; percutaneous coronary intervention.
Meta-analyses that included the same RCTs (SYNTAX, Boudriot et al., PRECOMBAT, EXCEL, NOBLE with/without LE MANS) reported varying sample sizes, ranging from 4594 to 4700 patients, while the overall intention-to-treat population consists of 4595 patients (5 RCTs) and 4700 (5 RCTs plus LE MANS, respectively) (Table 1).
Eleven meta-analyses reported MAC(C)E risk estimates at combined long-term follow-up varying from 0.99 (95%CI: 0.70-1.40) to 1.36 (95%CI: 1.18-1.58), although the composite of MAC(C)E differed among trials. MAC(C)E-specific definitions used by the various trials are reported in the Supplementary Appendix (Table S2). Ten meta-analyses reported risk estimates of all-cause mortality at combined long-term follow-up, varying from 0.94 (95%CI: 0.73-1.22) to 1.06 (95%CI:0.82-1.38). Two meta-analyses that also included observational data reported similar outcomes as compared studies only including RCTs [51, 54].
Published meta-analyses over the past decade. Since 2009, 41 meta-analyses reported MAC(C)E outcomes (Table S1). Of those, 33 reported outcomes at combined long-term follow-up (Figure S1) and 22 reported outcomes at 1-year (Table 1, Figure S2). All-cause mortality, at combined long-term follow-up, was reported by 38 meta-analyses (Table S1, Figure S3). Twenty-seven studies reported all-cause mortality at 1-year (Figure S4). Meta-analyses that only included RCTs reported similar all-cause death outcomes compared with those including also observational data.
Fifty-one meta-analyses covering the exact same topic were identified, and of these, 33 emerged over the past three years after the publications of the randomized EXCEL and NOBLE trials. Sixteen meta-analyses were published from 2009 to 2013 and this number more than doubled (n=35) from 2014 to 2018. While this study did not perform a meta-analysis of meta-analyses and had no intention on determining the preferred revascularization strategy for LMCAD, it systematically reviewed the abundancy of meta-analyses on PCI versus CABG in LMCAD over the past decade. Interestingly, the reported outcomes differed between meta-analyses due to several methodological reasons. Although meta-analyses (should) aim to present the highest level of evidence, there are multiple shortcomings which are summarized below [9, 61, and 62].
There were methodological limitations in the design of many meta-analyses. The reported sample-sizes varied without explanation. Several studies combined the intention-to-treat populations with as-treated populations. Many (n=38) meta-analyses report all-cause mortality at long-term follow-up, while the duration of follow-up differed significantly between trials. The SYNTAX trial for instance, reported 5-year follow-up, while EXCEL reported 3-year follow-up. Inclusion of studies with different follow-up durations could result in an under- or overestimation of the outcome, as it is well known that risk differences of MI and repeat revascularization diverge over time, favoring CABG.2,7,8,64,65 This is most evident in the landmark analysis of the EXCEL trial for the composite endpoint of death, stroke or MI: 0-30 days (HR: 0.61 (95% CI: 0.42-0.88)) versus >30 days -3 year (HR: 1.44 (95% CI: 1.06-1.96)). [7, 66].
Additionally, the statistical models used in the meta-analyses differed. Besides reporting various effect-measures, meta-analyses either used a random-effect or a fixed-effect model. A fixed-effect model assumes that the treatment-effect is similar across studies, while a random-effect model accounts for differences in treatment effect, study populations or follow-up length [67]. Some of the meta-analyses that included SYNTAX, Boudriot et al., PRECOMBAT, EXCEL and NOBLE used a random-effect model while others used a fixed-effect model. Moreover, meta-analyses that included observational studies, with substantial variations in follow-up time and patients baseline characteristics, used a fixed-effect model.
Finally, composite outcomes with different definitions were pooled. The definitions of MAC(C)E differed among SYNTAX [65], EXCEL [7], and NOBLE (Table S2) [8], but some meta-analyses did not take into account these differences in the composite end-points. This, however, is crucial information for both patient and physicians when deciding on the preferred treatment.
To diminish the overlap in future meta-analyses, it is recommended to register the rationale and protocol of a new meta-analysis at an online registration platform [68]. Finally, a preferable alternative for performing a meta-analysis is to conduct an individual patient data pooled analysis [69, 70]. Pooling individual patient data overcomes the different methods of reporting and analyzing data by individual studies. It has the advantage to use all available raw patients’ characteristics, account for missing variables, use accurate follow-up data and a standardized statistical method for analysis [69].
The present study identified 51 meta-analyses covering the exact same topic of PCI versus CABG revascularization in patients with LMCAD. With the publications of longer-term follow-up of the SYNTAX and EXCEL trials, one could anticipate another surge of meta-analyses. To ensure high quality studies and reduce overlapping publications, we call on all authors, editors and reviewers to critically appraise the evidence already available and use online meta-analyses registration platforms to avoid potential overlap. Collaborating and focusing research capacities, by conducting individual patient data pooled analyses could enable us to work more efficiently and ensure reporting the highest quality of available evidence.
We would like to thank Wichor M. Bramer; Biomedical Information Specialist, Medical Library, Erasmus University Medical Centre, Rotterdam, The Netherlands, for his expertise in constructing the comprehensive systematic search.
Dr. Kappetein and dr. Head report to work as employees of Medtronic, outside the submitted work. All other authors declare no competing interests relevant to this publication.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
