
Research Article | DOI: https://doi.org/10.31579/2692-9406/038
*Corresponding Author: Joseph M Bodi, Department of pediatrics, Kinshasa University Hospital, School of medicine, Kinshasa University.
Citation: Bodi JM, Makulo JRR, Monkoti MM, Aketi LP, Matula IK. (2021) A Congolese infant of 4 months and 8 days presenting a severe form of Covid-19. Biomedical Research and Clinical Reviews. 3(4); DOI: 10.31579/2692-9406/038
Copyright: © 2021 Joseph M Bodi, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 December 2020 | Accepted: 29 January 2021 | Published: 23 March 2021
Keywords: Covid 19; severe form; infant; sub-Saharan Africa; DR Congo
To date, only a few rare cases of severe forms of Covid-19 in children, especially infant, have been described in other parts of the world. So far no case reported in sub-Saharan Africa (SSA). We report the case in the Democratic Republic of Congo of an infant of 4 months and 8 days old, who presented after malaria disease, a picture of bronchopneumonia with severe respiratory failure (Pa O2 :49 mmHg). The RT-PCR made it possible to diagnose a Covid-19 of severe form. The infant had probably been infected by his mother and had no other co-morbidities that could induce a decrease in immunity. The CT scan injuries were comparable to those described in adults. Under oxygen, anticoagulation, hydroxychloroquine and Azythromycin, the outcome was good. Pediatricians in SSA countries should be careful and not miss cases of COVID19 in infant population with severe respiratory syndrome usually observed in most of lung infectious disease.
Several data around the world show that the effects of the new pandemic of COVID-19 are less of a concern in children, who seem to be asymptomatic or to develop mild illness [1-3]. The reasons justifying this relative protection of children are not fully understood. However, most studies suggest that in rare severe forms of Covid-19 in children, the same risk factors in adults are evoked to children, including comorbidities such as cardiac pathology, diabetes, chronic pulmonary disease, HIV and drug-induced immunosuppression [4]. In sub-Saharan Africa (SAA), children constitute a greater proportion of the population and may be more vulnerable for several other reasons as the prevailing malnutrition, HIV, tuberculosis which contribute to the occurrence of severe respiratory tract infection [5, 6]. In addition, the other risks are linked to the meager resources allocated to the health sector, the priority that families sometimes give to adult with health problems and low vaccines coverage which exposes SSA children to several diseases that can reduce their immunity [7-9].
To our knowledge, no severe form of Covid-19 in children has been described in Central Africa. Until now, rare cases of severe covid-19 in children living in SSA have been described, especially in South Africa [10, 11]. In general, these children had progressed well despite a sometimes serious clinical picture. This clinical case concerns an infant of 4 months and 8 days, who presented a severe form of Covid-19. Apart from malaria and anemia, no other co-morbidity was associated. The importance is to attract the attention of pediatricians so as not to overlook such cases despite their rarity. The CT images as well as the management strategy are also discussed. The requirement for informed consent was obtained from the patient's parents.
A 4-month and 8 days -old male infant admitted on 4th August 2020 with a severe distress respiratory. He was transferred from a private hospital. The story of the disease started by fever, dyspnea and cries 9 days before. He received tea and orange juice because parents suspected abdominal pain also because of cries. His condition was not improved after receiving these drugs from family members at home. He was admitted at a private hospital where he was treated with gentamicin, amoxicillin, vitamin C, Argyrol nose drops and received also blood transfusion because hematocrit was low (21%). The private hospital transferred the infant at University hospital because no improvement was observed. At admission, respiratory rate was high (60 cycles/minute) with tachycardia at 166/minute. The weight was 5Kg which was normal for the age and the birth weight was 2800grammes. The lung auscultation reported under crakes in the two lungs. Oto-Rhino-Laryngology exam was normal. After all the physical exam, the pediatric team suspected a severe Bronchopneumonia. Because of local COVID 19 score (table 1) with the value of 4/26 (fever: 2 and distress syndrome: 2), COVID 19 was suspected also. The diagnosis was confirmed by Reverse Transcriptase Polymerase Chain Reaction (RT-PCR). So, the children has been admitted at the Covid treatment center. COVID 19 IgM and IgG antibodies were nor performed.
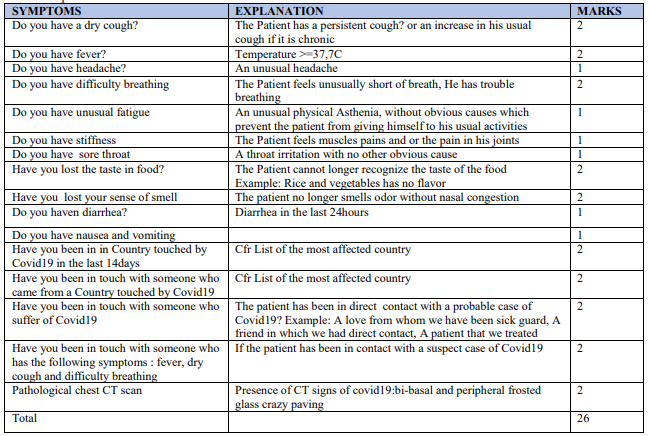
If the triage score is low, clinical suspicion of covid19 infection is retained
Conclusion:
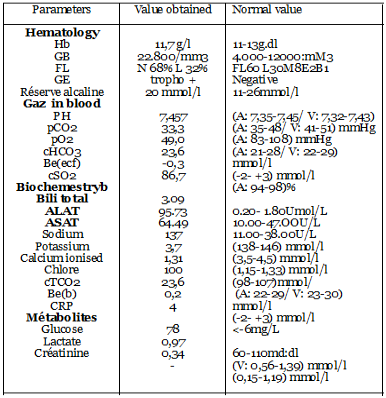
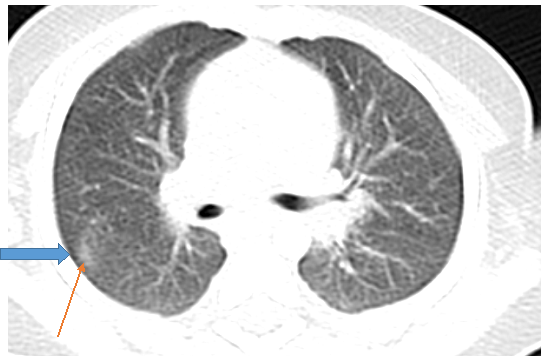
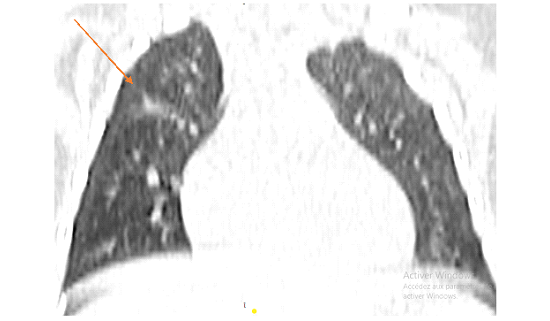
Laboratory tests showed an elevated white blood cell (WBC: 22.800/mm3) count and neutrophil count (68%), low C-reactive protein (CRP: 4mg/L), and elevated total and direct bilirubin (respectively 3.09 and 2.44umpl/L). Alanine aminotransferase (ALAT), and aspartate amino transaminase (ASAT) were elevated (95.3 and 64.46 U/L In addition, Blood gaz showed low Pao2 (Table 2). The chest CT showed pure Ground Glass Opacities (GGOs), located under pleural at posterior segment VI of upper right lobe (Fig1 and fig3) and hilar bilateral patches along with Broncho vascular bundles (Fig2).The test for the mother was positive for COVID 19 without any manifestations

Diagnosis: We concluded to: SARS –Cov-2 in infant 4 months and 8 days, sepsis with pneumopathy origin and malaria with hemolytic anemia.
The infant was treated according to the national policy of COVID 19 treatment in Democratic Republic of Congo with Azithromycin (10mg/Kg once per day for 5 days), chloroquine (10mg/Kg once per day for 5 days) Lovenox (0.025cc, twice per day for 7 days), Vitamin C ( 5ml, twice per day for 7 days) and Zinc (2.5ml twice per days for 7 days. Malaria was treated with quinine (5 drops, three time per day for 7 days: 3X10mg /kg of Quinine per day for 7 days). He received intermittent oxygen using extractor 5 liter/minute for 3 days. The child was treated during 8 days at Kinshasa University Hospital CTC and was discharged on 17 August 2020
This rare case in the context of Covid-19 is very illustrative. The initial table evokes malaria, but thanks to the attention of pediatricians (based on the warning signs), the in-depth examinations have made it possible to diagnose Covid-19.
Basically, children have often milder disease than adults. In COVID-19 children, severity is classified as mild (asymptomatic or subclinical), normal, severe, and critical [12]. Mostly in children, cases are mild or normal severity and case fatality rate is very low. In children, the milder course of the disease results to their immature immune system, which does not overreact to the virus, but the reasons why disease tends to be less severe in children requires more researches for best evidence.
It is observed and reported that children usually have, atypical, mild and asymptomatic disease with only fever (50%) and cough (38%) which are the main presenting complaints [9]. Two other children admitted in our CTC had no symptoms. They were just tested positive after family screening because parents were COVID 19 positive. Our patient presented fever and severe distress syndrome using oxygen treatment for the management of the case. According to the severity of the diseases in children, studies [13] found that children may develop also severe disease and lead to worse outcome, especially when diagnosis is delayed because of atypical presentations at the beginning of the disease. Our patient, finally developed severe clinical features with severe distress. So far, many questions remain without response, especially the reason which can explain the severity of the disease in our infant. Association with malaria could explain the severity of the disease? The first pediatrics severe case was reported in Wuhan. He was 13-month-old boy without previous comorbidity and he developed shock, acute respiratory distress, and renal failure [14]. Fortunately, our child did not develop shock and renal failure. Risk factors for severe disease in children are not well understood because no more cases are reported. Laboratories figures can be different compared to adults [15].In our case, whole White Blood Cells and neutrophil were increased but CRP was decreased. ALAT and ASAT were elevated
It is necessary to thing to other infectious diseases of the lungs in case of atypical features at chest CT for differential diagnosis, including bronchopneumonia, mycoplasma pneumonia, and seasonal influenza. CT scan, basically in adults found that injuries could involve all lobes. Injuries in the upper lobes are more severe and there are 4 categories of CT findings described in adults:(a) Pure Ground-Glass Opacities (GGOs), (b) pure consolidation, (c) both GGOs and consolidation; and(d) small nodules and patches along with Broncho vascular bundles, similar to bronchopneumonia [10]. The chest CT scan of the infant found Pure Ground-Glass Opacities (GGOs) under pleural at posterior segment of upper lobe of right lung and patches along with Broncho vascular bundles at the 2 hiles. These images observed in our children can explain the severity of the disease.
Mostly in children, the CT features are different compared to adults [11].The GGOs are regularly present in adult. The distribution of injuries is located frequently in the peripheral and posterior areas of both lungs [12].
The infant was treated according to the national policy of COVID 19 treatment .This protocol was approved by the concertation between University and the technic secretariat of COVID19 riposte. Corticoids were not given to our patient because not included in our protocol in that moment. The evolution were very good with this protocol and the infant was discharged after 8 days of treatment.
In conclusion, severe cases of SARS-COV-2 exist in pediatrics population. Pediatricians should be aware to check children with severe distress. By this way, we can diagnose early and treat correctly children infected by Coronavirus.
Competing interest
The authors declare that they have no competing interests.
Authors’ contributions
BJM, MJRR, MIK, MMM, ALP, MFM and LVV conceived, designed, deployed and wrote directed the case report study MJK, NBM, OGO, MNM received the patient sat the Centre of Covid Treatment and treated the infant.
LMT and TFT performed the CT scan exam.
Acknowledgments
The authors thank NGO ALIMA for the support received about the treatment of patients with VOVID19. They thanks INRB for the logistics support.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
