
Review Article | DOI: https://doi.org/10.31579/2692-9392/164
1 Midwifery department, Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences, Iran
2 Director of the Division of Medical Genetics and Molecular Optogenetic Research.
3 Division of Medical Genetics and Molecular Pathology Research, Harvard University, Boston Children's Hospital.
4 Medical Genetics-Harvard University.
*Corresponding Author: Shahin Asadi, Medical Genetics-Harvard University.
Citation: Maryam Mountazeri, Amir Shokri, Mohadeseh Zoughi, Narjes Arshia and Shahin Asadi, (2023) A Comprehensive and Clinical Review of Distal Deletion Syndrome of Chromosome 5q14.3. Archives of Medical Case Reports and Case Study, 7(1); DOI:10.31579/2692-9392/164
Copyright: © 2023, Shahin Asadi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 December 2022 | Accepted: 06 January 2023 | Published: 20 January 2023
Keywords: distal chromosome 5q14.3 deletion syndrome; chromosomal disorders; child syndromes
Cardozo et al. (2009) reported 3 unrelated children, 2 boys and 1 girl, with severe mental retardation, epilepsy, and bilateral periventricular heterotopia limited to the subcutaneous region of the temporal bones and occipital lateral ventricles. Other features of this syndrome include hypotonia, delayed motor development, lack of speech, and minor facial deformities such as prominent forehead, depressed nasal bridge, and high blood pressure
Clinical Signs and Symptoms of Distal Chromosome 5q14.3 Deletion Syndrome
Cardozo et al. (2009) reported 3 unrelated children, 2 boys and 1 girl, with severe mental retardation, epilepsy, and bilateral periventricular heterotopia limited to the subcutaneous region of the temporal bones and occipital lateral ventricles. Other features of this syndrome include hypotonia, delayed motor development, lack of speech, and minor facial deformities such as prominent forehead, depressed nasal bridge, and high blood pressure. Also, one of the patients showed polymicrogyria in brain MRI [1].

Figure 1: Illustration of children with distal deletion syndrome of chromosome 5q14.3 with distinctive facial features [1].
Etiology and Discussion of Distal Deletion Syndrome of Chromosome 5q14.3
Using array CGH, Cardoso et al (2009) identified a deletion of chromosome 5q14.3q21 in 3 unrelated patients with periventricular heterotopia. These deletions ranged in size from 6.3 to 17 Mb and included a common region of 5.8 Mb. Computational critical region analysis identified 14 candidate genes [1,2].
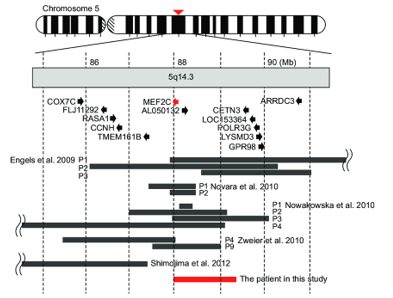
Figure 2: Schematic of the distal deletion mutation of chromosome 5q14.3 [1].
Sobreira et al (2009) identified a 7.4 Mb deletion of chromosome 5 at 5q14.3-q21 in an 11-year-old boy with mental retardation, bilateral iris coloboma, hearing loss, dental malformation, and facial deformity. features, but without periventricular heterotopia, which Sobreira et al. (2009) referred to the report by Cardoso et al., who identified a deletion region in the overlapping region of 5q14 in patients with periventricular heterotopia. One of these patients had a unilateral coloboma and shared part of the deletion with the patient reported by Sobreira et al. Comparison of the shared deletion regions between the 2 patients revealed a 2.6 Mbp putative region for coloboma and a 1.84 Mbp putative region for periventricular heterotopia [1,3].

Figure 3: Another view of a child with distal chromosome 5q14.3 deletion syndrome [1].
Le Meur et al (2010) reported 5 unrelated children with severe mental retardation, absent speech and stereotyped movements, each with deletions between different regions of chromosome 5q14 ranging in size from 216 kb to 8.8 Mb. The minimal common deletion region contained only the MEF2C gene. Le Meur et al (2010) noted that the 5q14 region partially overlapped with that deleted in patients with periventricular heterotopia reported by Cardoso et al. But only 1 of those patients has deleted the MEF2C gene. Furthermore, none of the patients reported by Le Meur et al (2010) had periventricular heterotopi [1,4].
Al-Kateb et al. (2013) reported an 8-year-old boy with a de novo deletion of 582 kb on chromosome 5q15, involving 5 genes. They compared their patient's findings with those of 3 patients reported by Cardoso et al. All of them had a minimum overlapping region of about 230 kb including 2 genes: FLJ42709 and NR2F1. All 5 patients had growth delay and facial deformities, 4 had hypotonia and 3 had eye abnormalities. Urinary tract obstruction was observed only in their patient. Periventricular heterotopia was also present only in the patients reported by Cardoso et al. Al-Kateb et al. (2013) stated that NR2F1 is the strongest candidate gene for overlapping phenotypes. Heterozygous mutations in the NR2F1 gene have been identified in patients with Bosch-Boostra-Schaaf optic atrophy syndrome, which is characterized by developmental delay, moderate mental retardation, and visual atrophy [1,5].
Figure 4: Schematic of the distal deletion mutation in the long arm of chromosome 5 [1].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
