
Case report | DOI: https://doi.org/10.31579/2642-973X/064
1 Obstt&Gynae, specialistreproductive endocrinology&Infertility specialist, Centre for Human Reproduction, India
2 Obstt&Gynae Rotunda-A Centre for Human Reproduction, India
3 Neurology Consultant Neurologist Department Swami Satyanand Hospital, Punjab
*Corresponding Author: Kulvinder Kochar Kaur, Obstt&Gynae, specialistreproductive endocrinology&Infertility specialist, Centre for Human Reproduction, India.
Citation: Kulvinder Kochar Kaur, Gautam Nand Allahbadia, Mandeep Singh, (2023), A complicated case of Sjogren’s syndrome (SS), Rheumatoid arthritis, Pyoderma gangrenosum, Quadriparesis, recurrent infections & Ischaemic Stroke, SIADH-an update with review of literature of neurological manifestations in autoimmune disease-A Case Report, J. Brain and Neurological Disorders, 6(5): DOI:10.31579/2642-973X/064
Copyright: © 2023, Kulvinder Kochar Kaur. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 June 2023 | Accepted: 26 June 2023 | Published: 03 July 2023
Keywords: sjogren’s s syndrome (ss); rheumatoid arthritis; pyoderma gangrenosum; recurrent ischaemic stroke; quadriparesis; t2dm
Autoimmune diseases are well known to be associated with neurological manifestations, usually they are not v complicated.Here we report a patient whose initial presentation was in the form of Rheumatoid arthritis whose robustness escalated gradually for which methotrexate 20mg/day , prednisolone-5mg/day, hydroxychloroquinone -400mg5mg/day was started .Over time in view of severe anaemia methotrexate was omitted and 3 units bloodtransfused Gradually she developed TB as well .8 yrs subsequently she generated quadriparesis secondary to recurrent Ischaemic Stroke as,besides pulmonary tuberculosis/herpes zoster subsequent to first dose of rituximab 1000mg iv infusion on day1 following which inview of CD19 zero she never got the second dose till now -9 mths after 1st dose.She had further formed another conditions where involvementofof both innate along with adaptive immune system occur that is pyoderma gangrenosum for which heavy dosage of corticosteroids were given this was followed by drug induced hyperglycaemia one mth later hence steroids were stopped.Despite all attempts at therapy and now on this admission Sjogren’s s syndrome(SS) wasdiagnosed with Ro52 3+,and SSA 2+.On admission she generated SIADH for which tolvaptan was started.Her right limb power has returned but left is still weak ,so she is unable to move.
1.1Sjogren’s syndrome (SS)
Sjogren’s syndrome (SS) constitutes an autoimmune disease whose presentation is in the form of lymphocytic along with plasmacytic infiltration into exocrine glands [1]. The central nervous system (CNS) is implicated in equivalent to 6% of SS patients as well as neurologic symptoms takes place prior to systemic symptoms in greater than 50%of cases [2]. Canonically, CNS implication present in the form of multiple sclerosis (MS)-like injuries in the brain, longitudinally extensive transverse myelitis (LETM), cranial neuropathies, vasculitis, aseptic meningitis, encephalitis, in addition to cerebellar ataxia [3,4]. Noticeably, whereas patients might meet criteria for SS, it is necessary to test for aquaporin-4 IgG as well as myelin oligodendrocyte glycoprotein (MOG) IgG since CNS implication in SS is usually correlated with simultaneous neuromyelitis optica spectrum disorder (NMOSD) [3,4].The confirmation for treatment of CNS disease in SS is restricted along with requires monitoring disease robustness in the form defined by the EULAR (European League Against Rheumatism) Sjogren’s syndrome disease activity index (ESSDAI) [5,6]. Classicalfirst-line therapy for robust inflammatory manifestation includes high dose intravenous methylprednisolone, 1000 mg daily for 3–5 days, followed by a course of oral prednisone, 0.5–1 mg/kg/day tapered over weeks to months [2-7]. Plasmapheresis (PLEX) combined with steroids might offer a strategy with effectiveness for LETM in addition to further mirrors rational empiric therapy given NMO overlap potential [8]. The 2020 EULAR SS guideline recommends cyclophosphamide as well as PLEX +rituximab as second-line and third-line therapy, respectively, for robust CNS implication however but breakthrough disease is frequent (level IV)[7]. Noticeably, however, for MS-like manifestation, MS disease- manipulating immunotherapy is required to be utilized (level V) [6].
1.1A Diagnostic Biomarkers in Sjogren’s syndrome
Autoantibodies to the autoantigens Ro/SSA as well as La/SSB are the most significant biomarkers isolated till date along with have been integrated into the classification criteria for primary Sjogren’s syndrome [5-9]. Subsequent to all these years of scientific evaluation, anti-Ro/SSA in addition to anti-La/SSB are still today significant for the disease classification like they work in the form of diagnostic markers for Sjogren’s syndrome. Ro/SSA as well as La/SSB actually are constituted of three cellular proteins Ro52, Ro60, along with La48 – dependent on their molecular weight, which was discovered in the late 1960s along with early 1970s[10,11]. Based on the testing method utilized, the selection criteria for primary Sjogren’s syndrome, in addition to the patient cohorts, the prevalences of seropositivity are about 70% for Ro52, 40% for Ro60, as well 50%for La48 [12]. The Ro as well as La proteins were first identified in addition to properties studied for their partition in ribonucleoprotein (RNP) complexes with human Y RNAs, which pointed to implication in cellular post-transcriptional controlling. More particular functions were subsequently attributed, with Ro52 (alias TRIM21) revealed to be a ubiquitin E3 ligase, as well as Ro60 in addition to La48 have both been illustrated to be RNA-binding proteins [13]. A data-guided study of international patient cohorts (5) has demonstrated that anti-Ro/SSA is the second-best anticipator of Sjogren’s syndrome subsequent to focus score, when the most recent criteria for Sjogren’ ssyndrome are employed. Anti-nuclear antibodies (ANA) [14]. along with rheumatoid factor (RF) [15]. are further paradigms frequently determined in Sjogren’s syndrome in the form of clinical along with diagnostic gadgets however have only partly made a position inthe classification criterion.
Muscarinic type 3 receptor(M3R) portray one of the new promising biomarkers with direct biological as well as functional links to exocrine liberation. It is thought that antibodies towards M3R might probably hamper saliva liberation [16]. Certain workers have displayeda 60–80% concordance of anti-M3R with Sjogren’s syndrome [17]. but the usage has been inhibited by replication issues and anti-M3R is thereby not widely utilized in the form of a biomarker [18]. in clinical settings. Calprotectin is a complicated marker of the S100A8 and S100A9 proteins observed with enrichment in neutrophils. In the presence of calcium (Ca2+), calprotectin possesses inflammatory in addition to antimicrobial activities. Salivary, however not blood, calprotectin has been illustrated to possess robust association with clinical signs of Sjogren’s syndrome [19]. Serum calprotectin has more recently been illustrated to be a marker for carotid atherosclerosis in primary Sjogren’s syndrome [20]. Reactions to rituximab treatment was further evaluated in a multicentre, randomized, double-blind, placebo-controlled trial known as ‘Tolerance and Efficacy of Rituximab in Primary Sjogren’s Syndrome’ (TEARS) [21]. Patients with primary Sjogren’s syndrome were examined with Salivary gland ultrasonography (SGUS) prior to the first placebo/rituximab infusion along with 6 months subsequently. At every examination, SGUS of the parotid as well as submandibular glands was performed the paradigms echo structure (score 0–4), size of each as well as the gland, along with vascularization dependent on the resistive index of the transverse facial artery of the parotid gland, were recorded prior to as well as subsequent to lemon juice stimulation. Parotid parenchyma echostructure improved in 50% of their rituximab-treated patients in contrast to 7% of the placebo-treated patients (P = 0.03). Submandibular gland echostructure also improved in a larger percentage of rituximab-treated patients, although not statistically significantly. The size of the glands along with the resistive index was unaltered. For diagnostic reasons, recent studies imply that simplified strategy for SGUS evaluation of the major salivary glands might be enough.
1.1A Sjogren’s s syndrome (SS)and weakness of limbs
Sjogren’s s syndrome (SS) has been detailed in the form of an inflammatory disease of salivary in addition to lacrimal glands having the properties of the canonical sicca symptoms presenting with dry mouth in addition to eyes along with lymphocytic infiltration of glandular tissue [22]. Extra glandular presentations are frequent as well as inclusive of inflammation of joints, skin, Kidney, heart, lung as well as Intestines [23]. Inflammation of the nervous system display another complication of SS. Peripheral nervous implication mainly manifests in the form of sensory neuropathy in addition to a broad range of sensory modes as well as organization designs [24]. Motor dysfunction secondary to neuropathy has not been encountered till now in patients with SS[24,25]. Nevertheless, this kind of robust complication of SS with fulminant generation of weakness of limbs however good reactions to immunosuppressive treatment was detailed in various case reports [26,27]. In view of the prevalence of peripheral neuropathy correlated with SS escalates with age [28]. Miscalculation of paralysis in the form of a neurological complication of SS is of extensive risk. Patients whose manifestation is in the form of weakness of limbs as the chief complaint of polyneuropathy are basically given treatment in a neurological unit where SS in the form of an etiologic cause might not be evaluated routinely. In view of diagnosis of SS is in general made in immunological departments, Rheumatologists have greater familiarity with this autoimmune disease in contrast to neurologists.
Seeliger et al. for definition of this condition in detail, evaluated the clinical features of SS patients with neuropathy in addition to motor impairment for promoting diagnostic strategies as well as treatment suitability. They evaluated 184 patients with neuropathy correlated with weakness of limbs who went through all diagnosis procedures inclusive of all investigations for SS.44 patients with Sjogren’s s syndrome (American College of
Rheumatology/European League Against Rheumatism(ACR-EULAR) classification criteria for primary Sjogren’s syndrome are the end result of an international collaboration and have been derived using awell-established and confirmed methodology) in addition to robust neuropathy were isolated. As per their outcomes SS was observed at a median age of 63 yrs as well as gender organization illustrated a ratio that was balanced with a female : male ratio of1:1.AntiSSA(Ro) antibodies were determined in 48% whereas seronegative patients had a diagnosis of SS made dependent on sialadenitis on minor salivary glands biopsy with a focal score of≥ 1. Maximum number of patients(93%) got a diagnosis of SS made subsequent to appearance of neurological symptoms. There was symmetrical involvement of limbs in 84% patients(57% tetraparesiss,27%paraparesis).No influence on sensory function was found in11% of patients pointing that Sjogren’s syndrome correlated neuropathy possess the capacity of presenting in the form of a pure motor syndrome. Electrophysiological determination did not display pathognomic observations(23?myelinating design,36% axonal design,41% both in addition to demyelinating in addition to axonal injury signs. Greater than 50% of their subjects were according to European Federation of Neurological Societies (EFNS) diagnostic criteria regarding chronic demyelinating neuropathy (CIDP), suggesting that differentiation amongst Neuro Sjogren’s in addition to other etiologies of neuropathy for instance CIDP poses a great challenge. Thus, conclusions drawn were that robust neuropathy with weakness of limbs is usually correlated with SS. This holds considerable significance in isolating as well as gaining insight with regards to etiologies of immune modulated poly neuropathy [29].
Rheumatoid arthritis (RA) mirrors an inflammatory condition possessing the properties of joint deformation, synovitis, as well as erosive arthritis [1]. In RA, activated monocytes in addition to lymphocytes infiltrate the joints, skin, eyes, lung, along with blood vessels, inclusive of the nervous system as well [30]. Compressive myelopathy is the most frequent CNS presentation whereas leptomeningitis, encephalitis, as well as CNS vasculitis can further take placealthough such brain implication in RA is rare [31]. Less than half of patients with CNS disease have active synovitis and 34% of patients had no history of RA prior to diagnosis [32]. The most frequent brain MRI observation is nodular patchy or lepto-meningeal thickening as well as enhancement, and biopsy is the gold standard for diagnosis [1-33]. Given that CNS disease in RA is germane occasionally, for therapy effectiveness is restricted to case series in addition to expert opinion [5-34]. Acute compressive myelopathy is maximumfrequently treated with surgical intervention along with IV steroids [5]. The advocated acute therapy for CNS vasculitis is high-dose IV steroids in addition to cyclophosphamide [5-35]. For RA- correlated leptomeningitis, steroids are the maximum frequent treatment to start with, but roughly 50% of patients will not respond to steroids alone [5-37]. Case studies validate the use of either cyclophosphamide or rituximab [36]. Anti-TNF agents should not be utilized as they may be inefficacious and escalate CNS disease activity [33]. Conclusive outcomes are absent with regards to the effectiveness of methotrexate for implication of CNS of RA [1]. According to thought of sustenance therapy, it is significant to notice that the recurrence of RA meningitis occurs occasionally [36]. In addition to disease manipulating therapy, there is confirmation that the transitory neurological deficiencies inRA meningoencephalitis should be treated with antiepileptic drugs (AEDs). Even episodes that are not clearly electroclinical seizures seem to respond toAED’s [33-37].
3.Case Report
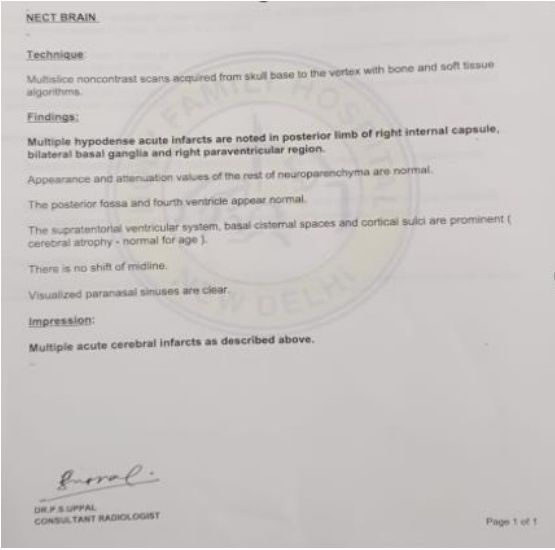
A47 year old lady was admitted with in ICU of GBP hospital with history of 8yrs of joints pains and escalated blood urea, fever x2days 1month back, sudden onset of rt hemiparesis subsequent to high grade fever-subsided with medicines ,2 days later developed sudden altered sensorium in the form of diminished responsiveness ,faecal as well asurine incontinence, altered sensorium on 8/9/22with the diagnosis of old case of Rheumatoid Arthritis(RA) / Sjogren’s s syndrome(SS) / type2Diabetes mellitus(T2DM) / recurrent Ischaemic Stroke/quadriparesis/ pulmonary Tuberculosis/herpes zoster/Bed sores GrII/SIADH. Prior to that in october21she had Pyoderma gangrenosum generated on both ankles for which high steroids given=>hyperglcaemia She was medicated as per that.Onaug2022 she fell semi-conscious at night for which she was shifted to Holy Family emergency .Was diagnosed as brain Stroke as well as pulmonary tuberculosis in left lung subsequent to CT Scan, MRI as well as Contrast MRI- following21 days ICUstty she was shifted to GBP hospital with multiple bed sores, feeding tube along with urinary catheter where she stayed in ICU x10 days followed by transferred to ward. Even here subsequent to Doppler Echo, brain MRI, concluded vasculitis and decided to give rituximab Previous history of 8yrs back was - initiation of methotrexate 20mg/day , prednisolone-5mg/day, hydroxy chloroquine one -400mg5mg/day-initially 200mg followed by bd since 2013 was done -,where prednisolone-5mg/day, and hydroxychloroquine one were omitted in view of patient’s consumption of nonsteroidal anti inflammatory drugs (NSAIDS) off and on for pain, had history of generation of generalized weakness, body aches and pain, easy fatiguability, which was insidious in onset as well as gradually progressive -6mths prior to that she had developed robust an aemia. hence methotrexate was omitted and 3 units blood transfusion was done. -7mths back she formed skin lesions in both ankles which was diagnosed as pyoderma gangrenosum for which heavy dosage of corticosteroids were, given this was followed by drug induced hyper glycaemia one mth later hence steroids were stopped Now she had presented with quadriparesis with altered sensorium On General Physical Examination (GPE)- spontaneous eye opening, poorly responding to commands, reduced verbal output
BP-140/90mmHg, p-96/min, RR-14/min
P+I-, C-, Cl-LN-PE-
CVS-S1, S2were+nt, Chest occasional crepts
Rt Lt
Tone- UL-Rt-increased-- Lt-decreased
LL Rt-increased Lt-decreased
Power - UL- 1/5 0/5
LL 0/5 0/5
PlantarsRt- increased Lt-increased
NR- KS-
4/9/22 14/9/22
CBC-Hb-9.3 9.6
TLC-14100 4900
DLC-94/5 77/16
Plt-6.6l 1.6l
OT/PT-U/ml 51/70 27/55
SB -0.5 mg/ml 0.4 mg/ml
Alp-343 U/ml 289 U/ml
TP/Alb-5.4/2.4 5.1/2.5
INR/APTT- 1.0
Cr/urea- 0.4/42 mg/ml 0.3/21 mg/ml
Na/K-127/4.2mEq/L 128/3.5 mEq/L
AntiCCP-106.21(increased)
APCAProfile- -ve
AntiSSA-++
RO-+++
Rest ANA profile- -ve
CRP-+VE
ESR-65
25/8
Bal-GeneXpert
MTB -detected
Rif-not detected
24/8
cerebrospinal fluid (CSF) -Cells-1
Prot-45
Sugar-69
GeneXpert- MTB -not detected
Fungal c/s—ve
OCB- --ve
SPEP-nor, Tridot- -ve ferrinin-1252
c/s-enterobacter aerogenosa-amika,lfx,meso,mox,diptaz
HbA1c-8
Carotid doppler
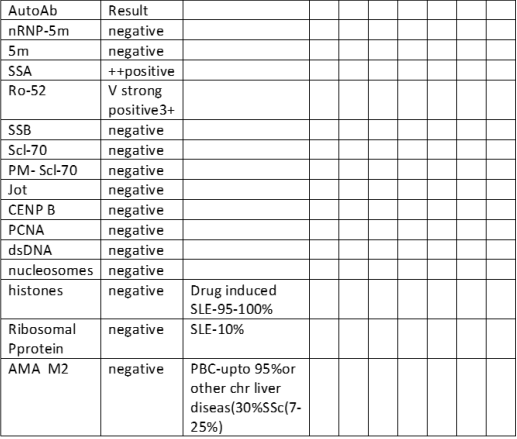
Her ANI profile was as follow
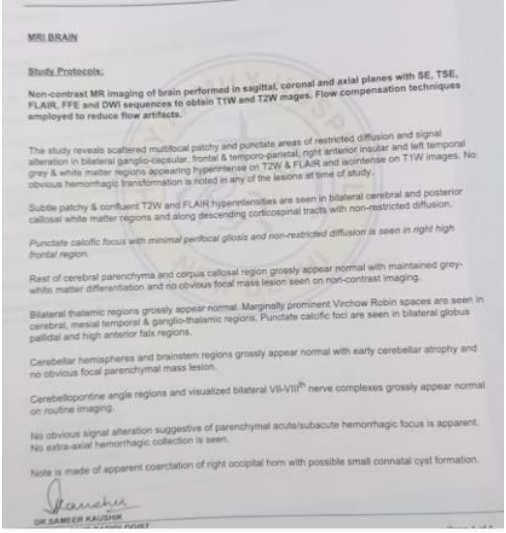
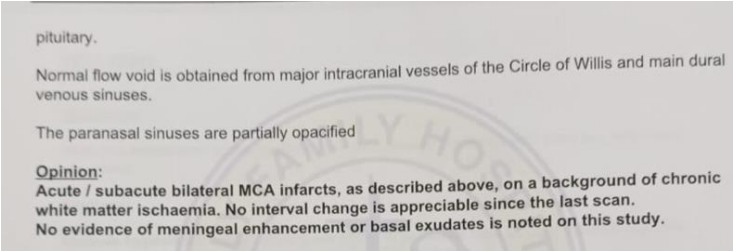
1st MRI REPORT-21/8/22
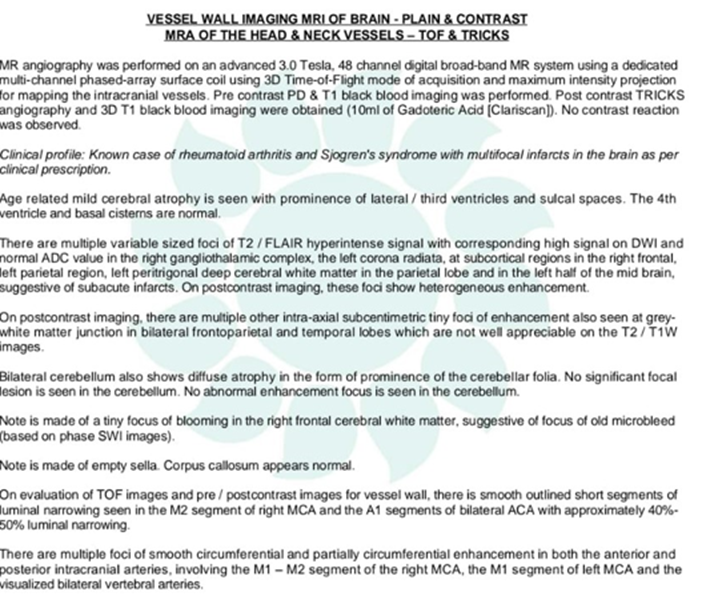
Repeat MRI-ON 28/9/22
Here we present a case of Rheumatoid Arthritis, Sjogren’s s syndrome which was not diagnosed till the development of recurrent Ischaemic Stroke as well as quadriparesis that too only in GBPH as had been suggested by Seeligeretal.[29]. Despite, a known diabetic that had got controlled with medication, she developed pyoderma gangrenosum for which heavy dosage of corticosteroids , subsequent to which she generated drug induced hyperglycaemia one mth later hence steroids were stopped, with her HbA1c rising to 8 .Ours is a complex case who had manifestations of numerous autoimmune diseases like RA, SS, DM, pyoderma gangrenosum which resulted in robust joint pains requiring HCQ, methotrexate ,although we feel she should have received high dose intravenous methylprednisolone, 1000 mg daily for 3–5 days followed by bya course of oral prednisone, 0.5–1 mg/kg/day tapered over weeks to months, rather than toxic methotrexate which led to development of robust anaemia. Gradually over time her condition became inimical with her generating numerous infections like TB, herpes zoster in addition to recurrent Ischaemic Strokes however not till 2022 despite Rheumatologists treating her for8 yrs Sjogren’s s syndrome was not suspected although they had a debate on ruling out APLA syndrome or RF with Sjogren’s s syndrome(SS) in 2020 in view of repeated leptomening it is with blood in CSF & so rituximab infusion was considered in 2020 however postponed in view of expenditure involved. It is our feeling that as recommended by 2020 EULAR SS guideline cyclophosphamide which is the first line drug advocated instead of rituximab that is 3rd line drug subsequent to cyclophosphamide, Plasmapheresis (PLEX) combined with steroids followed by rituximab 1000mg as a third line therapy was needed. She developed herpes zoster in addition to pulmonary tuberculosis following rituximab, besides CSF culture grew enterobacter aerogenosa-sensitive to amika, lfx, meso, mox, diptaz, for which she is getting Levofloxacin 750mg od till now & due toliver toxicity canonical ATT was shifted to streptomycin 750mg ,ethionamide-250mg now and though her right limb function has recovered ,she still has lt weakness with CD 19 count not escalating(still o) and she needed tube feeding till now .Hence one has to keep in mind once there is aberrant behave our of RF, one should keep in mind correlated SS. Furthermore, in view of syndrome of inappropriate antidiuretic hormone secretion (SIADH) production, tolvaptan-15mg od was initiated &further continued with caution not to be given unsupervised. Considering that use of tolvaptan is debatable might be it could have been avoided. Our patient still cannot get up on her own and move around with the expenditure mammoth yet no clear solution in sight .
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
