
Research Article | DOI: https://doi.org/10.31579/2693-2156/004
1 Anesthesiology HOD, Department of Anesthesiology and critical care Command Hospital Airforce Bangalore, India.
2 DM Cardiac Anesthesia, Department of Anesthesiology and critical care Command hospital Airforce, Bangalore, India.
3 DNB Anesthesia, Department of Anesthesiology and critical care Command hospital Airforce Bangalore, India.
4 DM Neuro Anesthesia, Department of Anesthesiology and critical care Command hospital Airforce, Bangalore, India.
*Corresponding Author: Satish Kumar Mishra, Anesthesiology HOD Departement of Anesthesiology and critical care Command Hospital Airforce, Bangalore, India.
Citation: Rajeev Nair, Satish Kumar Mishra, Parli Raghavan Ravi, Avanish Bhardwaj, (2020) A comparitive study between tranexamic acid and epsilon-amino-caproic acid in reducing post-operative bleeding in patients undergoing on pump cabg surgeries. J Thoracic Disease and Cardiothoracic Surgery, 1(1); DOI: 10.31579/2693-2156/004
Copyright: © 2020 Satish Kumar Mishra, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 May 2020 | Accepted: 09 June 2020 | Published: 12 June 2020
Keywords: TA: tranexamic acid; EACA: epsilon-amino-caproic acid; CPB: cardio pulmonary bypass; PRBC: packed red blood cell, FFP: fresh frozen plasma
The amount of strain that cardiac surgery exerts on blood bank services is an example that emphasises the need for multimodel blood conservation stratergy. The most common factor which is being attibutable to increased bleeding after cardiac surgery is hyperfibrinolysis. Thererfore the use of antifibrinolytics during high risk cardiac surgery becomes inevitable. Commonly used antifibrinolytic include Tranexamic Acid(TA) and Epsilon-amino-caproic acid (EACA) .The aim of our study was to compare the effectiveness of both TA and EACA in reducing post surgical bleeding in on-pump CABG surgeries and to asses the post operative complications associated with its use.Material and Methods After obtaining informed written consent,approval of ethics and research commitee patients who were scheduled for on-pump CABG were included in the study.Patients were divided into two groups randomly by using a comupter generated randomized block design namely group TA(n=40) and group EACA (n=40). TA group received tranaxamic acid at a dose of 10mg/kg IV over 20 min at the time of induction then 1-2 mg/kg in CPB prime followed by 1 mg /kg/hr infusion during surgery. Group EACA received EACA in a dose of 100mg/kg/IV over 20 min at he time of induction then 5-10mg/kg in CPB prime followed by 10mg/kg/hr infusion during surgery . Pateints were assessed for blood loss and were monitored for fibrinogen level and D- dimer levels, Re-exploration and post operative complications. Result Primary outcomes like bleeding at 4hrs, there was no significant difference between the groups but when total bleeding at 24 hrs was compared there was a significantly lesser bleed in group TA group compared to group EACA (P=0.0022).The requirement of PRBC in group TA was for 3 patients,where as in EACA group 4 patients required PRBC (P>0.05).There was no significant difference in the rate of post operative complications between the groups.(P>0.05) .Conclusion from our study we concluded that both TA & EACA effectively inhibits fibrinolysis during on pump CABG surgery and thus results in decreased post operative bleeding.When compared between the two, TA was slightly better with respect to post operative bleeding at 24hrs.Our study also re emphesized the fact that neither of the drug led to any additional risk of post operative thrombotic complications.
For decades the most common indication for blood transfusion is perioperative bleeding and cardiac surgery ranks high on the list. The reason which is being attributable to this complication is the institution of Cardio Pulmonary Bypass (CPB). CPB leads to series of events like compliment activation, platelet Activation and increased fibrinolysis which contributes to increased post operative bleeding1 .Post operative bleeding in itself carries a high risk for in hospital mortality. Cardiac surgical patients who are taken up for re exploration due to bleeding carry a four fold increase in mortality and sternal wound infection 2. Therefore a multimodal approach is recommended to reduce perioperative bleeding which includes the use of antifibrinolytic agents.
Anti fibrinolytic agents have been used during cardiac surgery to reduce the risk of post operative bleeding. Most commonly used antifibrinolytic agents include Aprotinin and lysine analogs (Tranexamic acid TA and E- amino caproic acid EACA).
Aprotinin is a serine protease inhibitor which inhibits multiple proteases like plasmin, kallikrein, trypsin, and activated factor XII, there by reducing blood loss.in 2007 a prospective study on high risk patients undergoing cardiac surgery know as Blood conservation using Antifibrinolytics in a Randomized Trial (BART) reported an increased mortality with use of aprotonin compared to lysine analogs 3 . Later due to warning from Food and Drug administration (FDA) ,Bayer health care withdrew aprotinin from the market. Now the Society of Thoracic Surgeons (STS) guidelines 4 recommend the use of anti‐fibrinolytic agents (only lysine analogues), as a strategy to reduce perioperative blood loss during cardiac surgery.
Tranexemic acid (TA) is a synthetic antifibrinolytic that blocks lysine binding site on plasminogen molecule, thus inhibiting the interaction with plasmin and fibrin which leads to decreased post operative bleeding5-6. Similarly EACA is a synthetic lysin analog which reduces the rate of plasmin formation and further decreases the degradation of fibrin to fibrin degradation product (FDP)7. Apart from this EACA also has a platelet sparing action which leads in inhibition of plasmin mediated platelet injury8 .
Both TA and EACA have been shown to decrease post operative bleeding associated with CPB. However there are no large studies comparing the effectiveness of both drugs in pateints undergoing on pump CABG surgeries.
The aim of our study was to compare the effectiveness of both TA and EACA in reducing post surgical bleeding in on-pump CABG surgeries with regards to the amount of blood loss at 4Hrs and 24Hrs as the primary outcome. The secondary outcome of our study included the rate of transfusion of packed red blood cell (PRBC), fresh frozen plasma(FFP) and platelets, re exploration rates, post operative D-dimer and fibrinogen levels.
After obtaining informed written consent, approval of ethics and research committee patients who were scheduled for on-pump CABG were included in the study. This study was carried out between June 2019 to Feb 2020. Patients with concomitant valvular heart disease, recent Myocardiac Infarction (MI<4wks) Ejection Fraction <40%, Preexisting neurological, pulmonary or hepatic dysfunction were excluded from the study.
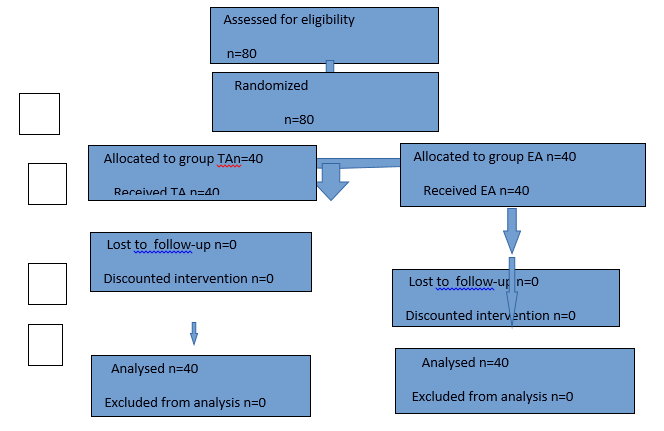
Patients were divided into two groups randomly by using a computer generated randomized block design namely group TA(n=40) and group EACA (n=40). In both the group under strict aseptic precaution under local anesthesia a wide bore peripheral IV cannula, right radial artery cannulation and right femoral artery cannulation was done for continuous hemodynamic monitoring. Anesthesia was induced with Inj etomidate (0.2mg/kg), Inj Fentanyl (3-5 ug/kg) and Inj Rocuronium (0.8-1mg /Kg). After induction of patient right internal jugular vein cannulation was done with 7.5 Fr Triple lumen catheter and PA catheter was inserted. Anesthesia was maintained with air and oxygen (50%),sevoflurane (1-3%) and Inj Atracurium (0.5-1mg/Kg). After sternotomy and heparinization CPB was established once ACT was >420 Sec.
TA group received tranaxamic acid at a dose of 10mg/kg IV over 20 min at the time of induction then 1-2 mg/kg in CPB prime followed by 1 mg /kg/hr infusion during surgery. Group EACA received EACA in a dose of 100mg/kg/IV over 20 min at he time of induction then 5-10mg/kg in CPB prime followed by 10mg/kg/hr infusion during surgery . Later Inj Protamine was administered to reverse the effect of Heparin.
After the completion of surgery patients were shifted to ICU and were assessed for blood loss at 4 hrs and 24 hrs after shifting. Indication for transfusion of PRBC was a haemoglobin level of < 8gm/dl. FFP was transfused if post operative drain was > 250ml/hr in first hour. Platelet transfusion was indicated if platelets counts were <50000/mm3. The degree of fibrinolysis was measured by Thromboelastography (TEG),(Hemostasis system, Haemoscope corporation USA)
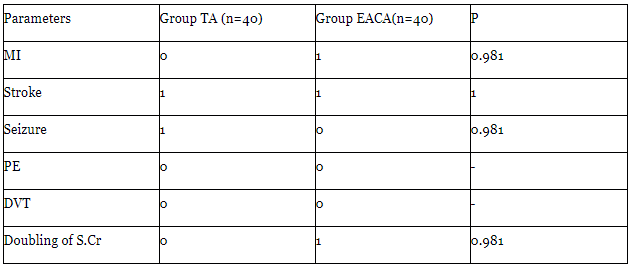
Other parameters which were monitored included fibrinogen level and D- dimer levels at 4 hrs and 24 hrs. Re-exploration of case was considered if the bleeding was > 300ml/hr in first 2 hrs or if >200 ml/hr for 4 consecutive hrs, with normal coagulation data. Patients were also observed for post operative complications like MI, Stroke, Deep vein thrombosis (DVT),renal dysfunction and seizures for 72 hrs.
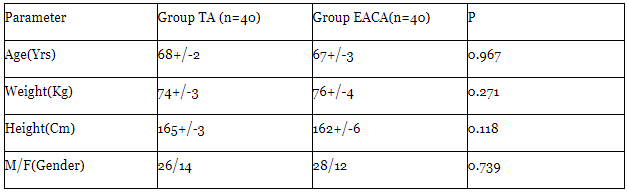
Demographic variables like age,weight,height, male-female ratio were comparable in both groups. (Table-1)
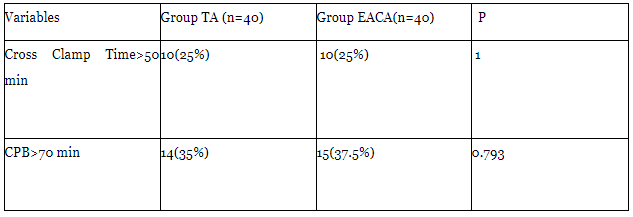
The cross clamp time & duration on CPB were also comparable in both groups (Table-2).
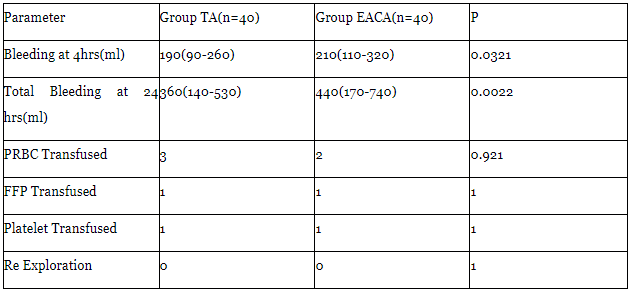
Primary outcomes like bleeding at 4hrs, there was no significant difference between the groups but when total bleeding at 24 hrs was compared there was a significantly lesser bleed in group TA group compared to group EACA (P=0.0022).
The requirement of PRBC in group TA was for 3 patients,where as in EACA group 4 patients required PRBC (P>0.05). One pateint in each group required FFP transfusion (P>0.05).Both the groups did not require any platelet transfusion & the transfusion rate was non-significant between the groups. Both the groups had no re exploration due to excessive bleeding (Table-3).
There was no significant difference in the rate of post operative complications between the groups. (P>0.05) (Table-4),
Statistical analysis was done with SPSS software version 19.0 normality of the test were checked using Kolmogorov-smirnov test. The values which were obtained were analyzed and were expressed as mean +/- Standard Deviation (SD) and median +/- range. For continuous variables for parametric data,Indepedent's test were used and for non parametric data Mann-Whitney u test were used. For categorical data, Chi-Square test or fisher's exact test were used. A P Value of <0.05 was considered to be statistically significant.
On pump CABG is associated with increasesd risk of post operative bleeding compared to OPCAB9-10 reason best attributable to use of CPB, which is associated with increased fibrinolysis & increased concentration of inflammatory mediators,which has urged researchers all around the world to investigate the probable role of antifibrinolytics in on pump cardiac surgeries 11.
In our study we found that there was no significant difference in the amount of post operative bleeding at 4 hours between the groups however at 24 hrs there was a significant difference between both the groups with lesser bleeding in group TA compared to group EACA. This may be due to the fact the TA is 10 times more potent than EACA12. Similar findings were obtained in a study comparing TA & EACA with placebo conducted by Karski Et al13.
Chauhan Et al 14 & Faure Et al 15while comparing both the drugs showed that there was no significant difference in the rate of post operative transfusion of PRBC,FFP / Platelet or the rate of re-exploration for excessive bleeding,which was comparable with our study.
Post operative blood transfusion after CABG is associated with increased long term mortality16. .Therefore the role of these drugs in reducing the transfusion rate after on pump CABG is very significant. There were no difference in the rate of post operative copmlications between the gropus. Hardy Et al in his study while comparing both the drugs did not find any significant difference between the drugs with regards to post operative thrombo embolic complications17.
There are controversis with regards to the dosing of the drug .A high dose(20mg/kg) TA is associated with increased risk of post operative seizures and therfore a low dose (10mg/kg) regiem is recommended18.Armelin et al compared the low dose and high dose TA regiem and found no difference with respect to amount of post operative blood loss or transfusion requirement19.In our study we used low dose TA dosing and did not find any significant post operative complications.
Based on the results of our study it can be concluded that both TA & EACA effectively inhibits fibrinolysis during on pump CABG surgery and thus results in decreased post operative bleeding.When compared between the two, TA was slightly better with respect to post operative bleeding at 24hrs.
Our study also re emphesized the fact that neither of the drug led to any additional risk of post operative thrombotic complications & thus can potentially become an standard of care for blood conservation in patients undergoing on pump CABG.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
