
Research Article | DOI: https://doi.org/10.31579/2690-1919/300
ENT Consultant \ ENT Department in Baaquba teaching Hospital
*Corresponding Author: Nasser Khalil Muhammed. ENT Consultant \ ENT Department in Baaquba teaching Hospital.
Citation: Nasser Khalil Muhammed, Amer Jawad Kadhim , Samih Faiq Fadhil, (2023) A Comparative Study on Intraoperative Local Mitomycine_ c Application in Primary Endoscopic Dacrocystorhinostomy (dcr) with Conventional Primary Endoscpic (dcr). J Clinical Research and Reports, 13(2); DOI:10.31579/2690-1919/300
Copyright: © 2023 Nasser Khalil Muhammed. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 January 2023 | Accepted: 31 January 2023 | Published: 03 February 2023
Keywords: mitomycin c; endoscopic dacrocystorhinostomy ; epiphora
Epiphora is an overflow of tears onto the face due to imperfect drainage of the tear conducting passages or excess lacrimal production.
Dacrocystorhinostomy ( DCR) is recognized as the most suitable treatment for patients with obstruction of the lacrimal system at the level of lacrimal sac or in nasolacrimal duct with aim of creation a bypass between lacrimal sac and the nasal cavity ( 1 ) The two most frequent causes of DCR failure are obstruction of the common canaliculus and closure of the osteotomy site. Thus if we can inhibit fibrous tissue growth and scarring by applying antiproliferative agents over the anastamosed flaps and osteostomy site , the failure rate may be decreased. (2)Mitomycin C is an antibiotic, antineoplastic agent inhibiting DNA, RNA and Protein synthesis. ( 3 )
Objectives: To evaluate the use of local intraoperative Mitomycin C in endoscopic DCR and comparing this with endoscopic DCR without Mitomycin C.
Methods:
In our study, a total of 77 eyes diagnosed with aquired epiphora were divided into a (Mitomycin C group) that we use local application of Mitomycin C intraoperativly in endoscopic DCR, and a (Non Mitomycin C group) in which no Mitomycin C is used. All done at Al-amal- day-case private clinic and Baqubah teaching hospital since 7th of May 2019 till 1st of March 2022.
Surgical procedures steps is the same in both groups, except in that (Mitomycin C) group was subjected to an application of local mitomycin C 0.2mg\ml for 5 minutes and this was done with the aid of Merocele that soaked in this substance. Merocele soaked with Mitomycin C 0.2mg\ml was applied to the osteotomy site and the margines of the flaps of the opening of the lacrimal sac for 5 minutes. The results of surgeries in both groups were evaluated by both subjectivly by asking patients about the result of surgery and if they still complaining of excessive tearing or not , and also were evaluated objectivly (by flexible fibro-optic nasoendoscope) to see the site of surgery and the opening of the lacrimal sac to the nasal cavity
Results: 40 eyes that are the ( Non Mitomycin C group ) were evaluated after 9 months after surgery ,this evaluation is done subjectively and objectively ,38 cases were symptom free and the endoscopic findings showed us opend and clean openings of the fistulae we created .2 cases give history of excessive tearing (go with recurrence ),in this cases , no benefit from syringing, and the endoscopic finding showed fibrous tissue adhesions that come from the axilla of the middle turbinate to the opening of the sac we created and also extends to the nasal septum and surrounding tissues.
In the other group of the 37 cases ( Mitomycin C ) group , patients give no symptoms of excessive tearing except 1 case , flexible fibro_optic endonasal endoscopic examination of these patients showed patent orifices created in our surgeries with no adhesion or fibous bands affect the tears passageway.the recurrent epiphoric patient was got no benefit from syringing and the endoscopic findings (this was after 9 monthes of the surgery) showed adhesion bands surround the area near the orifice created , ( really the septum in this case was near the orifice(not attached to it) but our decision during the surgery was not to do septoplasty )
Conclusion: intraoperative Mitomyicin C has little( no significant) effect on the results of DCR surgery.
Epiphora is an overflow of tears onto the face due to imperfect drainage of the tear conducting passages or excess lacrimal production.It is a common condition with many causes, a thorough history and examination are required to provide the appropriate treatment tailored to the underlying cause [4]. Epiphora not has a negative impact on patients comfort only, but also put them at risk for probable intraocular operations in the future [5] . Probing as a first line therapy shows 82% successullness in cases of nasolacrimal duct obstructions,so it is recomended as initial treatment procedure [3]. Medical treatment with nasal steroid spray may be effective but the majority of obstructed cases will require surgical intervention in the form of Dacrocystorhinostomy [6]. So DCR is the treatment of choice in resistant cases.
It should be known that epiphora may generate and lead to serious problems [5]
Dacrocystorhinostomy (DCR) (external and endoscopic approach) (a procedure performed for the treatment of epiphora) revealed high succeess rate and low risk of complicationsis [7]. Significant epiphora due to obstruction,chronic conjuctivitis, dacrocystitis & Dacryoliths in lacrimal sac causing periodic episodes of nasolacrimal duct obstruction are the main indications for DCR [8]. Endonasal DCR involves creation of a large ostium and construction of nasal and lacrimal sac mucosal flaps [9] Failure to maintain this patency will result in failure of the procedure [2] . Failure is generally defined as having symptoms of excessive tearing with the inability to irrigate [10]. The two main causes of failure of dacrocystorhinostomy are obstruction of the main canaliculus and closure of the osteotomy site by fibrosis and scar formation [2] Mitomycin C (MMC) is an antineoplastic agent that inhibits the synthesis of DNA, cellular RNA, and protein by inhibiting the synthesis of collagen by fibroblasts [11] It is an alkylatng agent that inhibits fibroblast proliferation and alter wound healing response leading to less fibrosis and scar formation around the common canaliculus and osteotomy site [2] Mitomycin C (MMC) is a chemotherapeutic antibiotic isolated from the broth of Streptomyces caespitosus. Its mode of action mimics that of ionising radiation. Cross linkage of the DNA base pairs adenine and guanine inhibits DNA synthesis in all phases of the cell cycle. Mitomycin C also causes breakage of single stranded DNA. Although its action is non-cell cycle specific, rapidly dividing cells are preferentially sensitive to these effects.[12] MMC has been used as an adjuvant treatment in DCR since 1998 to prevent excessive scarring and fibrosis causing adhesions in the postoperative period [13] They found attenuated epithelium with intracytoplasmic vacuoles and loose subepithelial connective tissue that was hypocellular on histopathological examination [14] Shi ming cheng and his colleagues concluded that intraoperative MMC application seems to be a safe adjuvant that could reduce the closure rate of the osteotomy and enhance the success rate after both primary and revision EN-DCR [11] . Intraoperative mitomycin C application is effective in increasing the success rate of DCR surgery in standard nasolacrimal duct obstruction, and no significant complications resulted from its use. [10] Güler Zilelioğlu in his paper said that Adjunctive use of a wound healing inhibitor is considered to increase the success rate of endoscopic endonasal DCR. Its intraoperative use seems to be easy and safe. But the study of this limited series shows no benefit in using it [16]. However, according to others, adjuvant use of MMC to prevent failure in Ex-DCR or EnDCR is innocuous and does not change the chance of success of the DCR procedure [13] Obstruction of the puncta or canaliculi is not an infrequent event after topical 0.04% MMC [12]. Contraindications of Mitomycin-C for topical use One-eyed patients, pregnant women, very old patients, severe dry eye, those with predisposing condition to corneal ulceration or poor healing such as immunocompromised patients or patients with Sjogren’s syndrome, atopic keratoconjunctivitis, acne rosacea or herpetic keratitis [15].
This study done to compare results of DCR that use local intraoperative application of Mitomycin C, with DCR that done conventionaly without this application use. All done at Al-amal- day-case private clinic and Baqubah teaching hospital since 7th of May 2019 till 1st of March 2022.
Endoscopic DCR done for patients (the ages range from 11years old to 70 years old), they were complaining from excessive tearing due to acquired nasolacrimal duct obstruction. Final diagnosis was done by the ophthalmologist Dr Amer J. K.We exclude congenital cases, canalicular obstruction, revision surgery, traumatic obstruction ,excessive tearing due to previous facial nerve palsy ,ectropion and connective tissue disease.
There are two groups of patients: (Mitomycin C group) that we use local Mitomycin C intraoperativly in endoscopic DCR, and a (Non Mitomycin C group) in which no Mitomycin C is used. In both groups we followed same surgical steps except that final step in which we applyed Mitomycin C 0.2mg\ml to the osteotomy site and the margins of the flaps of the opening of the lacrimal sac (this of course in the Mitomycin C group).Any patient in both groups need septoplasty to facilitate entrance to the site of the axilla of the middle turbinate or the site of nasolacrimal duct, we did it (Otolaryngologist Dr Nasser). Under general anaesthesia with hypotensive technique , a local nasal decongestion using Merocele soaked in Adrenaline:Lidocain 1:100000, waiting for about 5 minutes a no. 15 scalpel blade is used to make the initial mucosal incisions .The first incision is made horizontaly 8 to 10 mm above the axilla of the middle turbinate, starting 3mm posterior to the axilla and coming forward about 10 mm to the frontal process of maxilla ,from this end start another vertical incision extending to the level of insersion of the inferior turbinate ,from this end start another inferior horizontal incision that extend posteriorly to the insersion of the Uncinate process, this mucosal flap is elevated by freer elevator ,when reach the junction of the soft lacrimal bone with the hard frontal process ,remove the lacrimal bone, then use a Hajek Koeffler punch to remove the lower part of the frontal process of the maxilla pushing the lacrimal sac ( for protection) by the tip of this punch ,bone removal continue anteriorly and superiorly untill no bone can be grasped by the punch, this will uncover the antero-inferior part of the sac,the rest of the thick bone up to the level of the anteror mucosal flap can be removed by a small (2-3 mm)chizzle that used for osteotomy in Rhinoplasty (I have no drill) ,in most of the cases Agger nasi cell will be exposed at this stage and its mucosa will be exposed ,bone will be removed untill all the lacrimal sac is exposed at this stage of the surgery, opthalmologist start to dilate the inferior punctum with punctum dilator , and a bowman lacrimal probe is pass to the sac , then when the probe is moved up and down in the sac ,its tip should be seen behind the wall to confirm being within the sac. Then DCR spear knife is used to make vertical incision as far posteriorly as possible , the sac is slit from top to bottom , DCR mini-sickle knife is used to make upper and lower releasing incision in the anterior flap so that the flap can be rolled out on the lateral nasal wall. Three mm soft tissue scissors are used to make upper and lower releasing incision in the posterior flap, and this flap is also rolled out, the sac now is completely marsupilised and lie on the lateral nasal wall. The mucosal flap is trimmed so that the superior and inferior mucosal flap are matched to the row bone above and below the opened lacrimal sac. Most of the middle of the original flap is removed so that we can approximate it to the mucosal flap and the healing occur by first intention rather than by second intention which leads to granulation tissue formation and later closure by scar formation. No silicon lacrimal intubation tubes are used, nasal mucosal flaps(anterior and posterior ) and lacrimal sac flaps were joined together with 5-0 vicryl suture. In the ( Mitomycin C group ),a piece of Merocele attached with a long thread soaked in 0.2mg\ml mitomycin C was placed over the anastomosed flaps and osteotomy site with the long thread passing through the nostril ,and was then removed after application time of 5 minutes by pulling the thread. a piece of Merocele attached to a thread is put on position to stabilize the flap.in the first post-operative day we remove the piece of merocele gently by pulling the thread, give broad-spectrum antibiotics for 7 days, starting nasal wash with normal saline, this wash we contiue with it at least for 2 weeks, really we instruct the patint to visit us in 1,3,10 days post operativly, then1,2,4,6 and 9 month post operativly,. The results of surgeries in both groups were evaluated by both subjectivly by asking patients about the result of surgery and if they still complaining of excessive tearing or not , and also were evaluated objectivly (by flexible fibro-optic nasoendoscope) to see the site of surgery and the opening of the lacrimal sac to the nasal cavity,(and by syringing).so we did naso-endoscopy to all patients at 9 month post-operative period ,but any patint had a complain of excesive tearing told us during the visit we will do syringing followed by nasal endoscopy to evaluate the condition.
In our study we did 77 DCR surgeries that we divide them into two groups, 1st is the (Mitomycin C group) ( 37 eyes ) in which we used to put(of course after the conventional surgery for both groups) Mitomycin C in concentration of (0.2mg\ml) on the margins of the flaps of the opening of the lacrimal sac and osteomy site for 5 minutes , 2nd group ( 40 eyes )( Non Mitomycin C group ) in which we just escape the step of putting Mitomycin C on the flaps . Concurrent septoplasty was done in 5 cases ,3 cases from Mitomycin group and 2 from non mitomycin group. The age of the patients is ranging from 11 to 70 years old ,55 were females and 22 were males, epiphora was the presenting symptoms in 53 cases while other patients were present with swelling in the lacrimal cyst region

Table (1): Distribution of patients according to gender.
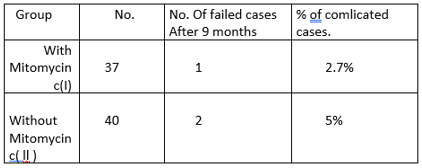
Table (2): show no. Of cases of DCR done with and without Mitomycin c and no. and percentage of its complications
Otolaryngologists move in the recent years to the field of DCR after the evolution of endoscopic instrumentations. Epiphora due to nasolacrimal duct obstruction is managed successfully by this surgery .recurrence of excessive tearing with inability to irrigate is an expected complication of this surgery. In primary external and endoscopic DCR, the failure rate has been reported to be 5% -10% and 20% -40% respectivly [17 ], this is due to fibrosis and scar formation [2] , thus if we can reduce fibrous formation at the site of osteotomy and flaps ,the success rate of the surgery supposed to be bigger.[10] Mitomycin C is the substance that used in many centrs for this purpuse.
ln our study, the rate of success in group l (Mitomycin c groupe) is (100%), and in groupe II (non Mitomycin c groupe) is (97.5%). This means that Mitomycin c is of no additional benefit in endoscopic DCR. Tamata T.S. Sousa concluded that intraoperative use of Mitomycin c is safe and slightly improves the success rate of external or endoscopic DCR, however the evidence was very weak [13]. S.Liao said intraoperative Mitomycin C is effective in increasing the success rate of DCR surgery in standard nasolacrimal duct obstruction surgery , and no significant complications resulted from its use [10]. Shi-ming Cheng concluded in his paper that intraoperatve Mitomycin C applications seems to be safe adjuvant that could reduce the closure rate of the osteotomy and enhance the success rate after both primary and revision endoscopic DCR [11].Our study is comparable with study of M.H. Roozitalab who concluded that the use of intraoperative Mitomycin C in DCR surgery does not change the success rate of this procedure [18]
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
