
Review Article | DOI: https://doi.org/10.31579/2690-4861/315
1 Physical. Rehabilitation Dept. King Faisal Specialist Hospital and Research Center, Riyadh, KSA.
2 Critical Care Nursing Dept. King Faisal Specialist Hospital and Research Center, Riyadh, KSA.
3 Respiratory Services Dept. King Faisal Specialist Hospital and Research Center, Riyadh, KSA.
*Corresponding Author: Mohammed Takroni, Cardiopulmonary Rehabilitation Specialist, Physical Rehabilitation Department, King Faisal Specialist Hospital& Research Center, Riyadh, Saudi Arabia.
Citation: Mohammed T., Al-Thumayri Abdulaziz, Shiji P., Al-Elissa S., Ahmed M., (2023), A Clinical Review of Physical Rehabilitation Protocol and Early Mobilization Patterns for Post-Covid-19 Patients: Tertiary Health-Care Facility Experience, International Journal of Clinical Case Reports and Reviews, 14(1); DOI:10.31579/2690-4861/315
Copyright: © 2023, Mohammed Takroni. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 May 2023 | Accepted: 29 May 2023 | Published: 06 June 2023
Keywords: ICU, COVID-19, rehabilitation, respiratory-care, early mobilization
Several studies have emphasized the urgent need for Physical Rehabilitation guidelines for COVID-19 patients and the effect of Early Mobilization (EM) in these patients. previous reports revealed that dealing with COVID-19 patients was based on expert opinion, evidence from patients with other lung diseases, and not on the recent literature concerning COVID-19. International guidelines also reported that early mobilization is safe and feasible, starting in the ICU setting. Therefore, this clinical literature review aimed to designate the indications of physical rehabilitation programs and early mobilization benefits to add to the existing literature the necessary up-to-date recommendations and share the experience of a tertiary healthcare facility in dealing with different stages of post-COVID-19 patients. Conclusion: The multidisciplinary approach of KFSH&RC for rehabilitating COVID-19 patients was integrated through early mobilization and remarkable follow-up of different clinical services divisions including physical and occupational rehabilitation, respiratory therapy, and nutrition, with the collaboration of the medical and psychological teams aiming to regain optimal physical function, psychological well-being, and better quality of life for those populations.
Patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), Known as a novel severe acute respiratory syndrome coronavirus (COVID-19) may have different symptoms involvements.[1] Some individuals may present with no or mild symptoms that do not require hospitalization, whereas others may present with severe symptoms that require hospital or intensive care unit (ICU) admission. Studies have stated that about 14% of individuals present with severe forms of COVID-19 symptoms requiring hospitalization and oxygen therapy; however, only 5% present with severe symptoms that necessitate admission to the ICU. [2, 3] COVID-19 symptoms may include numerous comorbidities such as respiratory failure, physical deconditioning, muscle weakness, [4] acute cerebrovascular diseases, and or acute cardiac injury. [6] Studies reported that in the ICU, COVID-19 patients may be exposed to infections, including ventilator-associated pneumonia, catheter-associated bloodstream infections, urinary tract infections, venous thromboembolism (VTE), delirium, myopathies, and neuropathies related to critical illness and stress ulcers; some patients develop neurological complications, psychological disorders, and cognitive impairments. [7-11] Other studies also showed that the incidence of ICU-acquired weakness (ICU-AW) ranges from 25 to 31% with about 3.25–6.2 million new patients annually. [12, 13] ICU-AW varies depending on age, sex, primary disease, and treatment. Up to 70% of elderly patients in the ICU experience complications due to muscle atrophy. According to current studies, the incidence of ICU-AW is estimated to be 40% in patients on mechanical ventilation for more than 7 days. De Jonghe et al. [14] confirmed that skeletal muscle is correlated with immune function and glucose and protein metabolism, and such patients have significantly higher mortality. It has been recognized that Musculoskeletal dysfunction and weakness is very common after acute critical illness, or in the ICU setting, about 25% of patients have muscle weakness. [13,14] A study of 116 patients reported that a reduction in limb strength was associated with respiratory muscle weakness and delayed weaning from mechanical ventilation. This study concluded that if these symptoms were not enclosed by early exercise and mobilization programs, they may lead to prolonged ICU and hospital length of stay (LOS).[15] Most previous studies and reports necessitate an urgent need to develop rehabilitation recommendations for COVID-19 patients that aim to guide the rehabilitation field and healthcare professionals to safe and effective practice. [15, 16] These recommendations can guide clinicians to the essential early rehabilitation programs for COVID-19 patients, which have been poorly utilized during and after the pandemic. The existing guidelines in the Kingdom of Saudi Arabia (KSA) are mostly oriented toward respiratory problems, showing a clear limitation on the importance of early mobilization and the role of physical and occupational rehabilitation for those populations. The term "early mobilization" refers to an implementation of physiotherapy programs (passive or active mobilization, breathing exercise, respiratory muscle training, etc.) [17]. Systematic reviews reported that EM for post-COVID-19 and ICU patients require interdisciplinary team cooperation, and can be performed by different health professionals, particularly physiotherapists, respiratory therapists, occupational therapists, and nursing teams [9,16,18,19,20]. Therefore, this clinical review aimed to highlight on the indications of physical rehabilitation programs and early mobilization benefits, add to the existing guidelines the necessary up-to-date recommendations, and share the experience of a tertiary healthcare facility in dealing with different stages of post-COVID-19 conditions or patients’ post-acute illness.
Stages and definitions of COVID-19
The Infection Control and Hospital Epidemiology (ICHE) Department at King Faisal Specialist Hospital and Research Center (KFSHRC) developed adult guidelines for the management of COVID-19 and categorize COVID-19 patients into stages according to their symptoms.[21] These symptoms were divided into four different categories according to the severity of the disease, the severity of the symptoms, the requirement for hospital ICU admission, and the necessity for a mechanical ventilator. Since there are minor variations in the severity of COVID-19, the ICHE department followed the Saudi Ministry of Health (MOH) classifications,[22] which adopted from the World Health Organization (WHO)’s classification and definition of COVID-19 severity for adults.[1] The stages and definition of COVID-19 patients are demonstrated in Table 1:
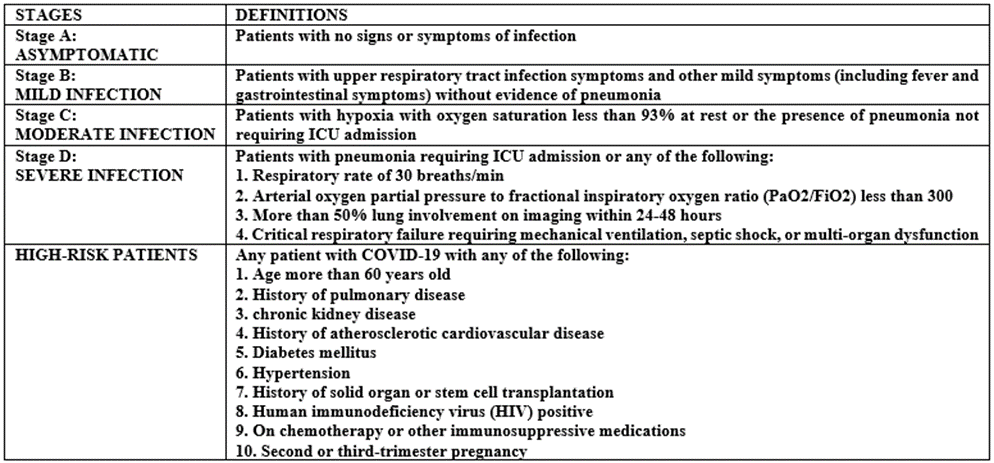
Table 1: Stages & Definition of COVID-19. [22]
Impact of Early Mobilization (EM) on Post COVID-19
The limitations in movement, prolonged bed rest, and immobilization of COVID-19 patients in the ICU are common practices, especially for sick patients requiring sedation and mechanical and high-alert drug therapy. [23] Although these restrictions are essential parts of the delivered care for COVID-19 patients in the ICU, they may cause serious physical and psychological damage. It has been observed that during their hospitalization period and even after their discharge from the hospital, patients often exhibit neuromuscular weakness, reduced cognitive function, and various psychological side effects. In addition, patients with COVID-19 admitted to the ICU may have multiple organ failures, including ARDS, acute kidney injury, cardiac injury, and liver dysfunction. [24] In association with these factors, mechanical ventilation duration in the ICU is another factor associated with acquired weakness, which is widely accepted to describe the difficult situation experienced by ICU patients. Studies reported that approximately 75-80% of patients hospitalized with COVID-19 have prolonged hospital stays of approximately 21 days. [25, 26] Muscle weakness and nerve damage started on the first day of hospitalization. Some of these patients have associated comorbidities such as advanced age, renal dysfunction, hypertension, diabetes, and heart disease, which may contribute to the incidence of ICU-AW. [12, 13, 15] All these factors contribute to immobility, which, in turn, has deleterious effects on the cardiorespiratory, nervous, musculoskeletal systems, and metabolism, leading to major changes in the patient's daily life and reduced quality of life. [26] Several international guidelines support early mobilization and have reported that it is safe and feasible in the ICU setting. Therefore, immediate action of early mobilization intervention has to be taken for those special populations to prevent their complications, improve muscle power, decrease ICU and hospital length of stay, and improve their quality of life. [27, 28, 29]
Evidence on EM, and Exercise Program
Earlier reports specified that dealing with COVID-19 patients was not dependent on recent literature but was mostly based on expert opinion and evidence from patients with other lung diseases. [30] Numerous clinical trials have emphasized the need for urgent up-to-date guidelines on the rehabilitation of COVID-19 patients. [2, 30, 31] A study by Schweickert et al. [32] also stated that EM and Rehabilitation have significant benefits for ICU patients in terms of functional capacity upon discharge from the hospital and should be initiated as early as possible. Several randomized control trials (RCT) and meta-analyses specified that EM intervention for COVID-19 patients helps in reducing the deleterious effects of the disease on cardiopulmonary function, mobility, muscle weakness, and functionality. [33,34] In addition, recent reviews by Goodwin et al. [35] and Bernal-Utrera et al. [36] reported that physical therapy exercise, early mobilization, and multi-component programs are necessary strategies to improve recovery after ICU admission for severe respiratory illness, and contribute to patient stability during critical periods for patients with COVID-19.
Referring COVID-19 patients to Physical Rehabilitation
In KFSHRC, the patients’ referral system follows the Saudi Ministry of Health (MOH) guidelines referral system. [22] If a COVID-19 patient is admitted to the ICU, will be assessed by the ICU multidisciplinary COVID-19 team. If the patient is hemodynamically stable, the team will refer the patient to the Physical Rehabilitation Services or other clinical services facilities. Patients can be referred also to Physical Rehabilitation services by other services that have been involved in the patients’ care such as pulmonologists, internal medicine physicians, or other medical services. The Physiotherapist (PT) will review the eligibility of the patient’s condition, and will evaluate the patient from all aspects; physical and psychological aspects including the previous history of any current illness, level of consciousness, respiratory condition, muscle strength, range of motion (ROM), functional status, bed and out of bed mobility. The Physical Therapist will then select a suitable intervention and will discuss it with the COVID-19 team.
PT Program for COVID-19 Patients & When to Start!
The assessments of COVID-19 patients should be complete before starting the EM, and the goals of the physical Rehabilitation program should be decided initially. It is also important to know the respiratory status and physical conditions of the patient and make sure that ventilation frequency, inspiration pressure (positive end-expiration pressure; mmH2O), Arterial blood gas values; PH, PaO2, PaCO2, PaO2/FiO2, and all vital signs (temperature, blood pressure, pulse, respiration rate, and oxygen saturation) are within normal limits. A quick check on the patient’s laboratory test results; C-reactive protein, white blood cells (WBC), Platelets counts, and hemoglobin level is also important.[37]. The first Rehabilitation step for those patients is usually started by having a fully present and past history of the patient before assessing the patient’s stability, and level of consciousness, Glasgow Coma Scale (GSC), and Richmond Agitation Sedation Scale (RASS). All this information should be available in the patient file and confirmed by the existing ICU Physicians and Nursing team. Assessing the patients’ attachments, joint range of motion (ROM), muscle power, and functional ability are very important to know patients’ functional ability. [38] The collaboration between the physiotherapist and respiratory therapists (RT) is very important in the ICU setting. However, The Saudi MOH [22] presented respiratory guidelines before starting the physical Rehabilitation program with COVID-19 patients (Table 2).
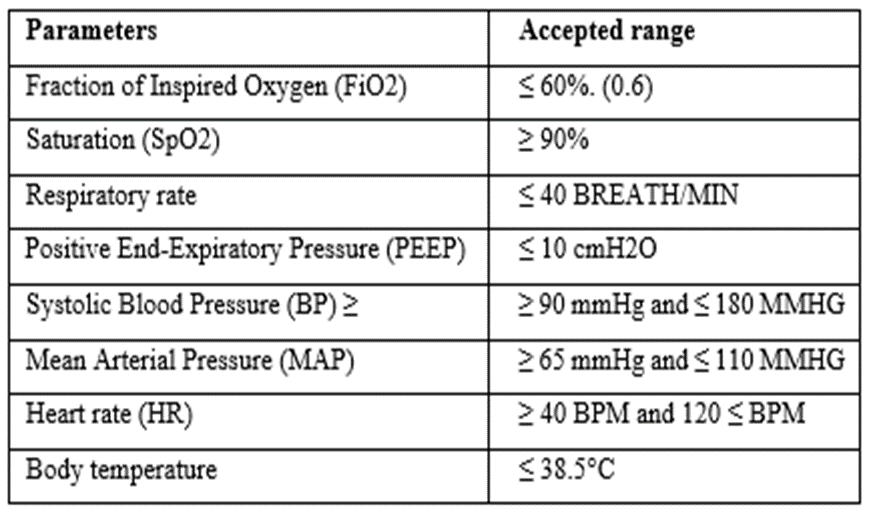
Table 2: Standard Respiratory Parameters before PT session. [17]
In KFSH&RC, the Critical Care Medicine Department, the Critical Care Nursing Department, and all clinical services divisions collaborated to implement EM attainment for COVID-19 patients from the initial phase of ICU admission, especially for severe COVID-19 conditions associated with hypoxia or pneumonia at different stages. The EM program for physical rehabilitation includes various exercise programs, starting with passive movement, active and active-assisted exercises, bed mobility, and out-of-bed mobility up to walking. This program is usually started immediately after the clinical stabilization of the patient's condition. At the King Faisal Specialist Hospital and Research Center, the harshness of the rehabilitation program for post-COVID-19 usually depends on the patient's condition, consciousness level, respiratory involvement, and COVID stages (See Figure 1).
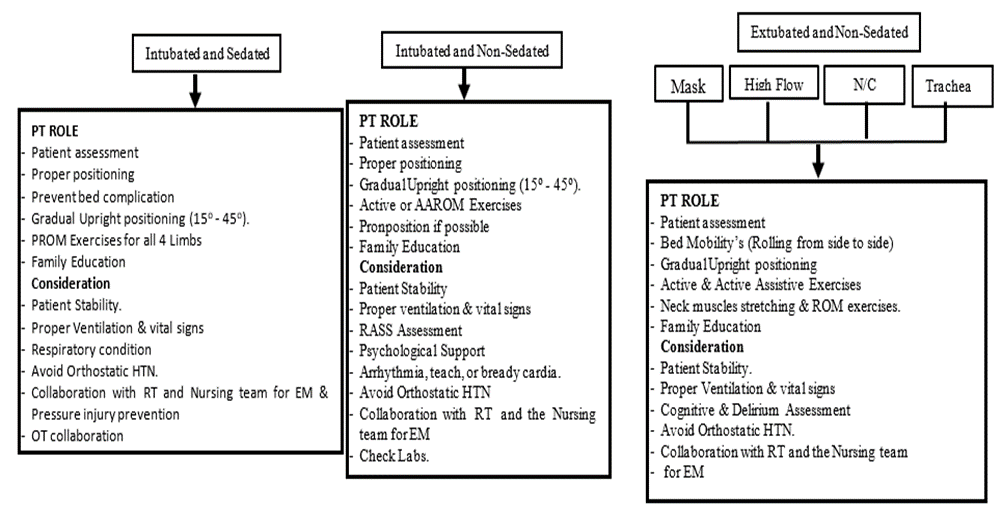
Figure 1: Strategies for implementing early mobilization in Acute & sub-acute COVID-19 patients
EM for Ventilated and Sedated Patients
Studies on early rehabilitation intervention for patients with COVID-19 have not reported any adverse events of early mobilization for mechanically ventilated patients (other than COVID-19) during deep sedation. Early mobilization, and exercises prescription for COVID-19 patients especially, sedated and intubated patients should involve careful consideration, and prescription parameters should depend on the current clinical situation of the patient. [39,40] In this stage, the patient will be admitted to the ICU. The EM program for sedated and ventilated patients should be started immediately after clinical stability is achieved, as confirmed by the COVID-19 team. [41] If the patient was under deep sedation or mechanically ventilated, the EM program might be limited to passive range of motion (PROM) exercises for both upper and lower limbs after appropriately assessing the ventilation mechanism. Proper postural exchange and gradually upright posture are necessary to be initiated as early as possible because patients are in the supine position most of the time. [34, 41, 42] This position may be changed increasingly to achieve an early sitting position to maintain good respiratory function based on lung protection, which is consistent with the treatment of acute respiratory distress syndrome, involving low tidal volume, low driving pressure, positive end-expiratory pressure, and long-term ventilator management. [43] Maintaining good ROM in all joints and preventing bed complications, such as bed sources is really important and the nursing team plays a significant role by turning the patient from side to side hourly. This early intervention for ventilated patients has been supported by several previous studies and reports. [34,41,43,44] Some unconscious or sedated critical COVID-19 patients’ studies recommended neuromuscular electrical stimulation (NES) [45] whereas other studies are not supporting applying “NES” to avoid any further muscle fibrosis injury. [46, 47] It is known that exercise programs are prescribed and supervised by physiotherapists [38,48,] therefore, bed positioning and ROM exercises could be initiated by PTs and then could be frequently done by the nursing team who are changing the patients’ positions regularly based on the patient’s clinical condition. [9, 49] Occupational Therapy (OT) services for COVID-19 patients are very important and recommended in this stage to confirm proximal and distal limb safety, especially during the sedation period when patients’ extremities position is in the wrong position or compressed against the patient’s body that could lead to nerve dysfunction. [37] OT therapists could also assess the need for splinting and may provide nursing staff or family members with the necessary education. One of the challenges in this stage is that the patients are not oriented due to sedation, the mechanical ventilation consequences, or due to other comorbidities such as heart and kidney problems, which may delay the early mobilization intervention. [32, 49]
EM for Ventilated and Off-Sedated Patients
In this phase, the patients will usually be in the ICU and could be either intubated/ventilated and/or with a tracheostomy, but without sedation. The first step in this stage is assessing the patient’s situation, physically and cognitively, and the therapist must clear the patient’s respiratory condition before starting the session. Certainly, Physiotherapists (PTs) in the ICU always work alongside Respiratory Therapists (RTs), nursing teams, and intensivists (ICU Physicians) to ensure proper ventilation and to avoid unexpected deterioration, respiratory complications, or any adverse reaction from early mobilization. The rehabilitation team should discuss the possibility of starting an active mobilization program as soon as patient sedation is reduced to avoid critical myopathy and physical disability. Assessing the patient's awareness or delirium is important as one of the most common symptoms among COVID-19 patients in the ICU especially amongst mechanically ventilated patients with an incidence ranging from 45% to 87%. [50, 51, 52] Delirium is an acute change in attention and awareness that develops over a relatively short time interval and is associated with additional cognitive deficits such as memory deficits, disorientation, or perceptual disturbances. [50] The EM program for COVID-19 in the ICU will depend on the awareness, delirium, and ability of the patient to follow verbal commands. Therefore, if the patient is off sedation but completely disoriented, with a high level of delirium or not responding to verbal commands, the program will be almost similar to the previous stage. This means that the exercise program will be more oriented to proper bed positioning, maintaining good ROM, preventing bed complications, and maintaining good ventilation and breathing patterns (see Figure 1). However, if the patient is attentive, oriented, and responds to verbal commands, the EM program will be more oriented toward active or active-assisted ROM exercises, bed mobility, frequent posture changes, and functional and balance training. [18, 53] However, the therapeutic approaches must be based on the patient’s clinical condition and can be stopped at any time if the therapist finds any serious deterioration in the patient's condition. [54]
EM for Extubated and Non-sedated Patients
This stage is important because the majority of the patients will be off sedation, but they might still be dependent on oxygen (O2) therapy, which could be through an O2 Mask, high flow, Nasal Cannula, or Tracheostomy. At this stage, patients are expected to be more responsive to the cardiac rehabilitation team, and the therapist may have the opportunity to push for activity and out-of-bed mobility. Thus, patient assessment is essential in this stage, with the aim of determining the level of stability, consciousness, and O2 demands, and the ability of the patients to perform advanced activities. In this stage, the CR program should include delirium assessment, breathing exercises, and the Active Cycle Breathing Technique (ACBT), which helps in clearing sputum from the airway. This technique involves a set of breathing exercises that loosen and move sputum from the airway and consists of breathing control, deep breathing, and huffing. As the patient improves, we could progress from the small-long huff technique that moves sputum from the low down of the chest to the big-short huff that moves sputum from higher up of the chest, taking into consideration the percentage of O2 saturation which should be > 90% during the exercise session. [55] Muscle power of the upper and lower limbs, hand grip, ROM, and functional mobility must also be assessed to determine the patient’s ability to properly initiate the exercise program. In addition to bed mobility encouragement such as circulatory exercise, ROM exercises, sitting at the edge of the bed, or sitting out on a chair should be initiated in this stage since patients will be more attentive and more responsive to the clinicians. [9] Physiotherapists in this stage may also need to collaborate with other clinical service members and the nursing team to achieve optimum goals.
When to interrupt the PT program for COVID patients?
The Saudi MOH guidelines [22] specified that Physical Rehabilitation sessions must be stopped during acute or subacute stages when the following situation occurs: a high intensity of fatigue and intolerance of physical activity of the patient, or when the patient is anxious or starts to have an arrhythmia or developing myocardial ischemia. When the resting heart rate was >120 BPM or the systolic blood pressure was <90> 180 mmHg. Sometimes, during the session, unsealing of the closed respiratory system may occur, and the clinician should stop the session immediately. The exercise session should also be interrupted when the blood oxygen saturation is < 90> 4% from the baseline, or when there is no synchronization between the patient and the ventilator machine. Exercise sessions should be stopped in cases of coexisting diseases that are unsuitable for exercise. [56]
EM Post-Acute Stage of CVID-19
At this stage, most patients have overcome the serious situation and are ready to be transferred to the post-acute units. However, patients may still have some COVID-19 symptoms, such as respiratory problems, O2 therapy dependence, and ICU-AW, and they may be dependent on functional motilities. Therefore, rehabilitation programs should be continued, and clinicians should resume working on deep breathing exercises, especially the Active Cycle of Breathing Techniques (ACBT), strengthening exercises, encouraging independent bed and out-of-bed mobility, AROM, strengthening exercises, and functional mobility. Considerations should be taken at this stage, including patient stability, proper ventilation, good vital signs, and delirium assessment. Avoiding Orthostatic HTN and collaborating with RT is important. In this stage, patient and family education about the clinical course of the disease and the estimated comorbidities are important. The EM exercise program should be progressively increased, depending on the patient’s ability and stability. In addition, encouraging patients to gradually move out of bed and take a few steps with the multidisciplinary team using a walking aid, if needed, is the main objective in this stage. In this stage family members' involvement in the treatment plan is advisable, and they could participate in some simple exercise program preparing them to deal with the patient after discharge home. [57] Considerations at this stage, such as proper ventilation, delirium assessment, and fall prevention, should be considered.
Home Discharge Planning and Rehabilitation Requirements
The discharge plan can help to limit any impact that may arise from any unprecedented situation for COVID-19 facilities to either home or long-term care facilities. Early discharge planning is very important after patients overcome acute stages and become clinically stable. This decision is usually made in collaboration with the COVID-19 and multidisciplinary teams. However, before discharge starts, COVID-19 patients need to regain most of their cardiorespiratory capacity by maintaining good oxygen saturation and performing good muscle-strengthening exercises. Though, some patients might be D/C with O2 support (home oxygen) thus, all the needed equipment must be prepared by the rehabilitation team including home assessments.[58] It has been reported that COVID-19 symptoms may persist for up to four weeks from the onset of symptoms to three months. Symptoms include myalgia, muscular dysfunction, sleep abnormalities, psychosocial alterations, pulmonary fibrosis, and reduced lung capacity. Therefore, before discharge, it is recommended to use the test-based strategy that includes resolution of fever without the use of fever-reducing medications, improvement in respiratory symptoms (cough, shortness of breath), and negative results of COVID-19 from at least two consecutive nasopharyngeal swabs specimens collected ≥24 hours apart (total of two negative specimens).[59] All equipment needed must be assessed and prepared by the COVID-19 Rehabilitation team, including home assessments. All COVID-19 patients must be provided with a home exercise program that includes breathing exercises (the ACBT technique), strengthening, and aerobic exercise programs such as bridging exercises, sideways leg lifts, and straight leg raises. From the sitting position, patients can perform seated knee extension, seated hip flexion, Sit-to-stand, Shoulder press using slight weight, and shoulder strengthening. From a standing position, the patient can perform the standing leg exercises using a chair, and then the patient can swing their legs back word and forward, and to the side alternatively. Patients may also add hip flexion and extension while exercising from a standing position. Patients are usually advised to start these exercises gradually with 10 repetitions on each side, with rest in between the sessions, and then progressively increase the repetition according to individual tolerance. [60] All these exercises must be reviewed by patients before D/C, and outpatient follow-up assessment is mandatory.
Out-Patient Rehabilitation Follow-Up for post-COVID-19
Studies have reported that the disabling effects of COVID-19 are typically complex and long-lasting. [61, 62] It is expected that outpatient multidisciplinary rehabilitation follow-up will need to continue for an extended period after discharge from inpatient rehabilitation.] The alteration in the quality-of-life post-COVID not only concerns hospitalized patients but also ambulatory patients who should not be neglected. Critically unwell patients with COVID-19 are likely to have rehabilitation needs during and after an acute illness. Herridge et al. [25] reported that many individuals recovering from COVID-19 might have health problems that extend beyond the acute infection stage. This study also revealed that limitations in function resulting from these problems may affect the physical, cognitive, and mental aspects of health and may have an important impact on work and social life. Consequently, COVID-19 patients have to undergo physical, respiratory, and functional independence assessments before starting the outpatient follow-up rehabilitation program. At this stage, attention must be paid to residual COVID-19 symptoms, such as residual muscle weakness, body fatigue, dyspnea and/or shortness of breath, and cognitive impairment, in addition to neurological sequelae. [63] The rehabilitation assessment of COVID-19 patients should include all aspects that remain post-discharge, such as cognitive impairments that range from problems with memory or attention deficits to difficulties with expression. Mental health impairments include anxiety, mood disorders such as depression, and Post-Traumatic Stress Disorder. All these problems need to be highlighted and supervised or self-directed physical exercises.[64] Rehabilitation for people experiencing severe problems or a protracted course of Post COVID-19 Condition most likely requires a person-centered, comprehensive, and multidisciplinary approach to interventions that are provided in close collaboration with primary health care and several medical specialties. During outpatient rehabilitation, patients may be seen by Physiotherapists, Occupational therapists, speech and language therapists, dietitians, and psychiatrists depending on their needs. Studies have reported that recovery from COVID-19 is time-consuming and varies from person to person. It can range from weeks to months. [63] It has been recognized that for some individuals, there may be an unacceptably high acute risk associated with starting a physical activity program or substantially increasing their level of activity; thus, pre-exercise screening and assessment tools are illustrated in Table 3. It is important to accept that it will take time to recover physically and psychologically. Several studies specified that the resources for the rehabilitation of COVID-19 recommended interventions for rehabilitation that include advice on the resumption of activities; breathing techniques; exercise therapy; psychological interventions; cognitive training; rehabilitation for communication and swallowing difficulties; and occupational rehabilitation.[65, 67] The recommended rehabilitation program will be tailored to the patient’s needs and depending on the pre-exercise screening outcomes. The rehabilitation program is illustrated more in Table 4.
| Required Screening and Assessment Tools | Justification |
| Family history of heart and other diseases | A risk is given if a 1st-degree family member has had a heart attack and was a male aged < 55> |
| Smoking history | A risk factor is assigned to smokers irrespective of how many cigarettes are smoked per day or if they have stopped smoking in the last 6 months |
| Increased BMI | A risk factor is assigned in either Stage 2 (self-report) or Stage 3 (measured) if the person has a BMI of 30 or greater |
| Vital signs (HR, BP, RR, SPO2) | Should be assessed before after and in between exercise sessions |
| Hypertension | A risk factor is given if the person has a resting systolic BP reading of >140 mmHg or resting diastolic BP reading of >90 mmHg (If both are greater, they have a maximum of one risk factor for BP) |
| Blood Glucose | R if they are taking medication to lower blood glucose. In Stage 3 a risk factor is given if the person has a fasting glucose level of 5.5 mmol/L or greater |
| High cholesterol | A risk factor is given if the person has a total cholesterol level of 5.2 mmol/L or greater. Or taking medication. |
| The current medications | Has to be reviewed and be sure that the patients are aware of their medications, and monitoring their adherence to taking them |
| Porge scale | Should be measured before the exercise prescription and before the end of the exercise program as an assessment tool to know the rate of preserved exertion. |
| Six min walk test | One of the important tests to be done before the exercise prescription is to know the pre-exercise functional capacity |
| Ejection Fraction | One of the tools that the clinician should be aware of is to build up the exercise intensity of the patients (mild, moderate, or maximum). |
| Muscle, bone, or joint pain or soreness | Must be measured to find out patients’ limitations and strengths. If the patient has pain in the muscles, bones, or joints, then the response is related to an acute problem, further medical guidance may be required. |
| Functional Ability | A risk factor is given if the person fails to meet 150 min/wk of weighted physical activity |
Cognitive Function & Psychosocial Well-being | Delirium monitoring is important to be assessed and managed before EM, exercise; and Family engagement too. Mental health such as anxiety and depression must be assessed also and the patient may need to follow up with Psychiatry or Psychosocial Services. |
Table 3: Screening and Assessment tools before outpatient Follow-up [64]
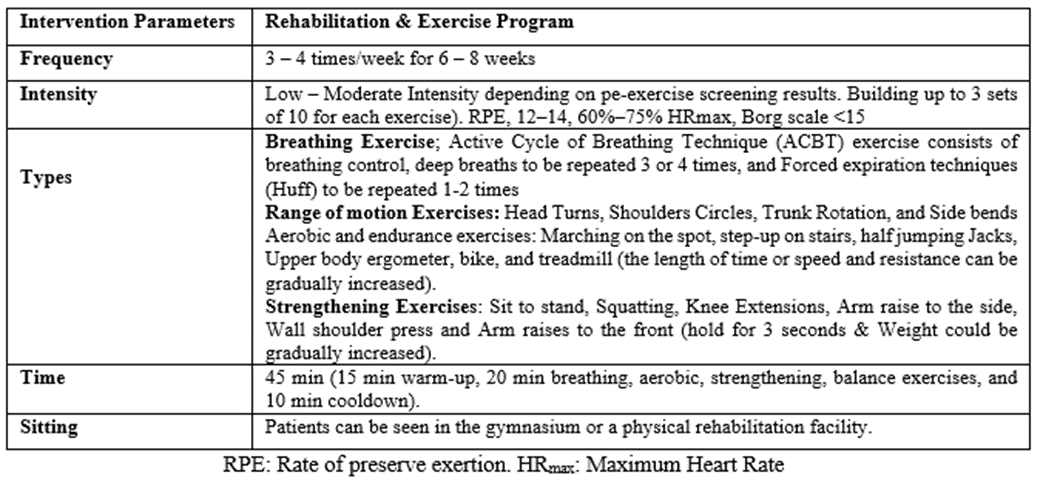
Table 4: The outpatient Rehabilitation program for post-COVID-19 patients. [68]
Tele-rehabilitation for post-COVID-19 in the KSA.
Early Physical Rehabilitation protocols have improved functional outcomes and reduced mortality rates. Virtual rehabilitation (VR) has allowed practitioners to provide safe treatment without the risk of viral contamination. Tele-rehabilitation was suggested as a clinical restoration administration with a focal point of assessment, finding, and treatment. This may significantly promote innovation in scientific discovery and learning opportunities. Telehealth is an expansive umbrella of modalities that incorporates clinical and non-clinical services. [69] For several reasons, virtual care sessions may be preferable to face-to-face contact post-COVID-19. However, it is a great option for patients with difficulties coming to a rehabilitation facility or who still have remaining symptoms. King Faisal Specialist Hospital and Research Center is one of the pioneers of Tele-Medicine, Mobile-Health, and Virtual Clinics. In addition, physical rehabilitation is one of the active departments in the clinical services section that utilizes this technology and gains the optimum advantage in serving COVID-19 and non-COVID-19 patients.
Although COVID-19 is a novel disease, rehabilitation providers routinely treat patients who experience disability due to critical illness and ARDS. All follow-up studies reported significant deficits, poor quality of life, limitations in physical functioning, and cognitive and mental health in post-acute COVID-19 patients. Studies have revealed that high-quality rehabilitation intervention is a key strategy to reduce the health impact of COVID-19, which plays a crucial role in bringing patients back to normal life, especially critically ill patients. In King Faisal Specialist Hospital, the multidisciplinary team approach and proper follow-up of Physical Rehabilitation, Occupational Therapy, Respiratory Therapy, and Nutrition, with the collaboration of the medical, nursing, and different clinical services divisions, is an integral part of the intervention designed to regain optimal physical function, psychological well-being, and better quality of life for post-COVID-19 patients.
All others contribute to the writing and reviewing equally. Mohammed Takroni, Abdulaziz Al-Thumayri: original draft and writing, Ms. Shiji Poulose, Ms. Sara Al—Eisa, Mohammed Al-Zahrani, Mohammed Ahmed, and Mohammed Takroni: review & editing.
The authors have no potential conflicts of interest to disclose for any of the authors listed in the article. This study did not require funding.
The authors would like to thank the COVID-19 team, all clinical services departments, respiratory therapists, and occupational therapists who worked side by side with the physical rehabilitation staff. Grateful thank the physical rehabilitation management for the prodigious support, and special thanks to Mrs. Shiji Poulose from the Critical Care Nursing Department for the tremendous guidance and support. The Digital Library Team for the remarkable help.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
