
Commentry | DOI: https://doi.org/10.31579/2694-0248/034
1Research Fellow, Department Orthopeadic Teaching Hospital Jaffna, Sri Lanka.
2Consultant Orthopaedic Surgeon Department Orthopeadic Teaching Hospital Jaffna, Sri Lanka.
*Corresponding Author: S.Thiruvarangan, Research Fellow Department Orthopeadic Teaching Hospital Jaffna Sri Lanka.
Citation: Thiruvarnagan S and Srigrishna P (2022). A Clinical Decision Making Pragmatic Approach for Lower Back Pain in the Clinical Context. J. Clinical Orthopedics and Trauma Care, 4(3); DOI:10.31579/2694-0248/034
Copyright: © 2022 S.Thiruvarangan, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 March 2022 | Accepted: 21 March 2022 | Published: 30 March 2022
Keywords: lower back pain; clinical decision-making; pragmatic approach; evidence-based practice
Lower back pain (LBP) is a collective musculoskeletal illness affecting the overall population although the frequency of back pain and dysfunction take place with aging. Earlier research suggests that LBP prevalence progressively increases with aging and its occurrence may be recognized as an occupational exposure among working-age adults in pain perception. This leads to tremendous strain in every nation as it represents one of the leading causes globally of growing disability and major socioeconomic burden in almost every healthcare system. Thus, an efficient back pain management strategy is an urgent priority given the alarming socioeconomic burden of this musculoskeletal disorder for nearly all healthcare providers globally.
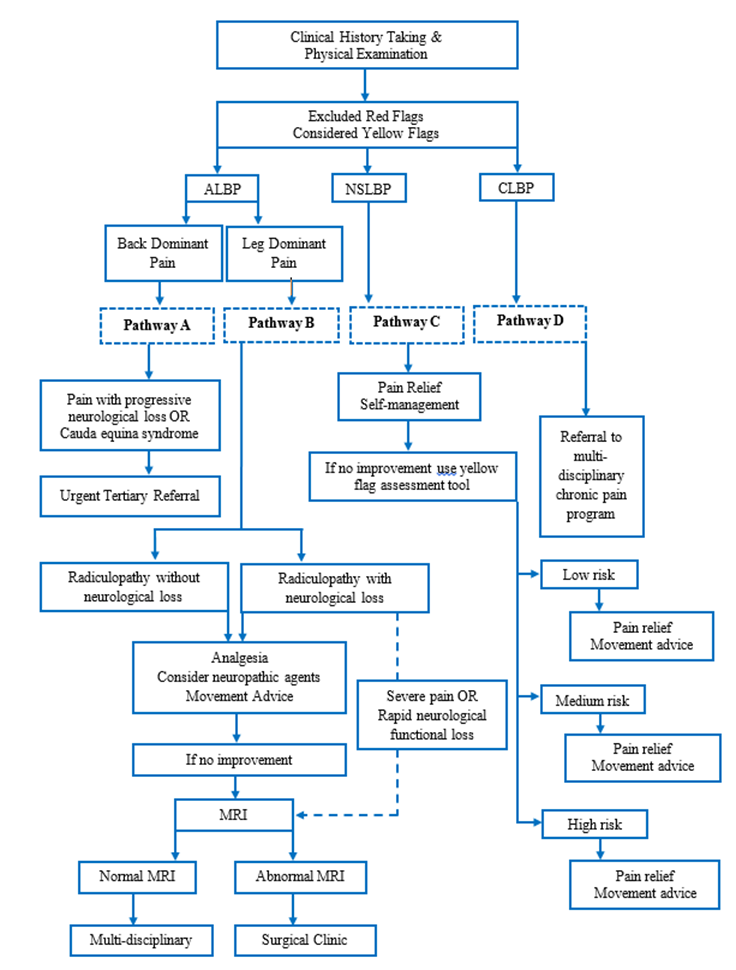
Low back pain (LBP) is the most common health problem and remains a global issue in every population. This common condition affecting many individuals at some point in their lives and incidences of LBP progressively increase with occupational exposure among working-age adults and age-related changes in community dwelling seniors [1]. The recent studies study estimated that approximately 97% of people experience back pain at any one time in their life while around 62% is mechanical nature or non-specific (NSLBP) but between 5% and 10% of cases develops chronic low back pain (CLBP) then it is likely to be the primary focus on seeking health care services [2]. In population-based studies, the 1-year prevalence of LBP ranged from 13 to 50% worldwide, up to 80% of back pain patients suffering in long-term and one-third of these cases are often inadequately treated [3]. The differential diagnosis is very important in acute cases (ALBP) because it has a wider-range of underlying pathological causes and it is an essential to have precise differential diagnosis to reach potential positive prognostic value and higher quality of patient care and safety. According to the Global Burden of Disease Study evaluation revealed that low back pain accountable for many years patient lived with disability, the back pain represents one of the leading causes globally for growing number of disability and major socioeconomic burden in almost every healthcare system. This musculoskeletal disorder potentially impacts on a person’s quality of life, work absence and leads to long-term disability subsequently dependency of activity of livings and developing huge socio-economic burden in worldwide [4]. A number of study findings reveal that lower back pain has a wider-range of potential etiologies and the back pain symptomatology can be overlap each other also depend on the patient population but among the mechanical nature and non-specific causes are most common. However, successful outcomes of lower back pain are dependent on precise differential diagnosis. It can be reached by detailed clinical history taking, knowledge of the regional anatomy, precise understanding of the pathology comprehensive physical examination and diagnostic studies [5]. A number of clinical guidelines show that potential success of conservative management for lower back pain approximately 70% although in certain cases surgical intervention is required [6]. Thus, the efficient back pain diagnostic triage is an urgent priority as the alarming rate of socioeconomic burden of musculoskeletal disorders for nearly all healthcare service providers in every nation in worldwide. This paper aims to provide a lower back pain algorithm for clinicians, who have potential diagnostic responsibilities in making clinical-decision on lower back pain.
Clinical Presentation
The increasing chronic lower back pain disorder is a global challenge. This leads to tremendous strain on health care services as they need to address rising numbers of patients with conditions that largely cause disability. There are some type of pain can be understood straightforwardly because there is a clear structural damage such as a cut or a bruise of skin but some pain mechanism is less obvious like chronic lower back pain. The lower back pain is classified as acute when it persists for up to 6 weeks period and it is considered as sub-acute when it is prolonged for up to 3 months. If the pain is persisted beyond 3 months that commonly requires to natural healing time it is considered as chronic lower back pain and has a huge negative impact on the lives of number of people [7]. The acute lower back pain is often
occurred as the result of tissue injuries and patients suffer from acute back pain are less likely to seek medical care because acute pain gets better on their own or with appropriate treatment. However, the chronic pain is associated with health care cost and burden has been reported across health care systems globally. The back pain is usually described as localized pain, muscle tension and/or stiffness below the costal margin and above the inferior gluteal folds with or without leg symptoms (sciatica). The common symptoms of non-specific low back pain are pain and functional [8]. The diagnosis and treatment for patients with low back pain have variation within and between country’s clinical practice guidelines.
Clinical diagnosis
The clinical history taking and comprehensive physical examination are the first and most important in the evaluation process of lower back pain to help narrow down the diagnosis. The goal of diagnosis in lower back pain is to describe the root causative factor of anatomic pain unambiguously as possible also focusing on carefully defined clinical subgroups with the
understanding [9]. However, this is not always likely classified. This is essential to careful structure of clinical questions, active listening to the answers and mapping out the location of the pain. The key area in the medical history taking helps to identify the present pain location and any changes since its onset [10]. Also it is needed to find out easing and aggravating of pain factors because these are important keys to arrive a precise differential diagnosis. For example, a back pain associated with herniated disc would be painful on sitting and better on standing or lying in comparison, a patient with lumbar canal stenosis would feel better on sitting while he suffers when he walks (neural claudication). Moreover, patients with facet joint degenerative changes and muscle sprains would be relieved when lying down [11]. At this point, it is essential to the treating clinician to clear understanding on the difference between radicular and referred pain. However, if pain does not fit any known diagnostic profile of a clinical picture, there may be other factors that interfere with diagnosis and recovery that need to be addressed.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
