
Case Report | DOI: https://doi.org/10.31579/2578-8949/091
Department of Dermatology, University Hospital Hassan II, Fès, Morocco.
*Corresponding Author: Mrabat Samia, Department of Dermatology, University Hospital Hassan II, Fès, Morocco
Citation: Mrabat Samia, Laamari Kaoutar , Douhi Zakia, Elloudi Sara, Baybay Hanane, Mernissi Fatima Zahra, A Chronic Inguinal Intertrigo Revealing Inverse Psoriasis J.Dermatology and Dermatitis . 4(2);DOI:10.31579/2578-8949/091
Copyright: © 2019 Mrabat Samia, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 October 2019 | Accepted: 20 October 2019 | Published: 25 October 2019
Keywords: psoriasis ; intertrigo ; inverse ; folds.
Plaque psoriasis is typically localized to extensor surfaces of the skin, whereas inverse psoriasis is defined by its localization to intertriginous areas where two skin surfaces meet. It can be localized to the axillae, groin, genital area, umbilicus, postauricular area, intergluteal, antecubital and popliteal fossae.
The lesions are well demarcated with less or no scaling compared to classical plaque-type psoriasis [1,2]. We report a case af inverse psoriasis that had been mistaken for a mycotic intertrigo.
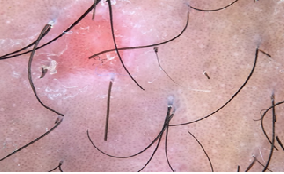
A 38 years old woman presented with a localized inguinal pruritus evolving for three years, the patient had already received local and oral antimycotic treatment with no improvement. The clinical examination found a well limited unilateral inguinal intertrigo, dermoscopy showed scales with regularly distributed, dotted vessels on a light red background. The rest of the skin examination, nails and scalp showed no abnormalities.The patient was then treated with topical corticosteroid with great improvement.

Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
