
Case report | DOI: https://doi.org/10.31579/2578-8868/314
1 Department of Neurosurgery, Sichuan Mianyang 404 Hospital, Mianyang, 621000, Sichuan, China.
2 Department of Neurosurgery, Affiliated Hospital of Southwest Medical University, Luzhou, 646000, Sichuan, China.
3 Department of Neurosurgery, Sichuan Mianyang 404 Hospital, Mianyang, 621000, Sichuan, China.
4 Department of Neurosurgery, Sichuan Mianyang 404 Hospital, Mianyang, 621000, Sichuan, China.
5 Department of Neurosurgery, Sichuan Mianyang 404 Hospital, Mianyang, 621000, Sichuan, China.
6 Department of Neurosurgery, Sichuan Mianyang 404 Hospital, Mianyang, 621000, Sichuan, China.
*Corresponding Author: Zhengfang Jiang, Department of Neurosurgery, Sichuan Mianyang 404 Hospital, Mianyang, 621000, Sichuan, China.
Citation: Zhengfang Jiang, Qiang Li, Lingyong Zeng, Chenglang Xu and Chengrui Tan, (2024), A chronic encapsulated expanding hematoma that developed 20 years after gamma knife surgery for a cerebral epilepsy, J. Neuroscience and Neurological Surgery, 16(1) ; DOI :10.31579/2578-8868/314
Copyright: © 2024, Zhengfang Jiang. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 17 April 2024 | Accepted: 08 July 2024 | Published: 02 August 2024
Keywords: chronic encapsulated expanding hematoma ; gamma knife surgery ; epilepsy
Background: We report a patient diagnosed with epilepsy 20 years ago who developed a chronic encapsulated expanding hematoma after gamma knife surgery.
Case presentation: A 49-year-old middle-aged female was admitted to our department due to headaches accompanied by left-sided limb weakness for 2 months. Cranial computed tomography (CT) and magnetic resonance imaging (MRI) scans revealed a giant cystic-solid mass in the right frontal-temporal lobe, accompanied by compression and edema of the surrounding brain parenchyma. After completion of relevant preoperative examinations upon admission, she underwent microsurgical evacuation of the chronic encapsulated expanding intracerebral hematoma. Postoperatively, the patient improved and recovered well.
Conclusion: Chronic encapsulated expanding hematoma is a rare complication after gamma knife surgery therapy. It's essential for individuals experiencing symptoms or complications related to a hematoma to seek medical attention for proper evaluation and management.
A chronic encapsulated expanding hematoma refers to a condition where blood accumulates within tissues, typically due to trauma or injury, and forms a contained mass surrounded by a fibrous capsule [1, 2]. Over time, this hematoma continues to expand within its capsule, leading to persistent symptoms such as pain, swelling, and potentially compression of nearby structures. Treatment usually involves surgical intervention to remove the hematoma and repair any damaged tissues. If left untreated, chronic encapsulated expanding hematomas can result in complications and further tissue damage [3]. We report on a patient who developed a chronic encapsulated expanding hematoma after Gamma Knife surgery and underwent microsurgery to remove a chronic encapsulated expanding hematoma.
A 49-year-old middle-aged woman presented to our hospital for treatment with headache and left limb weakness for 2 months. 20 years ago, the patient underwent gamma knife surgery for cerebral epilepsy, and since then the patient had no further seizures. Two months before the presentation, the patient had headache and left limb weakness without obvious cause. Computed tomography (CT) imaging revealed a giant low-density cystic lesion in the right frontal-temporal lobe (Figure 1a). Further magnetic resonance imaging (MRI) showed low and hyperintense on T1 and T2-weighted imaging, respectively(Figure 1b and c),No significant enhancement was seen after the enhancement scan(Figure 1d).After a series of preoperative examination, we decided to use microscopic chronic dilated brain hematoma removal, intraoperative found brain tissue pressure increased significantly, cerebral cortex vascular hyperplasia tortuous, lesions around the brain tissue tough, pale yellow, surface of tortuous necrotic blood vessels, we thoroughly suck blood clot, removal of abnormal brain tissue and blood vessels, complete hemostasis, using sterile saline rinse to clear, eventually brain tissue collapse is good. The postoperative CT showed that the hematoma had been emptied and the patient's symptoms were significantly improved (Figure 1e). Following half-year postoperative review, a cranial CT scan demonstrated no recurrence of intracranial hematoma in the patien (Figure 1f).The pathological results suggested that The perivascular inflammatory cells were mainly lymphocytes, and a little local bleeding with hemosiderin depositionl (Figure 2).
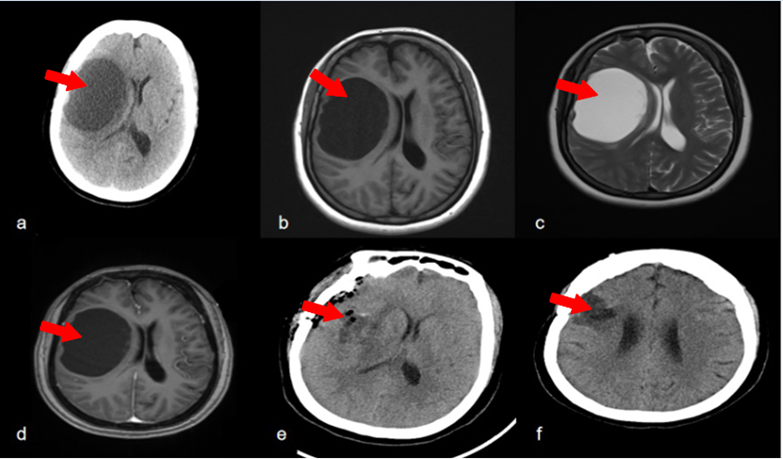
Figure 1: (a) Twenty years of computed tomography (CT) after gamma knife surgery treatment for epilepsy showed a giant cyst in the right frontotemporal lobe.(b) Preoperative magnetic resonance imaging (MRI) showed a cystic lesion in the right frontotemporal lobe appearing isointense on T1-weighted imaging and (c) hyperintense on T2-weighted. (d) No significant enhancement was seen after the enhancement scan. (e) The postoperative CT showed that the hematoma had been emptied. (f) CT scan half year after surgery showed no recurrence of hematoma.
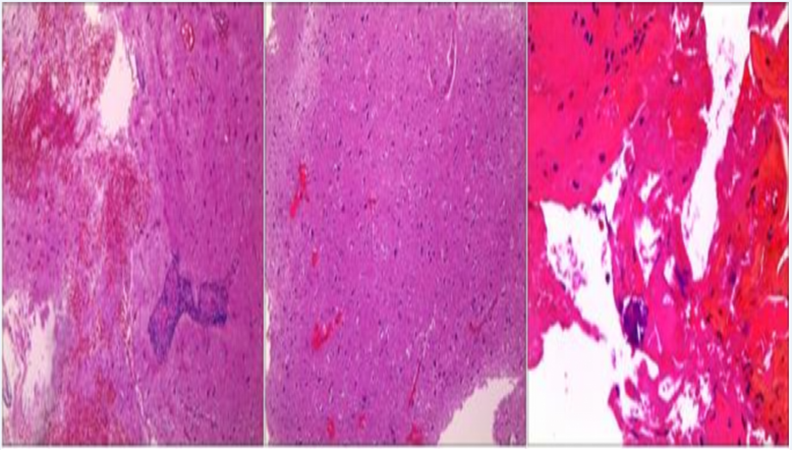
Figure 2: Histopathological results showed that the cerebral tissue sent for examination was vasodilated and hyperemic, with hemosiderin deposition, and the perivascular inflammatory cells were mainly lymphocytes.
Chronic encapsulated expanding hematoma refers to a rare but potentially serious complication that can occur following various surgical procedures or traumatic injuries [4]. This condition involves the formation of a hematoma, or a localized collection of blood, which becomes encapsulated within surrounding tissues over time. As the hematoma continues to expand within its encapsulated space, it can exert pressure on adjacent structures, leading to symptoms such as pain, neurological deficits, or tissue ischemia.
One of the key points for discussion regarding chronic encapsulated expanding hematoma is its pathophysiology. While the exact mechanisms underlying its development are not fully understood, several factors may contribute to its formation. These include inadequate hemostasis during surgery, disruption of blood vessels, foreign body reactions to surgical materials, or impaired wound healing processes [5-6]. Additionally, the presence of comorbidities such as coagulopathies or systemic diseases may predispose individuals to this complication.
Clinical manifestations of chronic encapsulated expanding hematoma can vary depending on its location and size. Patients may present with nonspecific symptoms initially, such as swelling, discomfort, or localized warmth at the surgical site. However, as the hematoma enlarges and compresses surrounding tissues, more severe symptoms may develop, including neurological deficits or compromised blood flow to adjacent structures. The diagnosis of chronic encapsulated expanding hematoma typically relies on imaging studies, such as ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI). These modalities can accurately delineate the extent and characteristics of the hematoma, as well as assess its impact on nearby anatomical structures [7]. Additionally, laboratory tests may be performed to evaluate for associated coagulopathies or other systemic abnormalities.
Management of chronic encapsulated expanding hematoma often involves a multidisciplinary approach, incorporating surgical intervention, pharmacological therapy, and supportive care measures. Surgical evacuation of the hematoma may be necessary to relieve pressure on surrounding tissues and alleviate symptoms [2,8]. In cases where surgical intervention is not feasible or contraindicated, conservative management strategies such as compression therapy or anticoagulation may be considered. Close monitoring of patients following treatment is essential to assess for recurrence or complications [2,9-10].
In conclusion, chronic encapsulated expanding hematoma represents a rare but potentially serious complication that can arise following surgical procedures or traumatic injuries. Understanding its pathophysiology, clinical presentation, diagnostic approach, and management strategies is crucial for healthcare providers to promptly recognize and effectively manage this condition, thereby optimizing patient outcomes and minimizing morbidity [11-12]. Further research is warranted to elucidate the underlying mechanisms and refine therapeutic strategies for this challenging clinical entity.
Chronic encapsulated expanding hematoma is a rare complication of gamma knife surgery for epilepsy. It emphasizes the need for prompt surgical intervention to remove the hematoma when patients develop clinical symptoms, and close postoperative follow-up monitoring is essential.
The research was approved by the ethics committee of the Sichuan Mianyang 404 Hospital. We have obtained informed consent from all family members of patients of this case report.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Not applicable.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This research was funded by the Sichuan Science and Technology Program of China (2017JY0035), and Mianyang Science and Technology Plan Project(16S-01-4).
Qiang Li analyzed the results and completed the manuscript. Miao Yuan assisted with editing and discussion points. Chenglang Xu and Chengrui Tan assisted with image selection and description. Lingyong Zeng revised the manuscript. Zhengfang Jiang conceived this study. All authors have read and agreed to the published version of the manuscript.
Not applicable.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
