
Case Report | DOI: https://doi.org/10.31579/2690-8794/117
1 Bindu’s Curative Clinic, Chheda nagar, Near Harihareshwar temple, Nallasopara west, Palghar- 401203, Maharashtra, India.
*Corresponding Author: Bindulata Maurya, Bindu’s Curative Clinic, Chheda nagar, Near Harihareshwar temple, Nallasopara west, Palghar- 401203, Maharashtra, India.
Citation: Bindulata Maurya, Miteshkumar Maurya (2022) A Case Report of Psoriatic Arthritis and Homoeopathic Remedial Approach, J, Clinical Medical Reviews and Reports. 4(3); DOI: 10.31579/2690-8794/117
Copyright: © 2022, Bindulata Maurya, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 November 2021 | Accepted: 14 December 2021 | Published: 07 January 2022
Keywords: homoeopathy, psoriasis, arthritis, atopic dermatitis, alternative therapy
With the advent of biologic agents in past few years, treatment armamentarium for psoriasis has largely enhanced. Each biologics has their own pros and cons with confusion over the preferred treatment for individual cases. With increase in research in psoriasis, there has been better upgradation in understanding about the pathogenesis of inflammatory psoriatic pathways with dominant interleukins IL-23/IL-17 axis involvement. Our case report begins with introduction about the psoriatic skin and joint disease with its pathophysiology and available treatments followed by the case description of adult male who was initially misdiagnosed as atopic dermatitis later confirmed to be psoriatic arthritis by rheumatologist. There was resolution of symptom after the homoeopathic treatment was started. This case report emphasizes the role of alternative therapy of medicine homoeopathy in treatment of chronic psoriatic skin and joint disease.
Psoriasis is a chronic inflammatory skin disease with strong genetic predisposition and autoimmune pathogenic traits. The global prevalence of Psoriasis is about 2% but lower prevalence in Asian and some African populations and up to 11% in Caucasian and Scandinavian populations. The pathognomic features of psoriasis is sustained inflammation leading to uncontrolled keratinocyte proliferation and differentiation while the histology reveals inflammatory infiltrates containing dermal dendritic cells, macrophages, T cells, and neutrophils [1]. Inflammatory Cytokines such as as TNF-α, IL-17 or IL-23 are implicated in the pathophysiology of the Psoriasis and can lead to synovitis, enthesitis, axial inflammation, and altered bone homeostasis as observed in psoriatic arthritis hence remains the cornerstone target for its treatment [2, 3, 4]. Mainstay therapy for psoriasis includes 11 US FDA approved biologic options till date with many in the pipeline. These includes biologic agents along with their year of US FDA approval: Tumor necrosis factor alpha inhibitors such as Adalimumab [2002], Entanercept [2004], Infliximab [2006], Certolizumab pegol [2008], Interleukin-17 [IL-17] inhibitors such as secukinumab [2015], brodalumab [2017], Ixekizumab [2017], Interleukin-23 [IL-23] inhibitors Guselkumab [2017], Tildrakizumab [2018], Risankizumab [2019] , IL12/23 inhibitor such as Ustekinumab [2009] but individual response to treatment may vary across different population ethnicity. [2] Moreover, the symptom of psoriatic arthritis are often misdiagnosed with atopic dermatitis. Diagnostic criteria of psoriatic arthritis is based on most commonly used ClASsification for Psoriatic ARthritis (CASPAR) Criteria [5, 6].
Patient information
A 33-year-old adult male medical professional resident of Palghar, hailing from state Uttar Pradesh, India reported to dermatology OPD at tertiary care referral hospital on 1st of January 2021 with chief complaints of maculo-papular and hyperkeratotic skin eruptions over both hands with involvement of fingers [extremities] affecting mainly the knuckles [Figure 1.] and ulnar aspect of both hands since 30th of December 2021. The symptom was associated with scaling of skin over elbows of both hands. All these skin lesions were itchy in nature exacerbated during evening hours and consumption of fatty meal. Mild itching over dorsum aspect of toes and phalanges involving both lower limbs. Patient observed and also reported about the flexion deformity of left little finger at distal interphalangeal joint [Figure 2.] since 01st January 2021. The other fingers had no deformity and were absolutely normal in structure and anatomy. There was no history of trauma to both hands and fingers [extremities]. Neither there were any skin eruptions/lesions in finger web spaces thus ruling out the possibility of scabies infestation. Patient has history of seasonal bronchial asthma and allergic rhinitis since 15 years of age. Patient had one episode of bronchial asthma on October 2020 managed by Homoeopathic treatment. Patient also history of seborrheic dermatitis of scalp almost 10 years back. There was no history of wearing gloves in past 6 months nor there any past history of allergy to latex hand gloves. No history of any insect bite [except mosquito bites] or contact with vegetation. No history of any drug allergy or substance abuse. Patient attributed the skin eruptions to use of poor quality sanitizers. Patient has already self-medicated himself with Permethrin lotion for local application thinking of scabies parasitic infestations. Patient often takes tablet cetirizine or levocetrizine 5 mg for his allergic rhinitis symptom or homeopathic remedy whenever there is bronchospasm episode usually exacerbated due to seasonal change.


Clinical findings & Diagnostic assessment
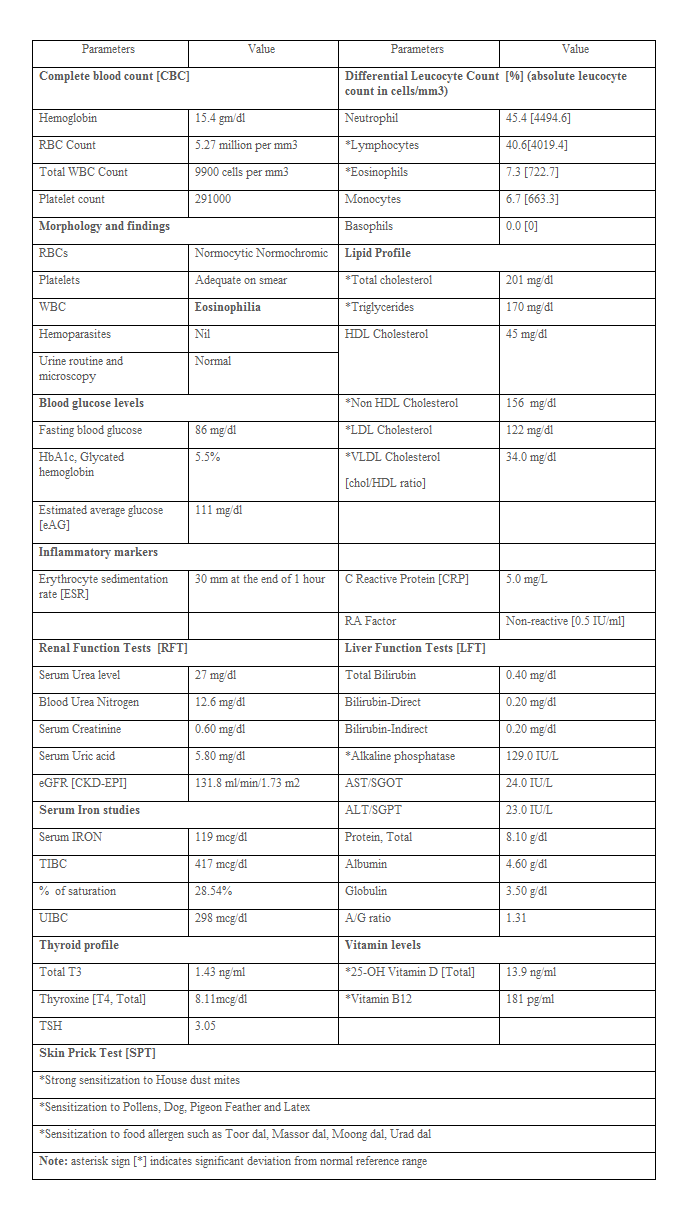
After careful assessment by dermatologists on 1st January 2021, patient was diagnosed with atopic dermatitis. No biopsy of skin lesion was performed. However, there was concern about the left little finger flexion deformity at distal interphalangeal joint [DIP] joints for which patient was referred to orthopedics. Orthopedic doctor advised for complete blood investigations [Table 1.] and roentgenogram [X ray] for left little finger-anteroposterior and lateral view. Blood investigation done on 6th February 2021 revealed low Vitamin D3 and Vitamin B12 levels with other parameters not clinical significant [Table 1.]. Chest X ray of left little finger did not reveal any bony erosions or fracture, so was referred to rheumatologist for further evaluation of left little finger flexion deformity. Rheumatologist diagnosed it as psoriatic arthritis, a manifestation of psoriasis that may affect wrist, metacarpophalangeal [MCP] joint, middle interphalangeal [MIP] joint, mainly affecting distal interphalangeal joint [DIP] to start with. Even skin prick test done by the allergy specialist revealed strong sensitivity to house dust mites [Table 1.]. According to the Classification Criteria for Psoriatic Arthritis (CASPAR) [5, 6], the patient had history of seborrheic psoriasis of scalp in the past [score 1], has current active psoriatic lesion at the elbow joint [score 2], dactylitis present [score 1] and was rheumatoid factor was negative [score 1] assigning total score of 5 thus confirming established inflammatory articular disease of psoriatic arthritis. However, there was no family history of psoriasis, no Juxta-articular new-bone formation on X-ray and no sign of nail dystrophy.
Therapeutic Intervention
On 1st January 2021, Dermatologist advised Tablet Levocetrizine 5 mg twice daily, Venusia derm cream and Mometasone steroidal cream for local application over affected sites on skin for 7 days as treatment for atopic dermatitis. Patient reported on 3rd of February 2021 to dermatologist for non-resolving skin lesions with hyperpigmentation with hyperkeratosis over the knuckles with fissuring. Erythema and excoriations present all over extensors of both forearms and hands. Bilateral elbow scaling was present. The patient was advised for Injection Triamcilinone 40 mg/ml stat intramuscular dose, Tablet Fluconazole 400 mg stat, Tab Levocetrizine 5 mg twice daily, Tablet Hydroxyzine 25 mg on SOS basis, Cerasoft cream thrice daily with Fluticatososne E cream for local application for 2 weeks, Fusidic cream local application over the fissured area on knuckles. Patient was started on intramuscular doses of injection methylcobalamin and Vitamin D3 alternate days for 5 days followed by two doses weekly for month along with oral supplementation with Calcium and Vitamin D3 tablets. Patient preferred taking homoeopathic consultation for psoriatic arthritis in view of non-resolving skin lesions. On the basis of symptom similarity, the patient was treated with homoeopathic medicine named Psorinum 1m, 4 pills stat dose prescribed along with Cosmos 30, 4 pills three times a day. Psorinum 1m was repeated as and when required.
Follow up & Outcomes
After treatment patient observed resolving skin lesions in two-three days. There was drastic healing of skin lesions over both hands and fingers [Figure 3.] with reduction in mild swelling at distal interphalangeal joints. Itching also resolved. Scaly skin lesions over elbows disappeared. Still there is persistence of left little finger deformity with mild hyperkerartotic healing psoriatic skin lesion at knuckles with hypopigmented spots over skin [Figure 4.]. Patients reports better results than before and was satisfied by the treatment.


It is difficult for clinicians to diagnose psoriatic arthritis in first instance and requires expertise in the field of autoimmune disorders. None of the treatment allopathic remedy available guarantee complete recovery. Homoeoptahic remedies work excellent in cases of chronic diseases and also autoimmiune disorders such as asthma, vitiligo, chronic skin diseases, and rheumatoid arthritis with lesser adverse effects. With good results/response, alternative system of medicine homoeopathy is gaining its importance with better patient reported outcomes. Witt CM et al designed prospective multicentre observational questionnaire based study over two years that revealed improvement in symptoms and health-related quality of life (QoL) in patient with psoriasis [7]. A case series published by Mahesh S. et al demonstrated that the classical homeopathy can heal psoriasis and its complications beyond skin care providing better wellbeing explained on the basis of the theory of "Levels of Health."[8]. Perez chada LM et al study reported other comorbidities when associated with psoriatic arthritis may be associated with poor clinical outcome hence require careful monitoring at early stage [9].
Psoriatic arthritis is often misdiagnosed. Homeopathic remedy works better in cases of psoriatic skin lesion and psoriatic arthritis if diagnosed appropriately by the physicians. However homoeopathic physicians should venture clinical trials with their treatment modalities to establish better evidence and recognition in par with allopathic system of medicine.
Written informed consent was obtained from the patient for publication of this case report.
The authors declare no competing interest.
CARE guidelines are followed to report our Case Report.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
