
Case Reports | DOI: https://doi.org/10.31579/2640-1045/044
1* Department of Endocrinology, Salmanyia Medical Complex, Ministry of Health, Bahrain.
2 Department of Internal Medicine, Salmaniya Medical Complex, Manama, Bahrain.
3 Department of Internal Medicine, Salmaniya Medical Complex, Manama, Bahrain.
4 Department of Pathology, Salmaniya Medical Complex, Manama, Bahrain.
5 Department of Internal Medicine, Salmaniya Medical Complex, Manama, Bahrain.
6 Department of Internal Medicine, Salmaniya Medical Complex, Manama, Bahrain.
*Corresponding Author: Husain Taha Radhi, Department of Endocrinology, Salmanyia Medical Complex, Ministry of Health, Bahrain.
Citation: Husain TR., Rawdha F., Aysha AS., Eman AJ., Riyadh A., and Hasan FA., (2019) Case Report of Cortisol-Secreating Adrenal Adenoma Causing Cushing Syndrome. J Endocrinology and Disorders. 3(1): Doi:10.31579/2640-1045/044
Copyright: © 2019 Husain TR. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 September 2019 | Accepted: 09 October 2019 | Published: 14 October 2019
Keywords: Cushing syndrome; Adrenal Adenoma; hypercortisolism
Cushing syndrome is a state of prolonged exposure to excess cortisol production. Causes can be varied ranging from exogenous intake or endogenous production from a pituitary source due to overproduction of adrenocorticotropic hormone (ACTH) or due to over secretion from unilateral or bilateral adrenal glands.
Cushing syndrome in an adult can present with proximal muscle weakness, facial plethora, wasting of the extremities with increased fat in the abdomen and face, wide purplish striae, bruising with no obvious trauma, and supraclavicular fat pads.
Here, we report a 38 year old male who presented with suspicion of having Cushing syndrome due to his clinical manifestations and high cortisol levels. He presented to the clinic with new onset diabetes, severe hypertension, chronic abdominal pain and distension which was being investigating by different specialties. The patient underwent CT scan of the abdomen which show right adrenal adenoma and on examination, he was found to have proximal weakness and purple striae. Laboratory data showed high morning cortisol, 24 urine free cortisol and ACTH levels which were strongly suggestive of ACTH independent Cushing syndrome.
Cushing syndrome is a condition resulting from chronic overproduction of glucocorticoid (1) therefore the signs and symptoms depend on the duration and intensity of excess steroid production (2) which lead to multisystem manifestations due to overproduction of the hormone.
The clinical manifestations can be categorized as reproductive, dermatologic, metabolic, cardiovascular, musculoskeletal, neuropsychiatric, and infectious (3-5). In addition to the considerable morbidity caused by hypercortisolism, there is also an increase in mortality rates.
The source of increased glucocorticoids can be exogenous due to chronic administration of corticosteroids for any underlying inflammatory condition or endogenous source which can be ACTH dependent or ACTH independent (6).
Pituitary ACTH-dependent Cushing's disease is five to six times more common than Cushing's syndrome caused by benign and malignant adrenal tumours combined (7). Thus, the incidence of Cushing's disease may be 5 to 25 per million per year. However, the reported incidences was much lower (1.2 to 2.4 per million per year) in one population-based study (8, 9). In a United States study, the incidences were higher than previously reported in European studies as it was found to affect 6.2 to 7.6 per million person-years (10).
Cushing syndrome due to adrenal adenoma is rare condition, but it is associated with high mortality rates if left untreated particularly from cardiovascular disease (3). However, median survival from cures was still excellent according to (cohort study) of patients who had been cured of hypercortisolism for at least 10 years at study (11).
A 38-year-old male attended the endocrine clinic with history of chronic abdominal pain, recent onset Diabetes Mellitus and severe uncontrolled hypertension despite being on treatment (Table 4).
Patient had previously visited several clinics and hospitals with the complaint of abdominal pain and distension which had been present for 3 years. His symptoms also included chronic fatigue, acne and the findings on the clinical examination demonstrated central obesity, proximal weakness, moon face, plethora, skin thinning, fat pads and purple striae (Figure 5-12).
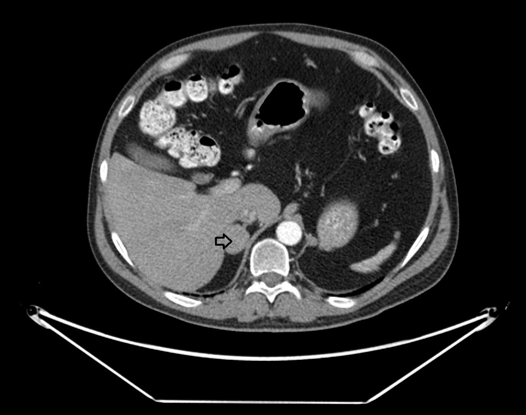
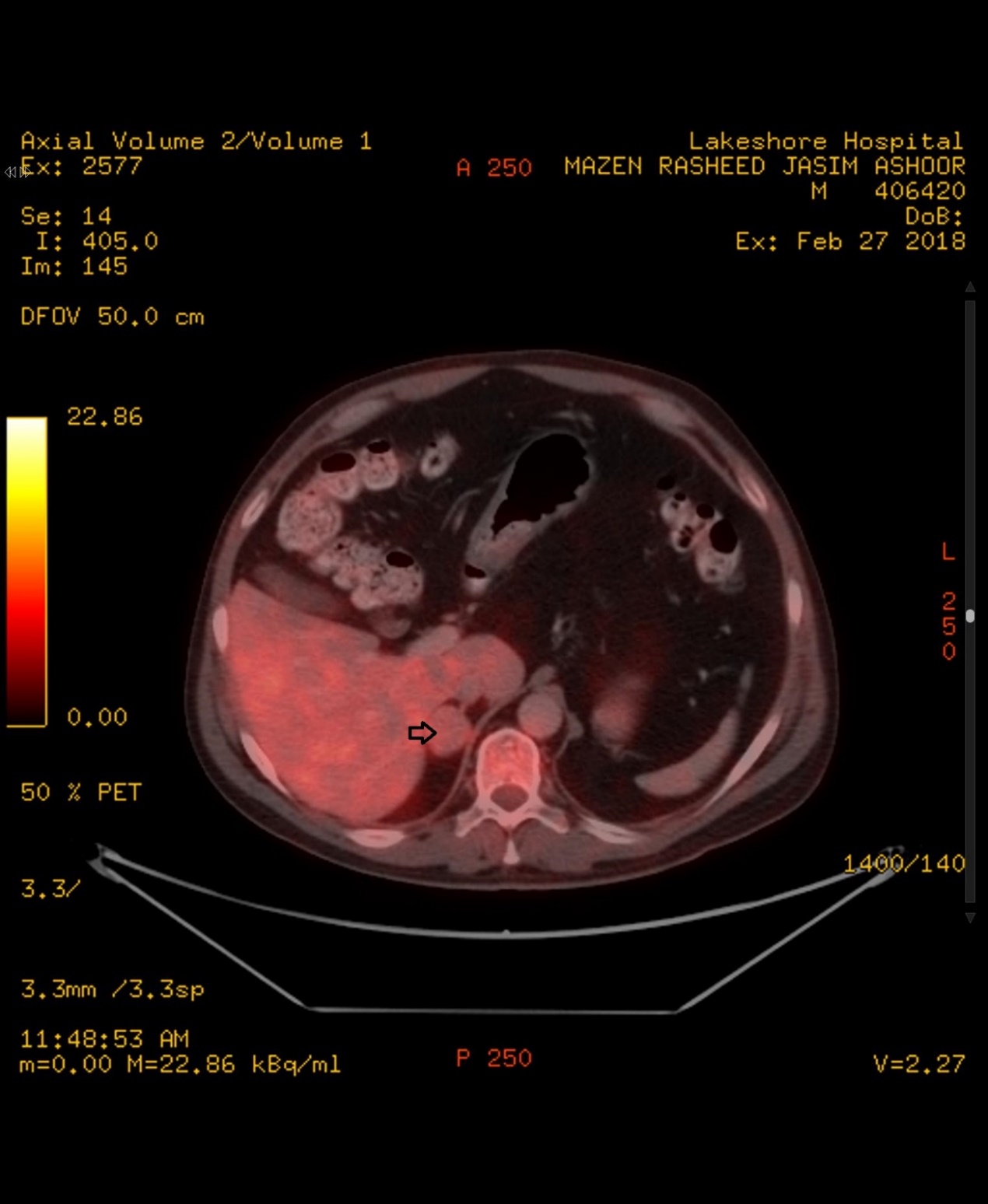
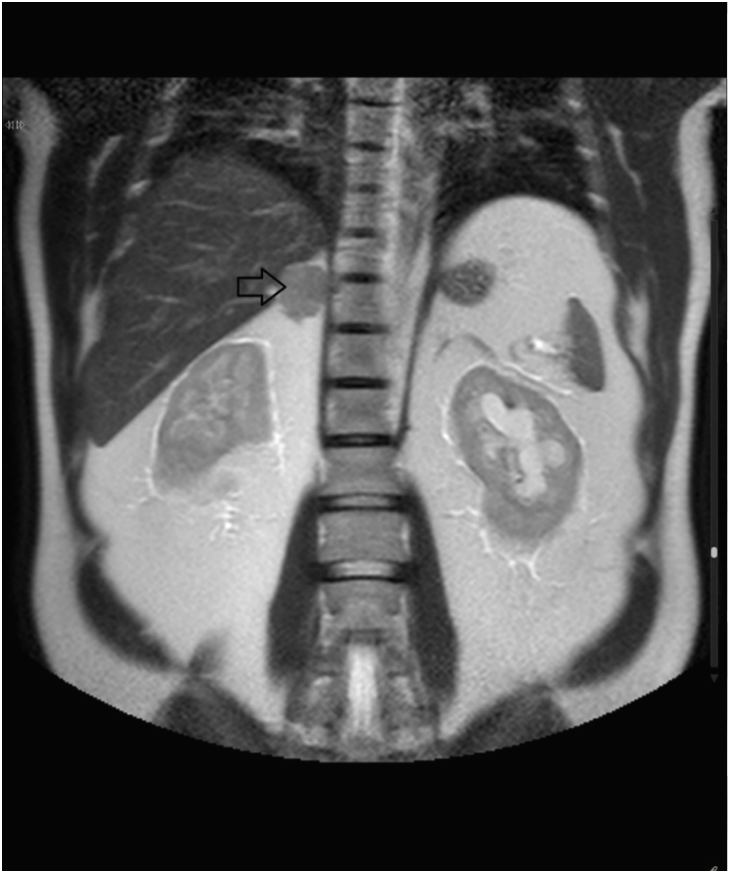
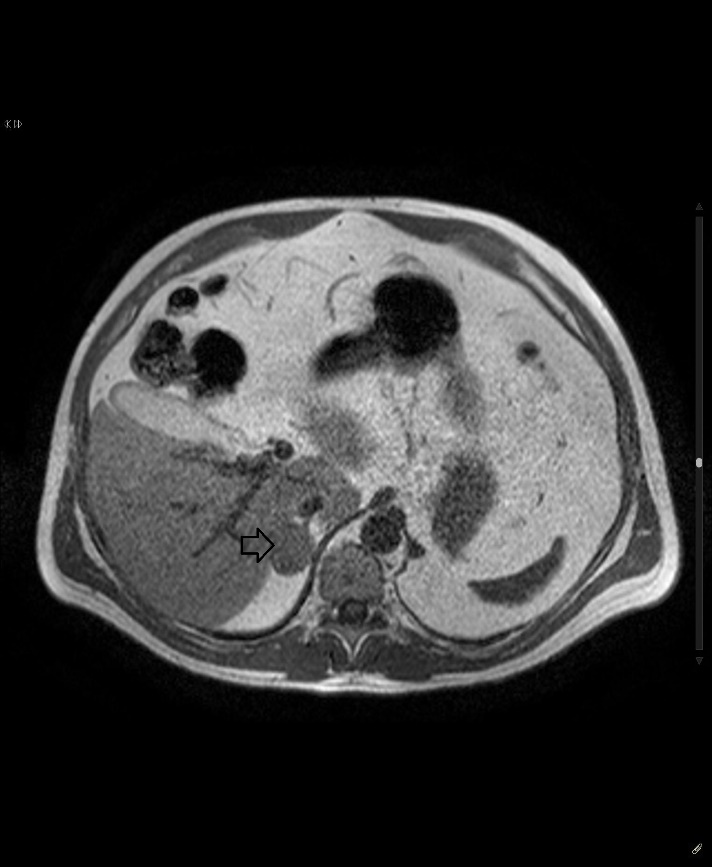
A CT scan of the abdomen was performed (Figure 1) along with whole body F18 FDG Pet/CT scan and it showed the right adrenal adenoma measuring 27x23 mm. (Figure 2).
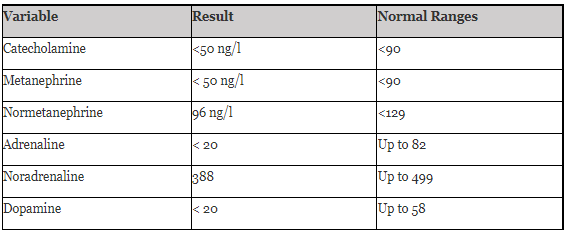
Extensive workup was done to investigate the adenoma for assessment of a functional tumor evaluating for Primary hyperaldosteronism (Table 1), Pheochromocytoma (Table 2), Cushing disease or any other condition.
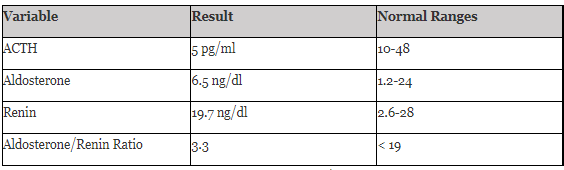
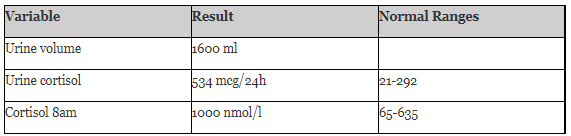
Confirmatory tests for Cushing syndrome came positive for cortisol 8 AM and 24 hour urinary free cortisol, supporting the diagnosis of Cushing syndrome (Table 3) and a low ACTH value excluding Cushing disease (Table 1).
Further investigation was requested to evaluate for the complications secondary to the disease including echocardiography and renal Doppler study, both of which were normal. His vitals were checked during his visits to the clinic and documented for high blood pressure (Table 4).

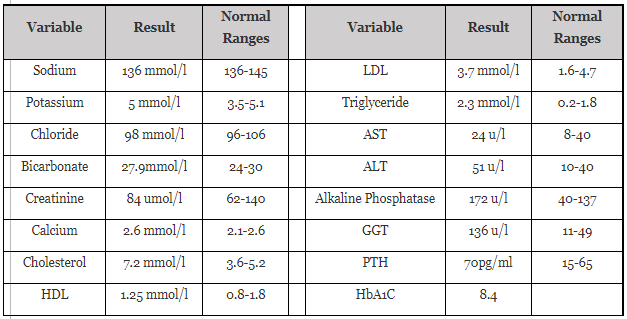
Metabolic panel was done as baseline for his condition (Table 5) which confirmed the new onset Diabetes mellitus and hyperlipidemia as well which are considered as part of his primary disease.
Based on the results of investigations done for the patient, the diagnosis of Cushing syndrome secondary to adrenal adenoma was confirmed clinically and biochemically supporting the CT and the MRI findings (Image 3, 4). So patient was referred for surgical removal of the functional adrenal adenoma for definitive treatment.
Patient underwent laparoscopic excision of the Right adrenal adenoma.







Histopathology
Histopathology showed encapsulated adrenal cortical adenoma composed of closely packed nests of polygonal cells with vaculated eosinophilic cytoplasm and central small nuclei (Figure 13 -14).
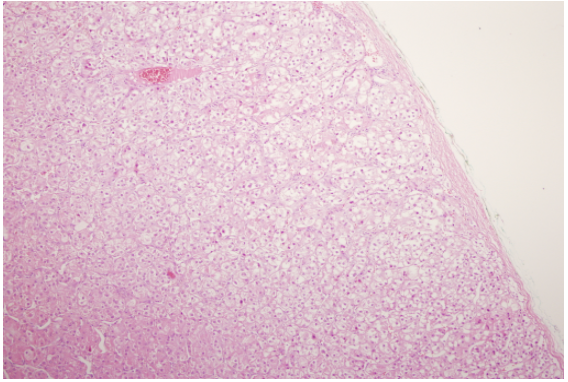
No capsular, sinusoidal or vascular invasion, diffuse architecture, significant pleomorphism, atypical mitotic figure or necrosis was seen and the adjacent adrenal gland tissue is unremarkable. The lesion measured 3cm in diameter on gross examination.
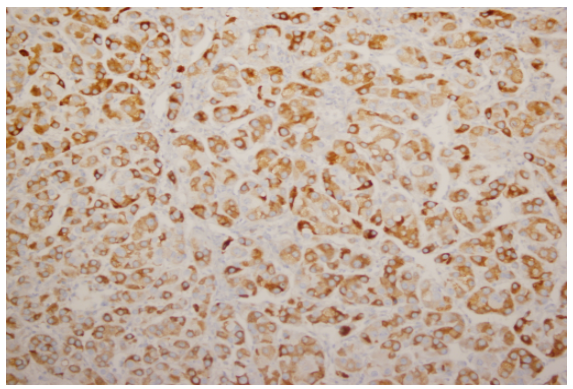
Immunohistochemical studies showed the lesion was positive for Inhibin (Figure 14 A) and Melan A (Figure 14 B), while negative for chromogranin. Proliferation index as estimated by ki67 was less than 1%.
During his post-operative follow up, the patient’s glucose profile improved and he was maintained on Metformin 2gm daily with an HbA1c of 4.4%. His blood pressure was maintained within target by monotherapy with Irbesartan (Table 6) and the patient attained a normal BMI of 23.48 with successful resolution of his symptoms and loss of central obesity.

This is a typical case of cortisol secreting adenoma causing Cushing syndrome. The diagnosis is often delayed because Cushing syndrome is frequently masked by its overlapping symptoms with many common medical problems. Like the patient in this case attended many clinics including a gastroenterologist clinic for his abdominal pain and CT was done for him as part of the work up.
The question here is whether all the incidentaloma’s should be investigated or not. The answer is yes especially with the incidence of increasing Cushing syndrome worldwide and because it is a serious disease with high morality if left untreated (12). Screening should be initiated in all patients with an incidentally discovered adrenal mass, particularly if the CT imaging density is low (<20>
Recent studies have suggested a much higher prevalence among high-risk patient populations, such as patients with diabetes mellitus (particularly if poorly controlled), hypertension, and early-onset osteoporosis (particularly if with fractures) (14-17). In a study done ontwo hundred patients with poorly controlled diabetes mellitus (HbA1C >8%) were screened for hypercortisolism and 5.5% were diagnosed with Cushing, mostly of adrenal origin (15).
Hypertension is frequently associated with Cushing syndrome with up to 67% prevalence demonstrated in a recent study (18). It resolved in 55% of the patients after treatment like in this patient, and if left untreated, it is a risk factor for cardiovascular events in association with diabetes and dyslipidemia (18). There may (19) or may not be (20) normalization of the risk factor after curative treatment of Cushing syndrome according as shown by different studies (19, 20).
In conclusion,The Endocrine Society clinical practice guidelines recommend testing for Cushing syndrome in patients with multiple signs and symptoms compatible with the syndrome and the early recognition of disease can prevent the long-term physical consequences and increased mortality that may occur when the disease is left untreated (21).
Informed Consent: Yes
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
