
Case Report | DOI: https://doi.org/10.31579/2690-1897/139
*Corresponding Author: Misha Lay, Royal Darwin Hospital, Darwin, Northern Territory, Australia.
Citation: Misha Lay and Omar Alghazo, (2023), A Case Report of Acute Emphysematous Pyelitis in Remote Australia. J, Surgical Case Reports and Images 6(1); DOI:10.31579/2690-1897/139
Copyright: © 2023 Misha Lay, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 November 2022 | Accepted: 29 November 2022 | Published: 16 January 2023
Keywords: acute emphysematous pyelitis; acute emphysematous pyelonephritis; remote medicine; urological emergency; urology
Acute emphysematous pyelitis (EP) is a rare suppurative urinary tract infection that is characterised by bacteria-formed gas within the obstructed urinary pelvicalyceal system. It often requires broad spectrum antibiotics, and urgent surgical intervention to gain decompression and source control due to the associated risk of mortality of up to 20%. The condition is also often incorrectly used interchangeably with “acute emphysematous pyelonephritis” (EPN), which is another condition associated with higher mortality, warranting more aggressive interventions such as emergent nephrectomy. This case is about a middle-aged woman from a remote community in Australia with poorly controlled type II diabetes and a recent urinary tract infection (UTI), presenting with urosepsis secondary to an acute left emphysematous pyelitis. The challenges of this case included the 36 hours of delayed access to the nearest urological service and initial concerns for acute emphysematous pyelonephritis, with associated worsening septicaemia and acute renal injury. The patient eventually had an emergency left ureteric stent insertion and made a full post-operative recovery. This case highlights the importance of early urological intervention for acute emphysematous pyelitis, and the importance of distinguishing between acute emphysematous pyelitis from acute emphysematous pyelonephritis. It also highlights the potential need for active consideration of excluding acute emphysematous pyelitis or pyelonephritis in high-risk patients, especially those living in remote and isolated from urological services.
Acute emphysematous pyelitis (EP) is a rare urological emergency associated with a significant mortality risk of up to 20%, warranting broad spectrum antibiotics and often urgent urological intervention to gain infection source control and to decompress the urinary collecting system [1]. It is characterised by bacteria-formed gas tracking within the infected and obstructed pelvicalyceal system, however, is distinguishable from a less favourable condition, emphysematous pyelonephritis (EPN) which involves gas in the renal parenchyma and is associated with significantly higher mortality. The major risk factors for EP include poorly controlled diabetes mellitus, obstruction of the collecting system and recurrent urinary tract infections (UTI). EP is often incorrectly interchangeably interpreted as EPN, which is a condition that often warrants more urgent interventions of percutaneous drainage or emergent nephrectomy for source control and mortality risk reduction [4]. This case report is about a middle-aged woman from a remote community in Australia with poorly controlled type II diabetes and recurrent E. coli urinary tract infections (UTI), presenting with urosepsis and an acute on chronic kidney injury secondary to an acute left- sided EP. This case report highlights the limitations and challenges faced in remote Australia, with an approximated 36 hours of delayed access to a urological service, associated with worsening septicaemia and renal injury. It reinforces the importance of early urological intervention for EP and to distinguish it from EPN to ensure appropriate management is in place.
A middle-aged woman from a remote community presents to the local nurse-led clinic with dysuria, suprapubic and left lower quadrant pain, associated with rigors and vomiting for approximately 48 hours duration. Her medical background includes recurrent E. coli urinary tract infections, most recently a month prior to this presentation, as well as chronic kidney disease presumed secondary to her poorly controlled type II diabetes mellitus. In the clinic, she was found to be tachycardic, tachypnoeic and pyretic. The patient was transferred via CareFlight to the nearest hospital for investigations. She was examined to have tenderness on palpation of the left side of the abdomen and left renal angle. Her bloods demonstrated leucocytosis with WCC of 40 (x 109/L) and CRP of 200mg/L. The urine dipstick identified leucocytes and nitrites, so she was subsequently treated for a urosepsis. Associated with this, she had anacute on chronic kidney injury with a creatinine rise of 450µmol/L from her baseline of 250µmol/L. An ultrasound of kidneys, ureter and bladder (KUB) performed demonstrated a moderate left-sided hydronephrosis. She subsequently had a CT KUB which demonstrated gas in the pelvicalyceal system and initial concerns for extension into the renal parenchyma (see Figure 1.1 and 1.2), with a provisional diagnosis made of acute emphysematous pyelonephritis (EPN). There were no other identified causes of urinary obstruction. Due to the absence of a urological service in that town, the patient required further urgent flight transfer to the nearest tertiary hospital after phone discussions with the nearest urological team. The time duration from initial presentation to the clinic to arriving to a hospital with the nearest urological service was approximately 36 hours.
Appendices:
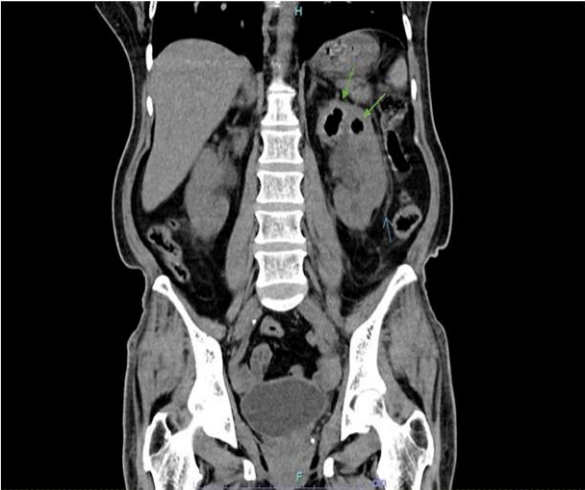
Figure 1.1: CT KUB demonstrating gas locules in the left collecting system (indicated by the green arrows) with associated left hydronephrosis and perinephric stranding (indicated by the blue arrow) suggestive of a left emphysematous pyelitis. There is no extension to the renal parenchyma to suggest emphysematous pyelonephritis.
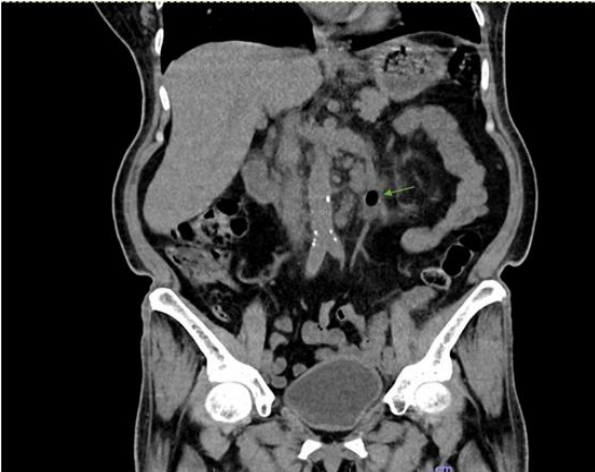
Figure 1.2: CT KUB demonstrating left pneumoureter and hydroureter. The gas locule in the dilated left ureter is indicated by the green arrow.
On arrival to the tertiary centre, she was persistently tachycardic, pyretic, oliguric and tachypnoeic which prompted an escalation of antibiotics from IV ceftriaxone to IV meropenem for empirical broad-spectrum coverage. The patient’s progression towards having an emergency ureteric stent insertion was further postponed overnight as she initially refused for any surgical intervention due to personal fears of having an operation. The patient wished for conservative management with antibiotics and bush medicine only, and was deemed cognitively competent to make that decision, as she remained resolute in her decision despite extensive discussions including her next of kin. Her CT KUB images were analysed again with some reassurance that the gas did not extend into the renal parenchyma, hence was unlikely to be EPN. Further extensive discussions took place in the next morning with the patient, involving the cultural liaison officer, an interpreter and the patient’s family members, with emphasis on the ongoing concerns and high risk of clinical deterioration, where the patient made the informed decision to undergo the operation.
Intraoperatively, there was evidence of obstructive uropathy with an obstructed left kidney that had gross purulence on cannulating the bulged left ureteric orifice. She had a tortuous dilated ureter and collecting system, however no calculus or stricture as a source of obstruction identified. A 6Ch ureteric JJ stent was inserted with a retrograde pyelogram performed to ensure adequate positioning (see Figure 2.1). The patient clinically improved post-operatively with a resolving septicaemia, with pan-sensitive E. coli grown in her urine, guiding the step-down of antibiotics back to IV ceftriaxone to complete a total of two weeks duration. Her inflammatory markers normalised along with a resolution of her AKI. She was subsequently fit for discharge four days post-operatively, back to the hospital nearest to her home community for the completion of her course of intravenous antibiotics. She was scheduled for an elective flexible cystoscopy and left ureteric stent removal in approximately six weeks.
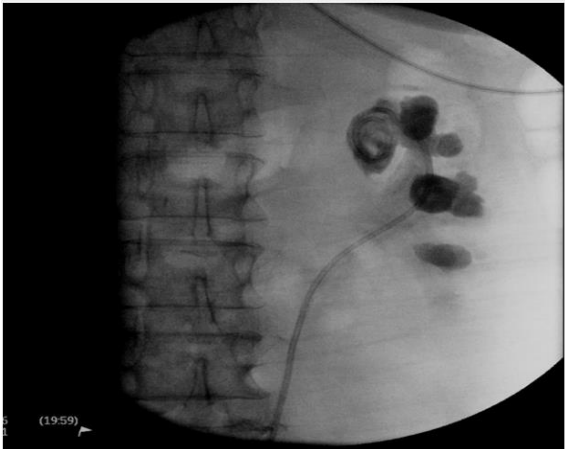
Figure 2.1: Intraoperative XR demonstrating the left ureteric JJ stent inserted within the renal calyc
Acute emphysematous pyelitis (EP) is a rare but serious urological condition that is associated with a high mortality of up to20% in limited literature, warranting urgent urological intervention to gain source control and decompress the urinary collecting system [1]. Although there have been less than 1000 published case series of EP at current, similarly as uncommon as EPN, there is some evidence that timely antibiotics and drainage of the collecting system to gain source control can avoid emergency nephrectomy and reduce risk of mortality [3,4]. Given the rarity of the condition, there are currently no clearly established algorithms for diagnosis, severity and management for EP or EPN [5]. Clinicians should be ultimately guided by the patient’s clinical status and progression, with aims to gain source control and optimise management for any organ dysfunction associated with sepsis [3]. EP is a distinct entity from acute emphysematous pyelonephritis (EPN) which is crucial to differentiate as the indicated management and associated mortality rates vary significantly where patientswith EP tend to have a more favourable outcome [2]. This case also highlights the challenges of living in a remote community, whereby access to emergent urological intervention is delayed hence the patient’s outcome may be compromised. It recommends early active investigations for EP and EPN in high-risk patients presenting with urosepsis, especially those living in remote region where early escalation of care and transfer to the nearest urological service may be required. There is also emphasis on the importance of adopting a multidisciplinary approach that incorporates interpreters and cultural advocates where necessary in achieving adequate patient advocacy, comprehension and informed consent as demonstrated in this case.
Acute emphysematous pyelitis is a rare and serious urological condition that is associated with urosepsis, acute renal injury and a mortality rate of up to 20%. This case highlights the importance of achieving early access to urological intervention to gain source control and decompression of the urinary system to reduce further renal dysfunction and risk of mortality. This is particularly emphasised in cases in high-risk patients who live in remote locations that are isolated from nearby emergent urological services.
No acknowledgements to be made. No financial support provided. The authorwas responsible for the preparation of this article.
No financial support or relationships that may pose a conflict of interest.
None declared.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
