
Case Report | DOI: https://doi.org/10.31579/2690-4861/285
LAU Medical Center – Rizk Hospital P.O. Box 11-3288 Beirut, Lebanon
*Corresponding Author: Sarah Assaf, LAU Medical Center – Rizk Hospital P.O. Box 11-3288 Beirut, Lebanon.
Citation: Daher R., Assaf S., Hayek F., (2023), A Case Report of a Thrombectomy of Internal Jugular Vein Tumoral Thrombus of Follicular Thyroid Cancer Origin, International Journal of Clinical Case Reports and Reviews. 13(3); DOI: 10.31579/2690-4861/285
Copyright: © 2023 Sarah Assaf, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 February 2023 | Accepted: 09 March 2023 | Published: 17 March 2023
Keywords: thyroid cancer; tumoral thrombus; follicular thyroid cancer
Intravascular tumor extension of a thyroid cancer is a rare but life-threatening condition. We report herein the case of a 66-year-old female patient with follicular thyroid carcinoma and an internal jugular vein (IJV) tumor thrombus. The patient had undergone a thyroidectomy at our institution and presented with left-sided swelling of face and neck. An MRI showed a thrombus within the left IJV, a finding confirmed by US. During surgery, a left IJV tumor thrombus was identified and excised followed by venous reconstruction. The pathological examination confirmed a follicular thyroid carcinoma. The patient received postoperative treatment with 150 mCi of 131I, followed by thyroid stimulating hormone suppression therapy with thyroxine. Although the fibrous capsule prevents the tumor’s invasion into the surrounding structures, the presence of a tumor thrombus carries a poor prognosis.
This is the case of a 66-year-old female patient known to have hypertension, peripheral vascular disease, gastroesophageal reflux disease, left eye cataracts status post phacoemulsification, and follicular thyroid carcinoma status post total thyroidectomy who is admitted for direct venous tumoral thrombectomy from the left internal jugular vein. 9 months prior to presentation, the patient presented with dyspnea of progressive onset. A chest X-ray showed widening of the upper mediastinum with deviation of the trachea to the right, likely related to an enlarged thyroid gland. An MRI showed an enlarged left thyroid gland mass exerting mass effect on the trachea and esophagus showing intraluminal narrowing with no evidence of obstruction and bulging anteriorly displacing the right platysma muscle. A Tumoral thrombus was found within the left internal jugular vein with preserved fat planes between the thyroid gland and left internal jugular vein. Pre-operative FNA showed follicular cells some cells arranged in microfollicles. A total thyroidectomy was thus performed, and it was complicated by transient hypoparathyroidism (PTH=3 pg/mL, nadir Ca 6.9 mg/dL). The patient received a treatment of radioiodine I-131 postoperatively, but her mass did not decrease in size. More recently, our patient presented with left-sided swelling of face and neck with no associated complaints. Physical exam showed tenderness upon palpation of left side of the neck. An ultrasound showed an intraluminal tumoral thrombus in the left internal jugular vein that shows a preserved patency (consistent with the previous MRI). She was admitted for excision of the tumoral thrombus from the left internal jugular vein (IJV) and venous reconstruction. Pre-operatively TSH 0.03 mIU/mL (low) and FT3=3.63 pg/mL
Old admission:
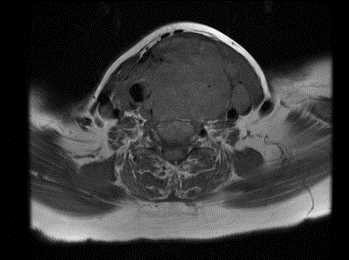
Figure 1: MRI Thrombus sub totally obliterating lumen of IJV
Current admission:
Our patient presented more recently with left-sided swelling of face and neck with no associated complaints. Physical exam showed tenderness upon palpation of left side of the neck. An ultrasound showed an intraluminal tumoral thrombus in the left internal jugular vein that shows a preserved patency (consistent with the previous MRI). She was admitted for excision of the tumoral thrombus from the left internal jugular vein (IJV) and venous reconstruction. Pre-operatively TSH 0.03 mIU/mL and FT3=3.63 pg/mL
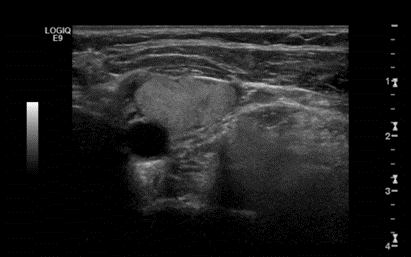
Figure 2: US showing thrombus in IJV
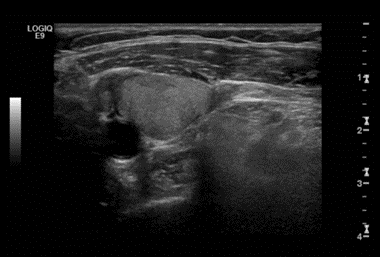
Figure 3: US
The patient underwent thrombectomy under general anesthesia. Intraoperatively/Longitudinal venotomy revealed a thrombus attached to the medial wall of the left IJV and was surgically excised. The vein was reconstructed with exclusion of the medial wall. Histopathology of the intraluminal mass was reported as an intravascular thrombus of follicular thyroid carcinoma. Recovery was uneventful. The patient received a treatment radioiodine I-131 postoperatively.
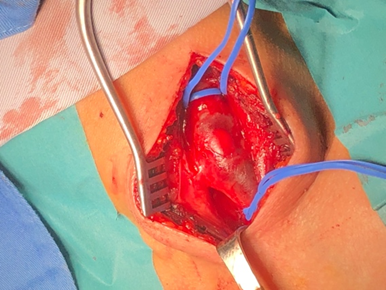
Figure 4: Operative findings: Swollen internal jugular vein identified

Figure 5: Operative findings: Internal jugular vein opened showing soft tissue tumor within its lumen

Figure 6: Macroscopic view of the tumor
Literature review:
Follicular thyroid cancer (FTC) is the second most common differentiated thyroid cancer, after papillary thyroid carcinoma, and accounts for approximately 10–15% of all thyroid cancers (Parameswaran et al., 2017). It occurs more frequently in women, and usually presents in the fifth and sixth decades of life. It typically spreads via hematogenous dissemination. Distant metastases occur in 10 to 15 percent of patients with follicular cancer, even in those with small primary tumors (Machens et al., 2005). Common sites of distant metastases are bone and lung and, less commonly, the brain, liver, bladder, and skin (Grebe & Hay, 1995).
Intravascular tumoral extension is extremely uncommon albeit life-threatening. The tumor invades the internal jugular vein through the thyroid veins and propagates, either by direct extension or by occult vascular spread with a freely mobile distal portion resembling deep vein thrombosis (Manik et al., 2016). Cervical and arm edema and pain are the most common presentations of IJV thrombosis, which may also range from being completely asymptomatic to acute pulmonary emboli and superior vena cava syndrome, so the history and examination may be indeterminate (Boedeker et al., 2004; Bukhari et al., 2011; Kobayashi et al., 2011). Recognition of a tumor thrombus by PET/CT can change the management plan and prevent unnecessary long-term anti-coagulation treatment because of wrong diagnosis of cancer-related venous thrombus (Lai et al., 2007). In thyroid cancer, the presence of a venous tumor thrombus should be considered as a risk factor of distant metastases or early relapse (Kowalski et al., 2002).
Due to the rarity of thyroid cancer vascular thrombi, no management guidelines have been established yet. Segmental venous resection or thrombectomy with venous reconstruction have been reported (Kawano et al., 2016). An intraluminal tumor mass is usually surrounded by a fibrous capsule which prevents the tumor cells from invading the adjacent vascular structures, thus making a total resection with vessel reconstruction more possible (Sugimoto et al., 2006). Invasion of IJV by thyroid cancer indicates a poor outcome (Kebebew & Clark, 2003) as thyroid cancer patients with IJV invasion or other great cervical veins are reported to have a two- to five-year survival rate (Carrington & Adams, 1988).
We report a surgical case of thyroid carcinoma with extensive tumor thrombus in the left internal jugular vein (IJV) and consider the appropriate treatment strategy (transcervical excision and venous reconstruction).
We have no potential conflict of interest. We have no competing interest to declare. The content of the manuscript has not been published or submitted for publication elsewhere. The manuscript has not been published nor is it under consideration for publication with any other journal.
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
The authors received no specific funding for this work.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
