
Case Report | DOI: https://doi.org/10.31579/2692-9562/104
1 Wyckoff Heights Medical Center, Department of Internal Medicine.
2 Sidney Kimmel Medical College at Thomas Jefferson University.
3 A.T. Still University School of Osteopathic Medicine.
*Corresponding Author: Leonard B. Goldstein, Assistant Vice President for Clinical Education Development, A.T. Still University.
Citation: Kelly Frasier M.S, Saad Javaid, Zeyar Thet, M., Mikayla Cochrane,Leonard B. Goldstein (2024), A case report of a paraneoplastic lichen planus associated with angioimmunoblastic T-cell lymphoma, Journal of Clinical Otorhinolaryngology, 6(1); DOI:10.31579/2692-9562/104
Copyright: © 2024, Leonard B. Goldstein. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 07 December 2023 | Accepted: 21 December 2023 | Published: 08 January 2024
Keywords: anesthesia for labor; sedation; childbirth
Angioimmunoblastic T-cell lymphoma (AITL) is an aggressive rare subtype of non-Hodgkin lymphoma associated with poor prognosis. Cutaneous involvement with an often-non-specific type of generalized morbilliform rash is commonly associated with AITL. Lymph node biopsy, skin biopsy, and bone marrow biopsy can be utilized when making the diagnosis of AITL. The present case study reported on a 70-year-old male patient presenting with a generalized diffuse morbilliform rash on the extremities, trunk, face, and neck originally diagnosed via skin biopsy as lichen planus pemphigoides. After an excisional cervical lymph node biopsy, however, the patient was diagnosed with AITL. Desmoglein 1 and 3 were, making the morbilliform rash more likely due to an immune response secondary to AITL. An original case report of a paraneoplastic lichen planus rash in the presence of a patient newly diagnosed with AITL provides insight to a rare cutaneous finding that corresponds to angioimmunoblastic T-cell lymphoma.
Patients with angioimmunoblastic T-cell lymphoma (AITL) experience a rare type of non-Hodgkin lymphoma, affecting 1-2% of individuals with non-Hodgkin lymphoma [1]. AITL most commonly occurs in individuals of European descent [2]. A rare symptom of AITL is a distinctive skin rash with or without pruritis. It has been found that 40-50% of patients have cutaneous involvement with AITL [3]. Typically, this rash appears as an erythematous morbilliform rash [1]. The identification of AITL often shows up through laboratory findings, excisional lymph node biopsy, and/or skin and bone marrow biopsy. AITL has a highly aggressive course and poor outcome despite chemotherapy and radiotherapy. The present study reported on an original case with an erythematous morbilliform rash associated with a diagnosis of AITL.
A 70-year-old man presented to the emergency department (ED) prior to admission to inpatient care complaining of “boils” all over his skin. He had a generalized diffuse morbilliform rash on the extremities, trunk, face, and neck. One day prior to his presentation the patient had an outpatient skin biopsy performed, which showed a pattern of linear basement membrane zone deposition with multiple conjugates consistent with a subepidermal autoimmune mucocutaneous blistering disorder including bullous pemphigoid, epidermolysis bullosa acquisita, bullous systemic lupus erythematous, or anti-collagen IV pemphigoid. At this time, the patient also had leukocytosis with banding at presentation, associated with cervical and supraclavicular lymph node enlargement. Concomitant shaggy deposition of fibrinogen along the basement membrane zone was seen in the setting of healing blisters, which was evident from the numerous amount of erupted bullae visualized upon exam. The patient left the ED with a diagnosis of lichen planus pemphigoides.
The rash began suddenly 2 months prior on the first day of taking a 6-day course azithromycin for a tooth infection. No prior history of a similar rash was reported. Physical exam was unremarkable except for a diffuse morbilliform rash sparing the palms and soles of the feet, 1+ bilateral lower extremity edema, facial edema, and cervical lymphadenopathy. His throat and neck were positive for neck lumps and swollen glands. The patient had difficulty closing his hands and making a fist due to edema in his palms. After admission, the morbilliform rash was present with multiple excoriations present, but there were no active blisters or bullae. He had 1+ bilateral lower extremity edema, in addition to edema in his palms and face. The patient also experienced loss of appetite, weakness, lethargy, malaise, and a 20-lb weight loss. A complete blood count (CBC) showed white blood cells (WBC) 26.10 K/UL, neutrophils 81.1%, and lymphocytes 4.9%. The remainder of his labs were within normal limits. Patient non-reactive for hepatitis, QuantiFERON-TB Gold, and HIV.
The generalized morbilliform rash, prominent cervical lymphadenopathy, and abnormal CBC prompted both a skin biopsy, an excisional lymph node biopsy and laboratory testing for Desmoglein 1 and Desmoglein 3 antibodies. Biopsy of the skin demonstrated separation of the epidermis and dermis with a lichenoid inflammatory infiltrated composed primarily of neutrophils (Figure 1, A and B).

Figure 1: Representative images of a skin biopsy from the left lower extremity. Photomicrographs of H&E-stained tissue sections collected at low (4x total magnification, A) and medium power (20x total magnification, B).
1A: Low-power view of skin shows separate of epidermis and dermis with a lichenoid inflammatory infiltrate
1b: Medium-power view of skin shows lichenoid inflammatory infiltrate composed predominantly of neutrophils
Desmoglein antibody tests were negative, eliminating pemphigus as a potential diagnosis. The diffuse morbilliform eruption of the extremities,
trunk, neck, and face was at first thought to be the results of a generalized fixed drug eruption, but the results of an excisional lymph node biopsy showed the patient had a diagnosis of angioimmunoblastic T-cell lymphoma (Figure 2, A and B). This report of AITL with negative findings for Desmoglein 1 and 3 antibodies indicated a paraneoplastic lichen planus rash associated with the newly diagnosed angioimmunoblastic T-cell lymphoma.
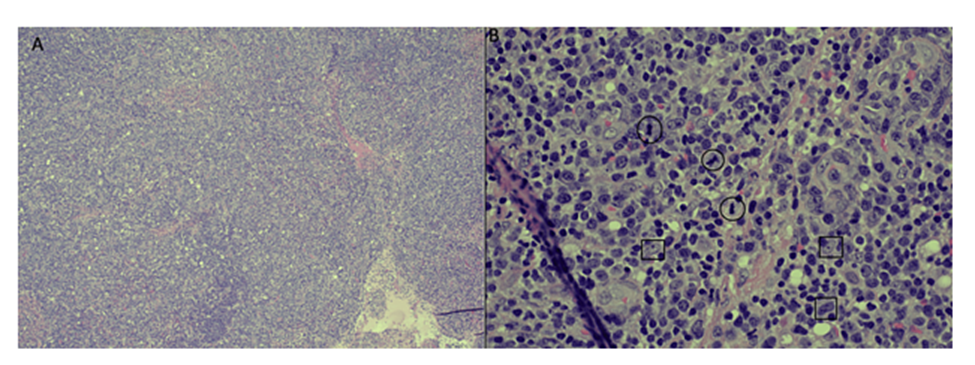
Figure 2: Representative images of a lymph node biopsy. Photomicrographs of H&E-stained tissue sections collected at low (4x total magnification, A) and high power (40x total magnification, B).
2A: Low-power view of lymph node shows complete effacement of normal architecture.
2B: High-power view of lymph node shows increased mitotic activity (circles) and large cells some with prominent macronucleoli (squares)
Angioimmunoblastic T-cell lymphoma was first reported in 1974 by Frizzera et al. and named angioimmunoblastic lymphadenopathy with dysproteinemia (AILD), classified as a peripheral T-cell lymphoma (PTCL) [4]. PTCLs are responsible for about 15% of all peripheral T-cell lymphomas [5]. PTCLs are known to be rare, aggressive types of lymphoma. They include T-cell lymphomas that develop from malignant T-lymphocytes and are both
aggressive and rapidly growing [1]. Due to their rarity, PTCLs are not well understood.
Angioimmunoblastic T-cell lymphoma involves the transformation of a T-cell into a malignant cell [1]. A differentiating factor of AITL involves immune system dysfunction, leading to a vast array of symptomatology. AITL often develops in men and women in their 60s-70s [1]. Symptoms of AITL include fever, unintentional weight loss, rash, edema, and generalized lymphadenopathy. Fatigue, pleural effusion, ascites, hepatomegaly, and splenomegaly may also be seen [6]. In 50% of patients, cutaneous symptoms are seen as macules, papules, purpura, nodules, urticaria, and nonspecific rash [5]. Symptoms arising from AITL are often due to the pathology of the immune system rather than the growth or spread of the lymphoma itself. Initial symptoms of AITL include “B symptoms,” such as fever, weight loss, and night sweats [5].
Diagnosis of AITL is made through clinical evaluation, patient history, lymph node biopsy, and/or biopsy of the skin. Lymph nodes are often easily palpable in the neck, tonsils, axillary, and inguinal regions. Splenomegaly and hepatomegaly are also common. Edema and abnormal fluid accumulation may also be seen [6]. Blood testing, bone marrow biopsy, MRI, CT, and PET scan may help evaluate a patient for AITL [7].
Therapies used to treat AITL include chemotherapy and corticosteroids. Prednisone may be used alone in treating AITL, but it can also be used in conjunction with chemotherapy agents [1]. The recommended treatment for this aggressive form of lymphoma has been titled the “CHOP” regimen [8]. This regimen includes cyclophosphamide, doxorubicin or hydroxydaunorubicin (Adriamycin or Rubex), vincristine (Oncovin), and prednisone. While the initial response to CHOP is positive, the overall effect has been considered less than adequate. Many patients relapse after treatment. Many different types of drugs are currently being studied to treat patients with AITL, including but not limited to cyclosporine A, interferon alfa, clarithromycin, prednisolone, and Romidepsin [8]. Chemotherapy, in combination with autologous stem cell transplantation and radiation therapy, has also been used with the promise of helping individuals with AITL stay in remission after treatment [9]. Additional research must be conducted to determine new combinations and therapies of drugs combined with alternative therapies as safe and efficacious methods to treat patients with AITL.
Angioimmunoblastic T-cell lymphoma (AITL) is an aggressive, rare subtype of non-Hodgkin lymphoma associated with poor prognosis. One potential sign of AITL is a generalized morbilliform rash. In this case study, we report on a 70-year-old male patient who presented with a generalized morbilliform rash on the extremities, trunk, face, and neck. Per skin biopsy, the rash was originally diagnosed as lichen planus pemphigoid; however, cervical lymph node biopsy revealed AITL. This case report demonstrates using different biopsy sites (lymph node biopsy, skin biopsy, and bone marrow biopsy) to diagnose AITL. In addition, this report raises awareness that AITL may appear as paraneoplastic lichen planus on biopsy.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
