
Case Report | DOI: https://doi.org/10.31579/2690-1897/136
"Research Institute of Cardiology and Internal Diseases"1, "Kazakh National University named after. Al-Farabi"2.
*Corresponding Author: Abzaliev K.B., Research Institute of Cardiology and Internal Diseases
Citation: Ormanov B.K, Abzaliev K.B, Kolesnikov A.E, Abzalieva S.A. (2023). A case of successful implantation of a modified stent graft in a dissecting aortic arch aneurysm, J. Surgical Case Reports and Images, 6(1); DOI: 10.31579/2690-1897/136
Copyright: © 2023. Abzaliev K.B. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 November 2022 | Accepted: 29 December 2022 | Published: 04 January 2023
Keywords: modified stent graft; dissecting aneurysms of the arch and thoracic aorta; fenestration; endovascular surgery
With the development of endovascular intervention methods, it became possible to save the patient in more cases. If it is not possible to install a stent graft for technical reasons or the patient is not transportable, open surgical interventions remain.
The authors described a method for treating a patient with a dissecting aneurysm of the thoracic aorta type IIIB according to DeBakey using a stent graft by forming a fenestration according to the model of the anatomy of the left subclavian artery orifice, modified by a physician "on the operating table". Such modifications on the table or in situ make it possible to model the prosthesis according to the variant of the anatomy of a particular patient, which allows optimizing the fit of the prosthesis, eliminating additional stages of complex surgical treatment, reducing the undesirable consequences of standard approaches, including preliminary endovascular occlusion of the left subclavian artery and the formation of a carotid-subclavian shunt, reduce time of stationary observation. The use of the described technique makes it possible to reduce complications in radical (open) surgical treatment of patients with dissecting aneurysms and increase the effectiveness of treatment. This technique is a promising direction in the development of endovascular and surgery and requires further study to assess long-term results and prognosis in a large number of patients.
In order to increase the radicalness of intervention for aortic aneurysms, various staged and combined techniques are used. In this case, the main problem is the optimization of the ratio of the volume of surgical intervention and the physiological reserve of the patient [1]. Open surgery was traditionally the gold standard of surgical treatment before the development of X-ray endovascular correction methods. Open surgery for this pathology is always associated with high perioperative risks and mortality. And with comorbid conditions or concomitant diseases and with complex anatomical features, the risk of open surgery increases significantly, and specialists understand this.
A much more complex aortic lesion, consisting of aneurysm and aortic dissection involving the aortic arch, presents a technical challenge for remodeling due to involvement of the left subclavian artery. With the development of endovascular methods, options for endovascular treatment of complex pathology of the aorta involving the arch are being developed. A promising approach is the use of fenestrated or branched endovascular aortic plasty (F/B-EVAR.
There are severe lesions of the aorta, in which it is difficult or impossible and generally contraindicated to install factory-made stent grafts. This is possible only in the case when endovascular plasty with a prosthesis can be personalized intraoperatively modified. For this procedure, the operating surgeon modifies the endovascular graft during the intervention by creating additional fenestrations according to the patient's anatomy. Numerous reports have been published demonstrating that this procedure can be performed with high technical success and acceptable perioperative and mid-term outcomes in high-risk patients [2,3,4]. We demonstrate our clinical case, which shows high success, the skill of the surgeon and is applicable in practice.
Case report No.1
Patient N. Male, 80 years old, underwent a routine examination at the place of residence in November 2019, and where an increase in the contours of the aortic arch was accidentally detected on a chest x-ray. The patient was examined by an angiosurgeon at the place of residence and received recommendations for optimal drug therapy, followed up until 2221. In May 2021, he began to notice the appearance of blood streaks in the sputum when coughing, in connection with which he consulted an angiosurgeon, who sent him for CT angiography with contrast. (Fig.1.)
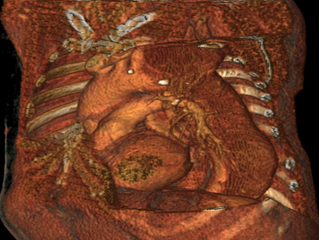
Figure. 1 Aneurysm of the descending aorta with wall dissection, type IIIb according to DeBakey.
The examination revealed a picture of a fusiform aneurysm of the descending aorta with dissection of the walls in the transversely descending and distal sections, type IIIb according to DeBakey. After that, he was referred to an X-ray surgeon, who recommended the installation of a stand-graft in stationary conditions. After a standard examination and identification of the causes of contraindications (chronic renal failure, the degree of ischemic coronary heart disease, the degree of arterial hypertension, gastric ulcer, diabetes mellitus, etc.), he was hospitalized. Patient: height 158 cm, weight 56 kg, BMI 22.3. An experienced smoker, registered with a cardiologist since 2007 for coronary heart disease, arterial hypertension with an increase in pressure up to 170/110 mm Hg, periodically adhered to antihypertensive therapy.
07.12.2021 after discussing the tactics and strategy of treatment, the patient underwent endovascular implantation of a fenestrated stent graft “on the table” into the descending thoracic aorta.
After spinal anesthesia, placement of a central catheter into the jugular vein on the right, and preparation of the surgical field of the upper third of the left thigh in the groin area, a skin and subcutaneous fat incision was made in the projection of the common femoral arteries. After opening the femoral fascia, blunt and sharp access was made to the common femoral artery (BOA) on the left. Then a standard thoracic aortography was performed, which revealed an aneurysm of the descending thoracic aorta. (Fig.2.)
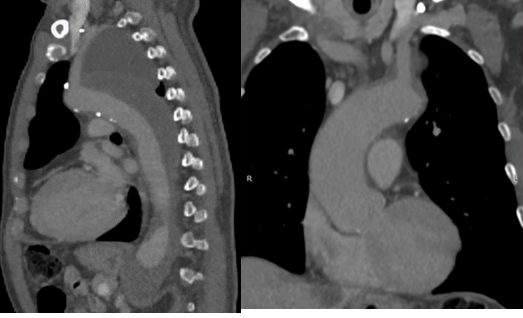
Figure 2. Aneurysm of the descending thoracic aortaThe stent-graft was removed by 1/4 of the length of the delivery catheter, in the projection of the landing zone at the orifices of the internal carotid artery (ICA) and the left subclavian artery (LAS), the proximal end of the stent-graft was fenestrated in the form of a wedge "on the table". Next, the selected CFA is pierced on the left. On a diagnostic catheter, a superrigid guidewire was introduced into the aortic arch and its distal end was placed in the ascending aorta. The catheter was removed and a partial arteriotomy was performed. After expanding the vascular access through a superrigid guidewire, a modified thoracic stent-graft Valiant Thoracic StentGraft 36.0x36x200.0 mm (No.……series…production….) was delivered to the aortic arch, mounted on a Captivia delivery system (company?).

Figure.3. Angiography for stent graft sizing
Then, under the control of angiography (Fig. 3.) and fluoroscopy, the stent-graft was placed in the descending thoracic aorta, capturing the area of the dissecting aortic defect, proximal to the celiac trunk. After the stent-graft was exposed, the “crown” of the proximal apparatus was opened immediately after the brachiocephalic trunk originated so that the fenestrated zone was at the border of the origin of the left common carotid artery and the orifice of the left subclavian artery. (Fig. 4.) During intermediate angiography, the crown of the stent graft was fully opened, the arteries of the aortic arch were patent.

Figure 4. Fenestration of the zone where the left common carotid artery and the mouth of the left subclavian artery will be locate

Figure 5. Stent graft fully deployed and implanted
The stent graft is fully deployed and implanted (at what pressure and for how many seconds, once or repeatedly?) (Fig. 5.) The delivery system is removed. During the control aortography, the stent graft and arteries of the aortic arch were completely patent, the false lumen was not contrasted. The CFA defect on the left was sutured with interrupted vascular sutures with a 6/0 Prolene suture. Hemostasis achieved. The wound was sutured in layers, drainage was installed, and an aseptic dressing was applied. The CFA introducer is on the right, the puncture site is removed, closed with the Angioseal 6F apparatus, an aseptic dressing is applied.
The patient was transferred to the intensive care unit for follow-up.
According to the European Society of Angiosurgeons of 2017, thoracic aortic arthroplasty (TEVAR) is not only considered an effective treatment for aneurysms of the arch and abdominal aorta, but is also recommended for use. According to the literature, the use of fenestrated or branched stent grafts showed the best clinical results in senile patients with comorbid pathology. The technique of "stent-graft fenestration" during surgery in the treatment of thoracic aortic aneurysms with dissection of the arch and abdominal aorta to bypass the visceral branches of the aorta is innovative and presents a certain risk. Subsequently, such technologies were tested with different manufacturers of stent grafts and different models.
This technique allows TEVAR to be carried out simultaneously without the development of undesirable consequences. Although today a technique using a special catheter with a puncture needle at the end is recognized as a safe technique for performing fenestration. This technique is aimed at maintaining blood supply to the left common carotid and subclavian arteries after the installation of a stent in the aortic arch, and makes it possible not to perform open bypass surgery in the future. Although such a tactic and strategy is also justified in high-risk comorbid patients, especially in situations where the administration of a contrast agent is limited. In situations where it is impossible to perform TEVAR, hybrid treatment remains the operation of choice in practice.
In our case, intraoperative fenestration "on the table" in the form of a stent-graft wedge allowed maintaining the patency of the LSA without forced occlusion with a plug and the formation of subsequent ischemia of the left upper limb with symptoms of Still's syndrome from the vertebral artery with inevitable neurological deficit. In the control study on MSCT, the modified stent graft was well positioned and there were no deformities. (Figure 6.)
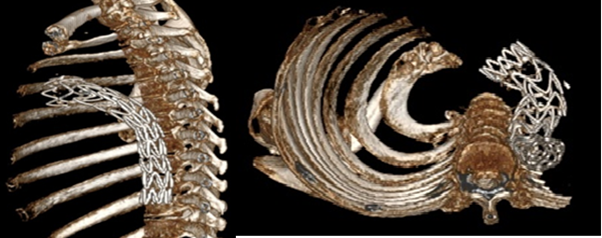
Figure 6. Implanted modified stent graft is well placed
Such modifications on the table or in situ make it possible to model the prosthesis according to the variant of the anatomy of a particular patient, which allows optimizing the fit of the prosthesis, eliminating additional stages of complex surgical treatment, and reducing the undesirable consequences of standard approaches, including preliminary endovascular occlusion of the left subclavian artery and/or the formation of a carotid-subclavian shunt. , reduce the time of stationary observation. The use of the described technique will reduce the radicalness of surgical treatment of patients with dissecting aneurysms and increase economic efficiency. This technique is a promising direction in the development of endovascular surgery and requires further study to assess long-term results and prognosis in a large sample of patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
