
Case Report | DOI: https://doi.org/10.31579/2690-4861/538
1Department of Surgery, Ohara General Hospital.
2Department of Gastrointestinal Tract Surgery, Fukushima Medical University.
3Department of Comprehensive Cancer Treatment and Research at Aizu, Fukushima Medical University.
4Cancer Treatment Center, Aizu Chuo Hospital.
5Department of Pharmacy, Ohara General Hospital.
*Corresponding Author: Masahiko Shibata, Department of Comprehensive Cancer Treatment and Research at Aizu, Fukushima Medical University.
Citation: Takahiro Kawamata, Masahiko Shibata, Takeshi Imoto, Chiaki Takiguchi, et al, (2024), A case of oxaliplatin-induced immune thrombocytopenia followed by complete remission of metastatic colon cancer, International Journal of Clinical Case Reports and Reviews, 19(2); DOI:10.31579/2690-4861/538
Copyright: © 2024, Masahiko Shibata. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 September 2024 | Accepted: 19 September 2024 | Published: 08 October 2024
Keywords: oxaliplatin, OIIS, thrombocytopenia, Evans syndrome
An 87-year-old male underwent laparoscopic left hemicolectomy for adenocarcinoma of the descending colon in December 2021. Lung metastasis was found in the left upper lobe 6 months postoperatively, and it increased in size after 9 months from the surgery. S-1 plus oxaliplatin (SOX) was started in October 2022. The lung metastasis was shrinking within 23 cycles of SOX therapy. The 24th cycle of SOX (only oxaliplatin) was administrated in April 2024, the catheter of venous infusion line of right forearm was removed after finishing the infusion, however bleeding did not stop. The platelet count was rapidly dropped into 2,000/μl from 131,000/μl (pretreatment) within 7 hours and hemoglobin levels decreased from 10.9 to 8.9 in the same period, furthermore, dropped into 6.2 g/dl in next 24 hours. PA-IgG was significantly high (204.0 ng/107 cells; normal < 30.2). Transfusion of platelet, red blood cell concentrate, steroid pulse therapy, antibiotic treatment with multiple agents and non-invasive positive pressure ventilation (NPPV with oxygen were performed. As a result, the patient’s platelet count was increased and his DIC score was decreased to 3 points (normal range) in April 2024. The patient’s general condition gradually improved, and he was discharged from hospital on the 35th day of hospitalization. CT scan after discharge showed complete remission of the lung metastasis. Possible mechanisms and approach to treatment are discussed.
Hematological disorders are common adverse effects of anticancer chemotherapeutic agents. Among them, thrombocytopenia is a frequently experienced complication during chemotherapy and sometimes is remained even after the chemotherapy is terminated. Chemotherapy-induced thrombocytopenia sometimes cause chemotherapy delays, dose reductions, and discontinuation of chemotherapy, and have negative influences on treatment outcomes. There is no approved agent available to manage thrombocytopenia [1].
An 87-year-old male underwent laparoscopic left hemicolectomy with a diagnosis of adenocarcinoma of the descending colon in December 2021. Lung metastasis was found in the left upper lobe 6 months postoperatively, and it increased in size after 9 months from the surgery (Figures 1a,b). The patient began S-1 plus oxaliplatin (SOX) treatment with first-line chemotherapy consisting of oral S-1 (a mixed drug of tegafur, gimeracil, and oteracil potassium) at a dose of 50 mg twice daily for 2 weeks following by 1-week off schedule, and intravenous oxaliplatin (100 mg/m2) given on day 1 of a 3-week cycle [2,3], was started in October 2022.The lung metastasis was shrinking within 23 cycles of SOX therapy (Figures 1c–f). The 24th cycle of SOX (only oxaliplatin) was administrated in April 2024, the catheter of venous chemotherapy line of right forearm was removed after finishing the infusion, however bleeding did not stop. The patient had vomiting, chill and pale face, and was transferred to the intensive care unit. The platelet count was rapidly dropped into 2,000/μl from 131,000/μl (pretreatment) within 7 hours and hemoglobin levels decreased from 10.9 g/dl to 8.9 g/dl in the same period, furthermore, dropped into 6.2 g/dl in next 24 hours. Disseminated intravascular coagulation (DIC) score was 8 points, and platelet-associated IgG (PA-IgG) was significantly high (204.0 ng/107 cells; normal < 30>.

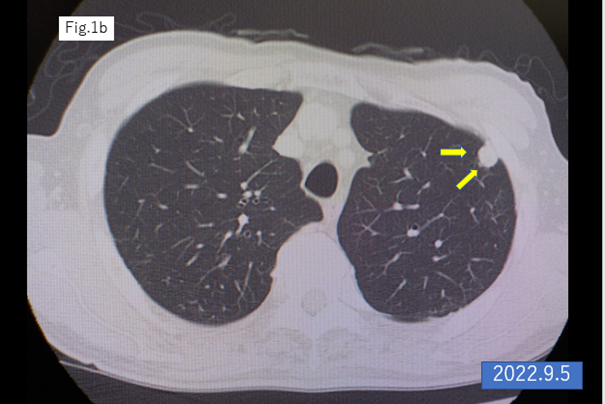
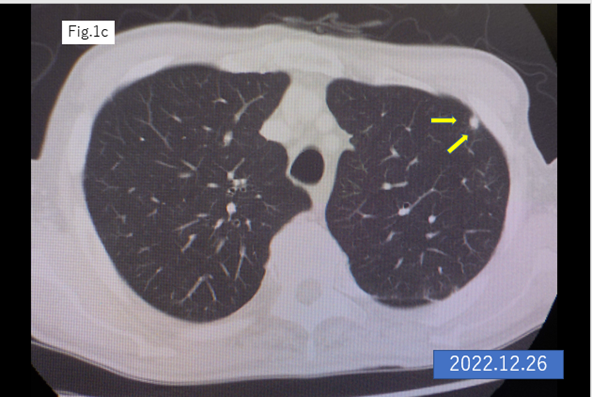
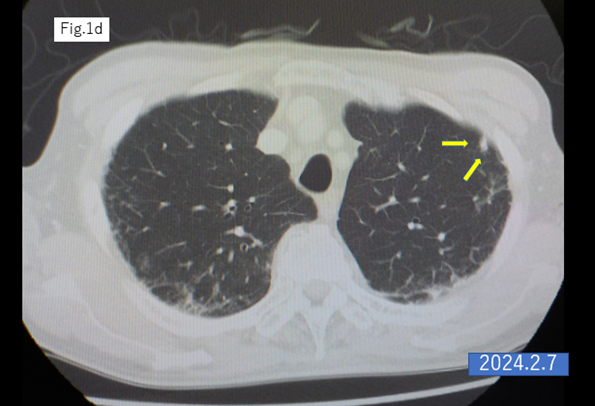

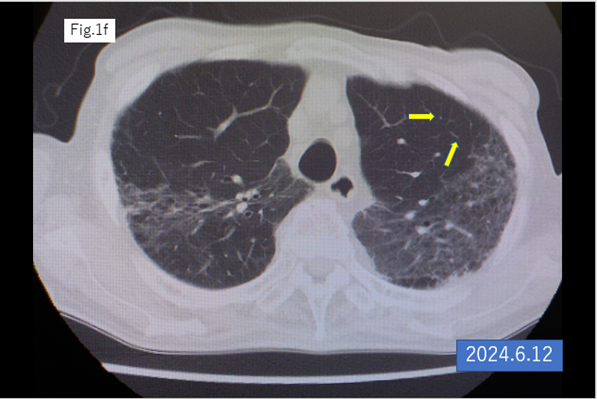
Figure 1: CT scan of the lung

Figure 2: Clinical course of the patient.
NPPV, non-invasive positive pressure ventilation
PLT 10U, platelet transfusion of 10 units
RBC 2U, transfusion of red blood cell concentrate of 2 units
Hb, hemoglobin (g/dl)
PLT, platelet count (/μl)
PA-IgG, platelet associated IgG (ng/107 cells)
Allergic hypersensitivity has been reported to occur in 10–23.8% of patients who have undergone oxaliplatin therapy, known as a type I hypersensitivity reaction involving IgE mediated release of antibodies, is well known complication and is usually well-managed with using steroid [9-11]. Oxaliplatin-induced ITP, as shown by our case, is a type II hypersensitivity reaction involving release of IgG antibodies binding tos platelet surface [12-15]. These two types of allergic reaction are known as oxaliplatin induced immune syndrome (OIIS) and the latter, as shown in the present case, has been reported to present hyperacute thrombocytopenia is recommended to be treated with steroid pulse therapy and platelet transfusion. In the present case, although DIC score was high and sufficient for DIC diagnosis, anticoagulation therapy was not selected but steroid pulse as well as infusions of platelets and concentrated red blood cells were performed, and alveolar bleeding and pneumonia were successfully managed followed by recovery. Although no anticancer therapy was administered since the onset of thrombocytopenia, the nodule of lung metastasis was disappeared after the recovery, and the mechanisms of this anti-tumor reaction are not clear. Given that oxaliplatin has been reported to induce immunogenic cell death in the tumor microenvironment [16,17], anti-tumor immune reactivities including in immunological memory may exist, and some mechanisms of immunosuppression might be altered by chain of immunological events occurred to this patient.
Evans syndrome, first reported in 1951 [18], is an uncommon condition characterized by ITP combined with autoimmune hemolytic anemia (AHA) with a positive direct antiglobulin test (DAT) and a positive direct Coombs test [19]. In the present case, since hemoglobin levels were dropped from 10.6 into 6.2 g/dl within 2 days combined with thrombocytopenia, the underlying pathophysiology of our case might be included in Evans syndrome. Rousseau et al. reported that there are two mechanisms, hapten-specific and neoantigen-dependent (immune complex), that are involved when Evans syndrome is induced by oxaliplatin [20]. In the second mechanism especially, the complement system may be activated, and the disappearance of metastatic nodule in our case might be associated with complement-dependent cytotoxicity against cancer cells.
Although this entity of pathophysiology is uncommon and has not been described well in the past reports, appropriate managements such as steroid pulse and blood transfusion may succeed. This life-threatening symptom should motivate physicians to refer to specialized laboratory examination for OIIS and Evans syndrome during and after oxaliplatin therapy.
We thank Dr. Atsuro Fukuhara of department of respiratory diseases for valuable advises and clinical staff of chemotherapy center of Ohara general hospital for prompt management for this case.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
