
Research Article | DOI: https://doi.org/10.31579/2768-0487/096
1 Clinic for thoracic surgery Clinical Center of the University of Sarajevo, Bosnia and Herzegovina.
2 Clinic for Pediatric Surgery, Clinical Center of the University of Sarajevo, Bosnia and Herzegovina.
3 Anesthesia and resuscitation clinic Clinical Center of the University of Sarajevo, Bosnia and Herzegovina.
4 Sarajevo Canton Health Center, Hadžići Bosnia and Herzegovina.
5 Department of Pediatric Hemato-Oncology, Pediatric Clinic, Clinical Center of the University of Sarajevo, Bosnia and Herzegovina.
6 Institute of Radiology, Clinical Center of the University of Sarajevo, Bosnia and Herzegovina.
7 Institute of Pathology Clinical Center of the University of Sarajevo, Bosnia and Herzegovina.
*Corresponding Author: K. Karavdic, Clinic for Pediatric Surgery, Clinical Center of the University of Sarajevo, Bosnia and Herzegovina.
Citation: Pilav I., A. Alihodzic-Pasalic, Karavdic K., Mesic A., Spiljak A., et al., (2023), A Case of Giant Posterior Mediastinal Ganglioneuroma – A 7 Years Old Boy, Journal of Clinical and Laboratory Research. 6(1); DOI:10.31579/2768-0487/096
Copyright: © 2023, K. Karavdic. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 April 2023 | Accepted: 17 April 2023 | Published: 24 April 2023
Keywords: case report; ganglioneuroma; resection
Introduction: Ganglioneuromas are rare, slowly growing, benign tumors originating from sympathetic ganglions with a benign histology. Although ganglioneuromas are benign, the treatment is surgical as they can cause pain or compression symptoms, can be locally aggressive and can lead to cord compression.
Case Report: A 7 years old-boy was referred to our Oncologic Pediatric Departement due to a giant retroperitoneal and mediastinal mass detected in computed tomography (CT) scans. The initial symptoms were presence of a nonproductive cough a few months early. Presurgical biopsy revealed a benign ganglioneuroma. Total tumor resection of 125x115x165mm tumor was obtained successfully via thoracotomy. Histopathological analysis confirmed the diagnosis. Surgically challenging aspects were the tumor invasion into the mediastinum through the aortic hiatus. Postoperative functioning was excellent without any sign of neurologic deficit.
Conclusions:
Ganlioneuromas of the mediastinum are slow-growing, large tumors, mostly asymptomatic, and the first symptoms are a consequence of the compressive effect of the tumor.
The gold standard in the diagnosis of ganglioneurinoma is CT and needle biopsy.
Complete surgical removal is recommended for symptom control or prevention of potential malignant degeneration
Subsequent long-term follow-up including imaging controls is mandatory to prevent potential relapse.
Ganglioneuromas are rare (1/1,000,000), slowly growing, benign tumors that can originate from any location in the paravertebral sympathetic plexus or more rarely from the adrenal medulla [1]. Loretz first described tumor in 1870.Ganglioneuromas are most commonly seen in pediatric populations, with 60percentage of total diagnoses occurring prior to the age of 20 [2]. The median age at the time of the diagnosis is reported to be approximately 7 years [3]. Ganglioneuromas, in general, occur more frequently in females than in males with a ratio of about 3:2 [4,5]. They are usually asymptomatic but these tumors are generally diagnosed due to compressive symptoms according to tumor size and rarely to systemic symptoms [6]. The treatment is complete surgical resection [7]. We present a 7 year old boy with a ganglioneuroma of the right posterior mediastinum who presented with presence of a nonproductive cough, together with the clinical features, CT and MRI findings, differential diagnosis tips and their contribution to surgical planning.
The patient, 7 years old boy, was accompanied by his mother who informed the primary healthcare physician that she noticed the presence of a nonproductive cough a few months back and that he is currently running a mild fever. The cough had been treated before unsuccessfully. During the physical examination while auscultating the lungs it is noticed that sounds are diminished on the right side, particularly above the lower lobe. Laboratory tests showed heightened CRP levels at 28 mg/L. Diminished lung sounds and elevated CRP caused suspicion and patient was referred to get a chest and lung radiograph. The RTG image showed an abnormal shadow on the right lung (figure 1) and the pulmonologist who read the imaging suggested emergency hospitalization at the Pediatric Hospital of the University Clinical Center Sarajevo.
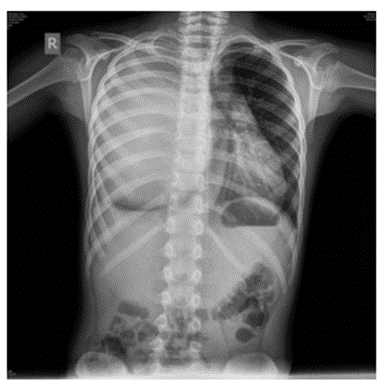
Figure 1: The RTG chest image abnormal shadow on the right lung
The pediatrician who saw the patient suggested parenteral and oral antibiotic treatment after which the patient was feeling subjectively better. The pediatrician who saw the patient suggested parenteral and oral antibiotic treatment after which the patient was feeling subjectively better. Physical examination of the chest on admission (examination of the thoracic organs): On the right side, muffled breathing sound by auscultation. Ictus cordis moved towards the front axillary line The patient was admitted to the Hemato-oncology Department of the Pediatric Clinic, where an additional diagnostic procedure was performed, chest CT and needle biopsy under CT control. The CT image is dominated by an enormously large Tm mass of the right hemithorax, which almost completely fills it - dimensions approx. 125x115x165mm (APxLLx165mm), predominantly solid tissue density (on average between 30-40 HU) but also fluid density in places. This mass behaves compressive on the contents of the anterior and middle mediastinum, i.e., the heart, above all, which is shifted to the left and anteriorly, with compression and the descending thoracic aorta, which is shifted to the left, as well as the VCS. A significant shift and compression of the trachea is visible, which is particularly observed in the segment immediately before the bifurcation. The right main bronchus is severely compromised width of the lumen, the same has a narrowed and deformed flow due to compression of the medial contour of the described tumor mass, with a consequent marked reduction in the width of the lumen and lobar and part of the visible segmental bronchial branches - the same are followed on a very short section. from the small branches of the descending aorta, while the branches of the pulmonary artery bypass it peripherally. On the right in the basal parts and in front, along the very contour of the tumor mass - peripherally on the right, a triangular dense consolidation according to the type of atelectasis is observed. The findings indicate an enormously large solid tumor mass of the right hemithorax that fills almost the entire right hemithorax. The tumor is very expansive and displaces the anatomical structures of the anterior and middle mediastinum as described in the description (heart and large vessels, trachea and the initial part of the tracheobronchial tree on the right), compromising the lumen of the mentioned vascular structures as well as the trachea and tracheobronchial branches (figure. 2, 3).
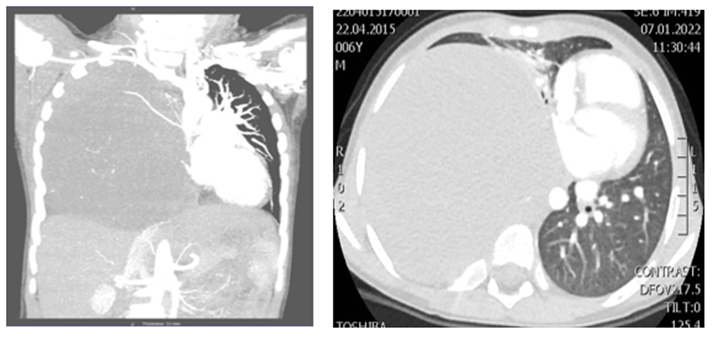
Figure 2,3: CT chest large Tm mass of the right hemithorax compressive on the contents of the anterior and middle mediastinum.
Under CT control, a needle biopsy of the mass in the right hemithorax is performed with an 18G needle, through a lateral intercostal approach. Four cylinders of tissue sent to PHD which confirmed the diagnosis of ganglioneuroma.
Based on the clinical picture, physical findings, X-ray and CT of the chest, and the pathohistological findings of the puncture biopsy, an indication for surgery is established. Operative findings: Right posterolateral thoracotomy opened the thorax through the sixth rib socket. Inspection reveals a clearly demarcated solid tumor mass, which behaves compressively towards the surrounding structures and fills the entire right hemithorax (figure. 4,5). During tumor removal, the 6th rib is planned to be broken due to the enormous size of the tumor and easier remove. At first, the lung lobes are not identified in the right pleural cavum, the right lung is collapsed. With the extra pleural approach, the fibrous capsule of the tumor is identified by meticulous preparation, which is opened. Reduction of the tumor mass with Impact and Ligasure is performed, considering the size and connection with the surrounding structures (figure. 6,7). The two arterial branches are ligated with Prolene 4-0 and resolved. After the complete removal of the tumor, meticulous hemostasis follows and the release of the lung wing into ventilation, where the complete re-expansion of all lung lobes is recorded (figure. 8,9). A 20Fr thoracic drain is placed in the right pleural cavity. They are treading on the number. Suture the thoracotomy wound in layers. The patient's awakening from anesthesia proceeds normally.
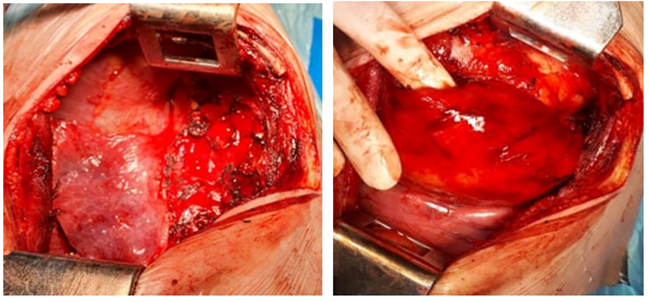
Figure 4,5: Right posterolateral thoracotomy solid tumor mass, which behaves compressively towards the surrounding structures
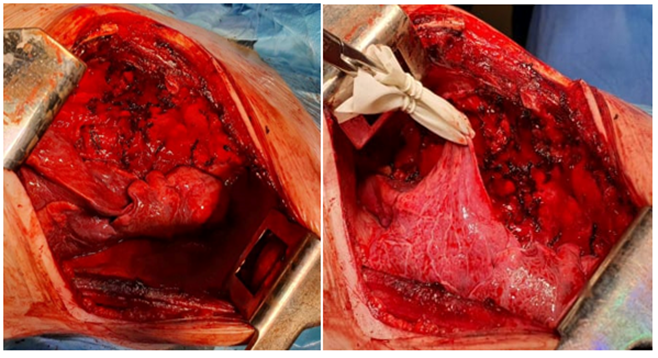
Figure 6,7: Reduction and gradual tumorectomy, atelectatic lung parenchyma and released mediastinal pleura.
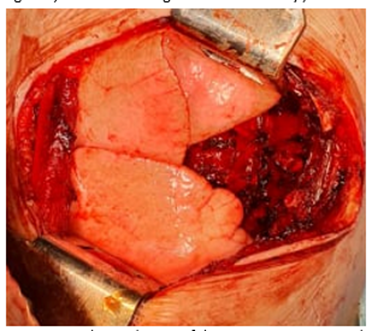
Figure 8: Complete reduction of the tumor mass, reexpanded lung parenchyma and empty mediastinal space where the tumor was located.
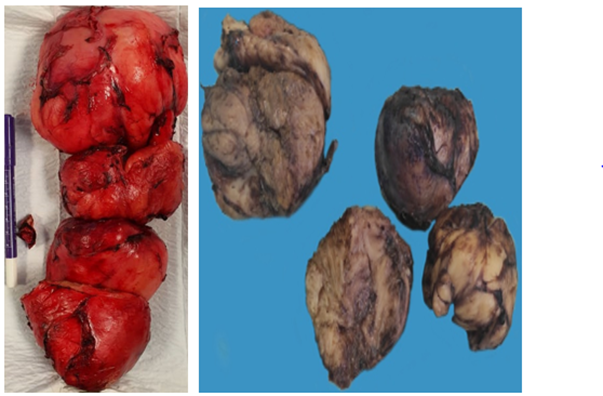
Figure 9,10: Completely removed ganglioneuroma (from 4 parts) solid tumor mass, with a grayish-white cut surface and whorled appearance
The postoperative course is satisfactory. The postoperative thoracic drain is partially active. Meropenem an 800mgx3, Vancomycin a 200mgx3, Metronidasol a 150 mgx3 are prescribed. A control X-ray is done and the drain is removed on the 5th postoperative day (fig. 11). Clinical patient satisfactory. On the 8th postoperative day, control laboratory parameters are performed, which are satisfactory. The control X-ray pulmoetcor shows a normal finding with a slight mantle pneumothorax. The patient is in a good general condition. The patient is discharged on the 8th postoperative day.
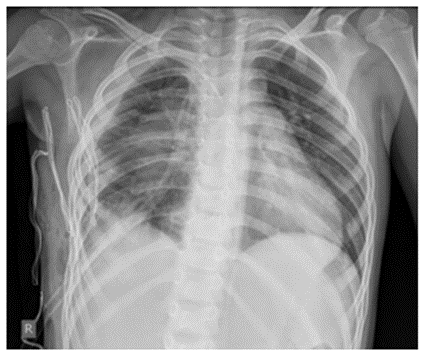
Figure 11: Chest Rtg Reexpansion of lung parenchyma and broken 6th rib on the right.
Pathohistological analysis showed a benign ganglioneuroma (figure. 12,13).
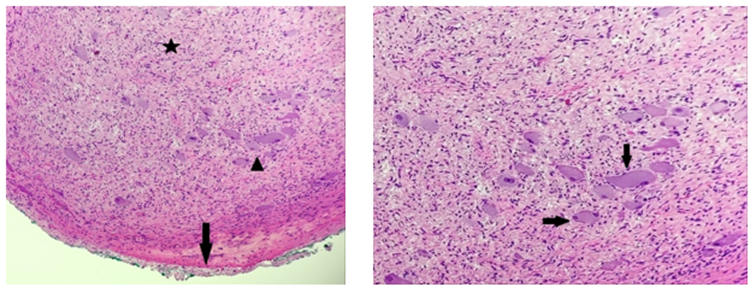
Figure 12: The microscopically tumor is well-circumscribed with fibrous capsule (arrow). Ganglioneuroma is consistent of bundles of Schwann cells (asterix) arranged in fascicles with individually dispersed mature and maturing ganglion cells(arrowhead).
Figure 13: The ganglion cells vary in size and shape, contain one to three nuclei, have abundant eosinophilic cytoplasm (arrow).
We followed the patient for a year and the control X-ray after 1 year showed a satisfactory finding (fig 14)
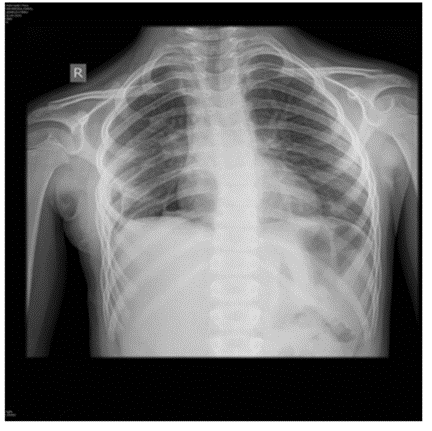
Figure 14: Control X-ray chest after 1 year shows a satisfactory condition.
Analyzing the literature and comparing the illness of our seven-year-old boy, we found that ganglioneuroma, there is usually a natural limit to tumor size given by the available space within the body cavity. We compared the size of the tumor in our patient 125x115x165mm with biggest resected GN assessable through literature research up to now showed a maximum diameter of approximately 23 cm [8] in a 42-year-old patient located solely thoracically [8]. Located most commonly in the posterior mediastinum (41.5%) such as our case report or retroperitoneally (37.5%), ganglioneuromas can be found in the adrenal glands (21%), in the neck (8%), retropharyngeally, or more rarely in the sella turcica [9-12]. Computed tomography (CT) or magnetic resonance imaging (MRI) represents the gold standard for diagnosis and estimation of tumor extent. The CT scan that we had provided accurate relationships with the surrounding structures, showing the compressive effect of the tumor, and thus helped us in making an accurate surgical plan [13]. Our patients ganlioneuroma was hormonally inactive. Ganglioneuromas show neuroendocrine potential which is attributable to their origin from the sympathetic neural crest, but the majority of them are reported to be hormonally inactive [14]. However, GNs have shown to have a secretory function in up to 39% of cases in some studies [15].
Malignant degeneration of a ganglioneuroma occurs rarely, with the highest prevalence occurring when tumors are penetrating into the spinal canal via the neural foramen, with transformation into neuroblastoma [16-19]. We performed a complete resection and removal of the tumor. Complete surgical removal is recommended for symptom control or prevention of potential malignant degeneration [20]. A control examination and control X-ray of the chest one year after the operation showed satisfactory results. Subsequent long-term follow-up including imaging controls is mandatory to prevent potential relapse, especially when only partial tumor removal was achieved. There is no need for neoadjuvant or adjuvant antineoplastic treatment. Additionally, prognosis after total tumor resection is deemed to be excellent, although surgical morbidity has to be taken into account especially when dealing with large GN.
Ganlioneuromas of the mediastinum are slow-growing, large tumors, mostly asymptomatic, and the first symptoms are a consequence of the compressive effect of the tumor. The gold standard in the diagnosis of ganglioneurinoma is CT and needle biopsy. Complete surgical removal is recommended for symptom control or prevention of potential malignant degeneration. Subsequent long-term follow-up including imaging controls is mandatory to prevent potential relapse.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
