
Case report | DOI: https://doi.org/10.31579/2578-8949/104
Department of Medicine, Defence Services Medical Academy, Mingalardon 11021, Myanmar
*Corresponding Author: Khin Phyu Pyar
Citation: Khin P. Pyar, Khine K. Su, Wunna K., Win K. K. Ko Min, Soe W. Hlaing at el. (2022) A case of Cervical Cold Abscess Refractory to Empirical Anti-Tubercular Therapy due to Mycobacterium Fortuitum: Awareness on Non-Tuberculous Mycobacteria (NTM) Infection! Dermatology and Dermatitis. 7(3); DOI:10.31579/2578-8949/104
Copyright: ©2022 Khin Phyu Pyar, this is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 August 2022 | Accepted: 20 August 2022 | Published: 05 September 2022
Keywords: cold abscess; tuberculous lymphadenopathy; non-tuberculous mycobacteria (NTM); mycobacterium fortuitum;
A third-year medical student, 19 years, had multiple cold abscess at left posterior triangle with systemic symptoms- poor appetite and weight loss. Histopathology was consistent with tuberculous lymphadenopathy as it showed Langham’s giant cells and caseation necrosis. Both systemic symptoms and local lesions were refractory to empirical treatment for tuberculosis standard anti-tubercular therapy: isoniazid, rifampicin, ethambutol and pyrazinamide. Pus for Gene Xpart was negative. Pus culture showed non-tuberculous mycobacteria (NTM); Mycobacterium fortuitum.
The aetiology of cold abscess is mainly due to tuberculosis i.e Mycobacterium tuberculosis; therefore, it resolves with standard anti-tubercular therapy. However, it may be rarely due to NTM infection.
Infections caused by NTM are increasing particularly in developing countries; and, NTM causes severe respiratory, skin and mucosal infections in humans. They are difficult to treat as it has intrinsic resistance to many common antibiotics (Johansen et al., 2020). NTM includes all Mycobacterium infection except Mycobacterium tuberculosis; they are Mycobacterium fortuitum, Mycobacterium abscessus, Mycobacterium intracellulare, Mycobacterium avium and Mycobacterium simiae.
Mycobacterium fortuitum is a rapidly growing mycobacteria, generally of low virulence; however, it is capable of causing a wide spectrum of infections (De Groote & Huitt, 2006). It causes skin and soft-tissue infection producing slowly progressive granulomatous disease. Pulmonary disease and disseminated infection are relatively uncommon (Gebo et al., 2002) though there were case reports; “Mycobacterium fortuitum infection in previously healthy lung” (Park et al., 2008) and those with underlying cystic fibrosis (Johansen & Kremer, n.d.). Moreover, it rarely caused peritonitis in patients on chronic peritoneal dialysis (Hamade et al., 2014) , acute central nervous system infection in patient with ventriculoperitoneal shunt (Xess et al., 2019), choroidal granuloma (da Silva Neto et al., 2019), disseminated folliculitis (Macente et al., 2013) and retroperitoneal cold abscess (Nguyen et al., 2009).
A 19-year-old girl, third year medical student had COVID-19 infection in third wave; she had fever and cough for one week. She recovered with symptomatic treatment; she was back to normal for one month. Later on, she had poor appetite for 3 months and also noticed weight loss 9 pounds (95 lb to 86 lb) over that period. Then, she noticed painful swelling in left side of neck with fever [1].

Figure: (1) Self photo showing swelling at left neck
There was no dental problem or swallowing problem. There was no organomegaly or other lymphadenopathy. She had BCG vaccination; there was no history of tuberculosis before.
Blood for complete picture was normal apart from mild anemia (Hb 10.9
gm%, Total WBC 7.3 x 109 /L, N 57%, L34 %, M7%; platelet count 339 x 109 /L), ESR 35 mm/1st hr. Chest radiograph revealed calcification in hilar area compatible with old healed primary complex; no parenchymal lesion [2].

Figure: (2) CXR revealed hilar calcification suggestive of old healed primary complex
On examination, 4 cm tender left cervical lymphadenopathy at posterior triangle with features of abscess was noted. Lymph nodes in other areas were not palpable. Tonsils were normal. ENT surgeon did incisional biopsy; brownish pus 3 cc was drained. The culture was sterile. The histopathological sample showed giant cells with caseous necrosis. Figure [3, 4, 5]

Figure: (3) Low power view showing multiple area of caseation necrosis in the cervical lymph node biopsy

Figure: (4) Low power view showing multiple area of caseation necrosis with Langhan’s giant cells in the cervical lymph node biopsy

Figure: (5) Large area of caseation necrosis
Therefore, she was treated as a case of tuberculous cervical lymphadenopathy with isoniazid, rifampicin, ethambutol and pyrazinamide. Her appetite was still poor; moreover, she still had intermittent fever.
Three months later, there was another swelling below previous lesion; and, it was painful. Apart from cold abscess, no new physical finding was noted. Figure [6] As it had features of abscess, incision and drainage was done. Pus for culture was sterile.

Figure: (9) recurrence of abscess in upper old scar with healed lower scar after 4 months anti-tubercular therapy
Anti-tubercular therapy was continued while waiting for culture results of Mycobacterium tuberculosis. Figure [7] & Figure [8] showed progress. She had poor appetite and felt unwell.

Figure: (6) old incision scar with 2 abscesses below after 2 months anti-tubercular therapy

Figure: (7) old incision scar with 2 abscesses below after incision and drainage after 2 months anti-tubercular therapy

Figure: (8) old incision scar with healing lower one after 3 months anti-tubercular therapy
After 4 months of anti-tubercular therapy, a small abscess with underlying 1 cm indurated area was noted over the old healed scar. Figure [9].
After several negative cultures of the material drained from the abscesses, finally one of the cultures isolated the agent Mycobacterium fortuitum. Therefore, anti-tubercular therapy was discontinued; clarithromycin and ciprofloxacin were initiated. Three days later, she had good appetite and felt better. The small abscess over old upper scar resolved over one months. Figure [10].
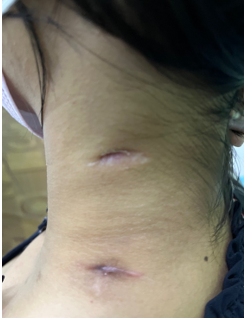
Figure: (10) Improvement two weeks after treatment for non-mycobacterium tuberculosis
First, the patient had poor appetite following COVID-19 infection; she recovered completely within few weeks. One month later, she lost her appetite with significant weight loss for 3 months. Then, she noticed painful swelling in neck. The scenario should not be confused with long COVID syndrome as the patient had complete recovery period for one month. It highlighted the importance of history taking.
The patient had unilateral cervical lymphadenopathy with cold abscess. Typical tuberculous cervical lymphadenopathy is usually bilateral; and, unilateral involvement is not common. It is one of the reasons for presenting this case.
The diagnosis of tuberculous cold abscess was confirmed with histopathological examination; therefore, empirical anti-tubercular therapy was prescribed. However, the patient’s appetite was still not good with ongoing weight loss with definitive treatment; empirical anti-tubercular therapy. The important differential diagnosis to be considered at this point were drug resistant Mycobacterium tuberculosis, non-mycobacterial (NTM) infection like Mycobacterium fortuitum, nocardiosis and actinomycosis; they could be differentiated by special culture and sensitivity. Drug resistant Mycobacterium tuberculosis is common in pulmonary tuberculosis; not with cold abscess. In actinomycosis, typical yellowish sulfur granules can be seen in discharge. Bacterial cultures and pathology are the cornerstone of diagnosis.
Moreover, untoward effects of anti-tubercular drugs causing poor appetite could not be ignored in this case. If poor appetite was due to drug side effect, the local abscess should be responsive. Having both local lesion unresponsiveness and persistence of poor appetite gave a clue to different aetiology/causal organism in this case.
Side effects of standard anti-tubercular therapy are common. Are the patient suffering side effects of drugs? Isoniazid, rifampicin and pyrazinamide commonly cause hepatotoxicity; jaundice, nausea and raised liver parenchyma enzymes are clue to drug induced hepatitis. In this case, liver function tests were normal; therefore, the appetite problem could not be explained with side effects of drugs.
Mycobacterium fortuitum is notorious for anti-microbial resistance. The case presented with unilateral lesion with marked systemic features; and, systemic features as well as local lesion improved with clarithromycin and ciprofloxacin which are sensitive for Mycobacterium fortuitum.
Both histopathological and special microbiological services are essential for NTM infections. High index of clinical suspicion for NTM is important if cold abscess is not responding to standard anti-tubercular therapy. Mycobacterium fortuitum is often regarded as one of the most antibiotic-resistant mycobacteria, leaving us with few therapeutic options. With an increasing prevalence of NTM worldwide, all clinicians should recognize and treat NTM infections
The authors would like to thank the patient for giving consent to this article. Also, to all doctors and nursing team for making great efforts in caring him. The authors acknowledged the following team; Professor Kyaw Min Oo, Senior Consultant ENT surgeon, Professor Myint Zaw, Professor Kyaw Zay Ya and Professor Ko Ko Lwin for administrative support.
The authors declared no potential conflicts of interests with respect to authorship and publication of this article.
Our institution does not require ethical approval for reporting cases.
The authors received no financial support for publication of this article
The informed consent for publication in this article was obtained from patient.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
