
Case Report | DOI: https://doi.org/10.31579/2690-8794/066
*Corresponding Author: Priyanka Mishra, Department of Anesthesiology and Critical care, All India Institute of Medical Sciences, Rishikesh, India.
Citation: Mishra P, Gupta B. and Parameswaran P., (2021) A case of bradycardia and hypersensitivity with intravenous ketamine monotherapy. Clinical Medical Reviews and Reports 3(2); DOI: 10.31579/2690-8794/066
Copyright: © 2021 Priyanka Mishra, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 January 2021 | Accepted: 13 February 2021 | Published: 20 February 2021
Keywords: bradycardia; hypersensitivity; intravenous ketamine monotherapy
Anaphylaxis during anesthesia is an unforeseeable and potentially life threatening syndrome that is dose independent. Ketamine is a widely used hypnotic for procedural sedation in the emergency department, in anesthesia and intensive care units (ICU). It is popularly employed for both children and adult patients. Though, dose dependent adverse effects of ketamine have been described, the hypersensitive reactions with the same are extremely rare. We are hereby presenting a case of an allergic reaction and isolated bradycardia with ketamine, given as intravenous monotherapy in a patient with no previous history of atopic disease. Our article aims at reminding all the medical professionals to never let a drug (however commonly used) throw away caution, be vigilant to timely diagnose an adverse drug reaction (even the most infrequent and rare) and be prepared to tackle the worst with the necessary supportive measures like hemodynamic support and advanced airway procedures.
The incidence of anaphylactic reactions during anesthesia ranges between 1 in 4000 to 1 in 25,000 and the mortality is estimated to be between 3 to 6% [1]. These are commonly seen with latex, neuromuscular blockers, opioids, antibiotics and blood transfusion etc. Though, dose dependent adverse effects of ketamine have been described, the hypersensitive reactions with the same are extremely rare. After taking informed consent for possible publication in literature, we are presenting such a rare case of intravenous ketamine allergy accompanied with bradycardia.
A 53 year old, 52 kg female patient was posted for incisional hernia repair under general anesthesia. She had an uneventful history of two caesarean section and one hernia surgery in the past. The anesthetic records of these surgeries were unavailable. Our anesthesia team was conducting a study regarding propofol induced pain in which intravenous (IV) ketamine was one of the test drugs. Post randomization, this patient was allocated to the ketamine receiving group. The study involved achieving venous stasis by inflating a tourniquet on the arm in which the selected drug would be given. Inside the operating room, the baseline vitals were recorded as heart rate (HR) - 62/min, Blood pressure – 106/64mm Hg and oxygen saturation (spO2) of 99% on air. After securing venous access and tourniquet inflation at 100mm Hg, we began to give the sub-anesthetic dose of ketamine (15mg) IV. Patient immediately complained of burning sensation and itching over the forearm so further administration was stopped and tourniquet released.We noticed red macular spots that evolved into morbilliform, blanchable rash over the forearm and hand below the tourniquet. There was a transient fall in HR to 45/min that resolved spontaneously. However, there was no associated change in respiration or blood pressure. Suspecting an allergic reaction to the given drug, we gave inj. hydrocortisone 100 mg and inj. pheniramine 45.5 mg IV stat. This was followed by regression of rash. Patient was then induced and surgery commenced. Patient was extubated uneventfully at the end of procedure. However, still the rash had not resolved completely.
Ketamine hypersensitivity test was done later by an intradermal injection of 1mg/ml ketamine both 2 days and 6 weeks after surgery.
Differential diagnosis
The possibility of these lesions being petechiae induced by the tourniquet was ruled out as they were blanchable and the coagulation profile and platelet count was normal in the patient.
Outcome and follow-up
While the control using normal saline was negative (Figure 1), redness with eruption of size 13 mm and 12 mm respectively at 2 days and 6 weeks with ketamine confirmed positive tests (Figure 2).


Based on the clinical history, examination and investigations, we formed a diagnosis of ketamine induced hypersensitivity.
Ketamine, a phencyclidine derivative, is a commonly used agent in both children and adults for sedation, analgesia and intravenous induction. Despite frequent use, the hypersensitivity reactions to ketamine appear to be extremely rare. A meta-analysis by Bellolio et al. revealed no cases of anaphylaxis in 13,883 pediatric sedations, most of whom received ketamine [2]. Common side effects of ketamine include over-sedation, tachycardia, increased secretions, vomiting, laryngospasm, confusion and hallucinations. Bradycardia and hypotension are very infrequent side effects. There are few case reports on allergy and anaphylaxis but most of them involved co-administration of other agents. Bylund et al have described anaphylaxis by intramuscular ketamine as monotherapy [3]. In another case report, an allergic reaction with intravenous ketamine infusion for procedural sedation in the emergency department has been documented [4]. Several factors make the assessment of allergic response in an anesthetic-related reaction difficult. These include the fact that induction drugs are generally administered in quick succession rendering it difficult to identify the actual culprit for hypersensitivity and the clinical manifestations like tachycardia or hypotension can get altered by these concomitantly administered drugs. Draping may prevent the early detection of signs like urticaria or angioedema. It should be noted that history of atopic disease constitutes a risk factor for development of drug allergy and thus, shall be carefully inquired in the pre-anesthetic evaluation. Guyer et al. showed that 55% of patients reported drug allergy history, 48% of them had history of allergic rhinitis, 32% were diagnosed asthmatic, 15% reported a positive history of a severe allergic reaction [5].
We are presenting a case of hypersensitivity to ketamine in a female patient with no previous history of allergy or atopy. As no other drug was administered to the patient before ketamine, the suspicion of ketamine allergy was high. Owing to the low dose of drug given and tourniquet inflation leading to venous stasis in our case, severe systemic response was prevented. Hence, we did not confront life-threatening respiratory or cardiovascular compromise in our case. The transient isolated bradycardia (without other cardiovascular abnormalities) that was witnessed resolved spontaneously. Sheth et al have postulated that oldage, lower baseline vitals, and non-trauma patients are more likely to predict the occurrence of bradycardia after ketamine injection [6]. We believe that the old age and low baseline heart rate could have resulted into the bradycardia response. Benzethonium chloride was the preservative in our ketamine supply. The hypersensitivity test with benzethonium chloride came out to be negative. None of the other patients who were given ketamine from the same vial had any allergic response. There can be development of morbilliform petechial eruption due to tourniquet inflation in thrombocytopenic patients [7]. However, the blanching character of the rash and normal platelet count ruled out that suspicion. The differential diagnosis in our case may include an allergic reaction to latex or ketamine. Latex allergy was ruled out by the history of uneventful previous surgeries where latex gloves were used. Ketamine hypersensitivity was later confirmed by a positive intradermal test. Tryptase level assessment was not available in our institute. The skin testing can be conducted at least four to six weeks after the occurrence of a suspected perioperative allergic reaction, thus allowing for the clearance of suspected drugs and anti-allergic medications [8]. We had attained positive results for ketamine sensitivity in both the tests done on second day and six weeks post operatively. The symptoms in our patient and their improvement with anti-histaminics and steroids were consistent with activation of mast cells and release of mediators like histamine. The Naranjo Adverse Drug Reaction Probability Score was ten indicating a definite ketamine related adverse drug reaction. (Table 1)
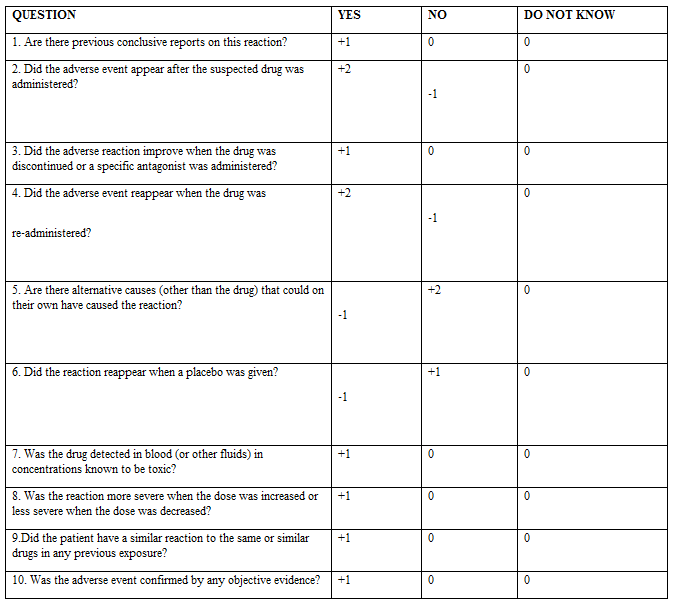
Total score in our case - 10 (DEFINITE)
1 Doubtful
1-4 - Possible
5-8- Probabe
>9 – Definite
Few studies indicate that ketamine induced allergy is mediated by histamine release and the evidence indicated against an IgE mediated response. However, whether this was the sole mechanism cannot be declared with certainty as there was not complete resolution of rash despite before said treatment. As ketamine does not have a reversal agent, once administered, the physician must be ready to handle the consequences. The only feature of anaphylaxis may be characterized by airway obstruction or cardiovascular collapse in the perioperative period. After an adverse drug reaction, the agent should be discontinued at the earliest. Adequate oxygenation with 100% oxygen, antihistaminic agents (diphenhydramine, pheniramine), corticosteroids (dexamethasone, hydrocortisone), bronchodilators and epinephrine may be administered to control the allergic response. It is essential to avoid the allergen for all future purposes. To the best of our knowledge, there is no published literature documenting incidence of bradycardia with intravenous ketamine hypersensitivity.
Our report aims to send a reminder to all the medical professionals to be highly vigilant and prepared for the rare potentially fatal allergic responses to commonly used drugs. Isolated bradycardia (in absence of other cardiorespiratory abnormalities) and hypersensitivity with intravenous ketamine is a very rare occurrence. All necessary supportive measures like hemodynamic support and advanced airway procedures shall be readily available to efficiently tackle such situations.
Learning points/take home messages
No potential conflict of interest relevant to this article was reported
Not applicable.
None.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
