
Case Report | DOI: https://doi.org/10.31579/2690-4861/862
*Corresponding Author: Yaghoobi Gholamhossein, Department of ophthalmology, Birjand University of Medical Science.
Citation: Yaghoobi Gholamhossein, (2025), A Brief Review of Optic Nerve Head Abnormality and Report Three Cases, International Journal of Clinical Case Reports and Reviews, 28(2); DOI:10.31579/2690-4861/862
Copyright: © 2025, Yaghoobi Gholamhossein. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 May 2025 | Accepted: 09 June 2025 | Published: 31 July 2025
Keywords: abnormalities; ophthalmology; optical coherent tomography
Congenital Optic disc anomaly have conflicting feature that sometimes it will be difficult to differentiate acquired or congenital entity of each other. This anomaly in spite of rarity but diagnosis of many congenital or acquired optic disc derangement is a diagnostic dilemma. So it need clinical and paraclinical study which in this report discuss the variety of clinical and paraclinical finding of them.
One of the rare abnormalities of the optic disc is congenital optic nerve head pit. This lesion, if accompanied by macula involvement, causes progressive vision loss due to failure of the embryonic cleft to close during the developmental period in the optic nerve head.
Only 15% of cases are bilateral, and its incidence is one in 11,000 people, with no difference in the two sexes. Unilateral cases are hereditary and are seen as autosomal dominant. [1]
There is no consensus on the cause of its embryonic origin, and its physiopathology in the formation of intraretinal or sub retinal fluid is not completely clear. [2] Although the majority believe that the origin of this edema is either from the vitreous fluid or from the cerebrospinal fluid. Since a normal eye has a closed system and its different parts have a slight pressure difference between them, the pitting of the optic nerve head may cause the transfer of cerebrospinal fluid to the retina or vice versa. [2] In this report, we present three cases of optic nerve head abnormalities with clinical and pathological manifestations conflict, two of which were accompanied by maculopathy and obvious optic disc anomalies and one case with peripapillary atrophy indeed of macular edema in the macula-papilla area. So, there is diagnostic conflict which not only the clinical examination but also Para clinical examination could be done for diagnostic purpose.
The first case is a 12-year-old boy with decreased vision. On examination, the visual acuity of the right eye was 10/10 without correction and the left eye was 10/5. On fundus examination, as seen in Figure 1, serous retinal detachment is evident as a balloon appearance, and cystic edema is also seen on optical coherent tomography (OCT). The retina of the left eye is normal, and other examinations of both eyes are normal in terms of eye examination.

Figure 1: Fundus photo and OCT of both eye
The second case is a 10-year-old boy. The visual acuity of the right eye is 10/3 and the right eye is 10/10. The anterior segment examinations of both eyes are normal. On fundus examination, the nerve head appearance in the right eye is sunflower-shaped and the left eye also has a coloboma-like appearance.

Figure 2: Fundus photo and OCT of both eye
Another case is a 45-year-old individual with peripapillary atrophy, as seen in Figure 3. There is evident prepapillary atrophy on the optic nerve head which apart from its cause has a similarity to congenital disorder resembling congenital optic disc anomaly. Although the maculopathy showed retinal edema, hemorrhage and prepapillary atrophy and cystic change in OCT which is obvious in figure 3.
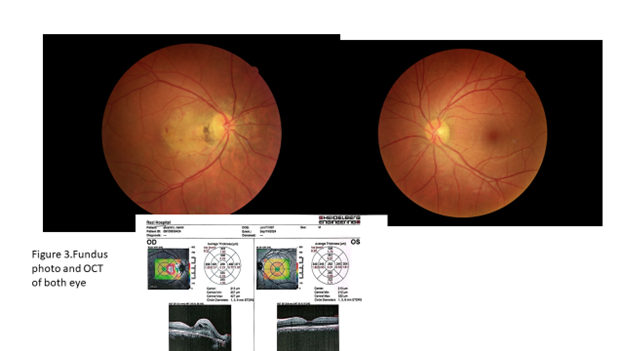
Figure 3: Fundus photo and OCT of both eye
Congenital optic nerve head disorders are rare and since they are most often discovered incidentally, this congenital anomaly must be distinguished from other similar lesions of the nerve head, whether acquired or congenital. Considering that retinal imaging, from fundus photography to OCT, is currently of great help in distinguishing them from each other, some of these types of anomalies have similar clinical manifestations.
In this review, we have illustrated 3 different cases of optic nerve head abnormality to be helpful when dealing with such lesion in differentiate them. So, separation and definitive diagnosis of each other plays a role in follow-up and treatment. The first case is located in the temporal part of optic disc and in the transverse line, its clinical appearance shows a transverse bell shape figure serous macula detachment clinically. The second case have a pit-like appearance which is located in the temporal region and has a view of the sunflower nerve head anomaly. The other eye has a similar view of the nerve head coloboma like abnormality clinically in fundus view. The extensive prepapillary atrophy in the third case could indicate repeated serous detachments that most probably be secondary atrophy and vascular changes. Although to find the definite diagnosis it needed more paraclinical evaluation. A study by Patel, Megha B et al supposed to differenciate such varity of optic disc anomaly. [3] Optic disc holes and morning glory disc anomaly both serve as differential diagnoses for each other. OCT showed subretinal fluid and intraretinal cystic spaces in our case. Various possibilities have been suggested such as vitreous infiltration through macular hole formation, cerebro spinal fluid infiltration from the subarachnoid space through the optic disc pit defect, leakage from blood vessels in the optic disc pit defect and fluid from the choroid, through Bruch's membrane, and peripapillary atrophy. Thus, the diagnostic dilemma between morning glory disc anomaly and optic disc pit was resolved using OCT angiography. [4]
Unfortunately, these aforementioned cases did not cooperate or did not refer despite requests for follow-up and imaging. This cases indicates the specific location of the pit is not diagnostic especially in all cases in the temporal region, unlike report 1, which was seen in the inferior temporal region. Therefore, congenital optic disc anomaly have broad spectrum that differentiation of each one needed clinical and paraclinical evaluation.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
