
Review Article | DOI: https://doi.org/10.31579/2767-7370/111
1 Obgyn PGY-1 at Dubai Health, United Arab Emirates (UAE).
2 Consultant Obgyn at Dubai Health, United Arab Emirates (UAE).
*Corresponding Author: Asma Marwan Al-Rawi, Obgyn PGY-1 at Dubai Health, United Arab Emirates.
Citation: Asma Marwan Al-Rawi and Laila Yahya Al-Hubaishi, (2024), A Brief Overview About Postpartum Urinary Retention, J New Medical Innovations and Research, 5(6); DOI:10.31579/2767-7370/111
Copyright: © 2024, Asma Marwan Al-Rawi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 July 2024 | Accepted: 10 July 2024 | Published: 22 July 2024
Keywords: cesarean deliveries; postpartum; urinary retention; vaginal deliveries
Background: Postpartum urinary retention (PUR) or puerperal urinary retention is quite a common obstetric condition affecting postpartum women. Despite its significance, ubiquity, and morbidity, it remains an under-discussed and poorly understood topic.
Objective: This literature review is aimed to examine the latest research and findings in the field, with a focus on three key areas: the incidence and risk factors of PUR, the comparison of PUR in vaginal versus cesarean deliveries, and the management and prevention strategies. Since we believe it needs to receive more attention and awareness.
Conclusion: In conclusion, PUR is a complex condition with varying incidence and contributing factors. Understanding its pathophysiology, risk factors, and effective management strategies is essential for better outcomes in postpartum care.
Urinary retention (UR) is the inability to empty the bladder normally. Postpartum voiding dysfunction is defined as failure to pass urine spontaneously within six hours of vaginal delivery or catheter removal [45]. Another common clinical definition of urinary retention is significant post-void residual bladder volume (PVRBV), where PVRBV is defined as the volume of fluid remaining in the bladder immediately following the completion of micturition [8, 30, 69]
The presence of PVRBV implies an imbalance between the forces of urine expulsion and the outflow resistance or a failure or decrease in detrusor contractility. Accordingly, a significant PVRBV represents an abnormality of bladder function and could be used as the definition of PUR. Postpartum urinary retention (PUR) is a common condition in obstetric units. It is also known as puerperal urinary retention or insidious urinary retention after vaginal delivery [61]. If postpartum voiding dysfunction is not diagnosed promptly, it can lead to bladder over-distension and activity, and prolonged voiding dysfunction, with sequelae such as incontinence and recurrent urinary tract infections (UTIs), [16].
The definition of PUR varies among studies. Yip et al. (1997) divided PUR into overt and covert urinary retention, with overt PUR defined as an inability to urinate autonomically 6 h after vaginal delivery or the need for re-catheterization 6 h after catheter removal following cesarean section. Carley et al. (2002) defined PUR as an inability to undergo spontaneous micturition within 12 h after vaginal delivery. However, other reports defined PUR as a symptom requiring at least one catheterization within the first 24 h postpartum [10,50].
Bladder symptoms that should raise clinical suspicion of voiding dysfunction include urinary frequency, voiding small amounts, slow or intermittent stream, bladder pain or discomfort, straining to void, reduced sensation to void, incomplete emptying of the bladder and urinary incontinence [15, 17]. PUR can be silent, and some women may be unaware of the large volume of urine in the bladder or that they are unable to void to completion. This may occur because of reduced bladder sensation and contractility due to injury or trauma to the nerves supplying the bladder [43].
The reported prevalence of PUR varies widely ranging from 1.7%–17.9%. In a recent study, the overall prevalence of PUR was 12.9 % [64]. There is increased risk of voiding dysfunctions leading to PUR in the postpartum period due to the physiological changes and traumatic events occurring during pregnancy and childbirth [47]. The reported incidence of postpartum voiding dysfunction varies considerably due to differences in the definition, methods of diagnosis, and mode of delivery. Overt UR incidences range from 0.45%, 1.7% to 17.9%, and from 0.05% to 37% have been reported [38].
The incidence of UR following cesarean section varies between 3.38% and 11.5% [60]. However, if post-void residuals are not checked and recorded, it may not be possible to identify these women. As a result, the actual incidence may be higher than reported, and as many as 5% of these women may have significant and long-term bladder dysfunction [32].
Two types of urinary retention can affect a woman in the postpartum period [59]. PUR is classified as overt, which is defined as the inability to void spontaneously within 6 h of either vaginal delivery or catheter removal after delivery [36]. Overt or symptomatic urinary retention is easily detectable, with clear clinical appearance, and therefore is adequately treated (Figure 1), [19].
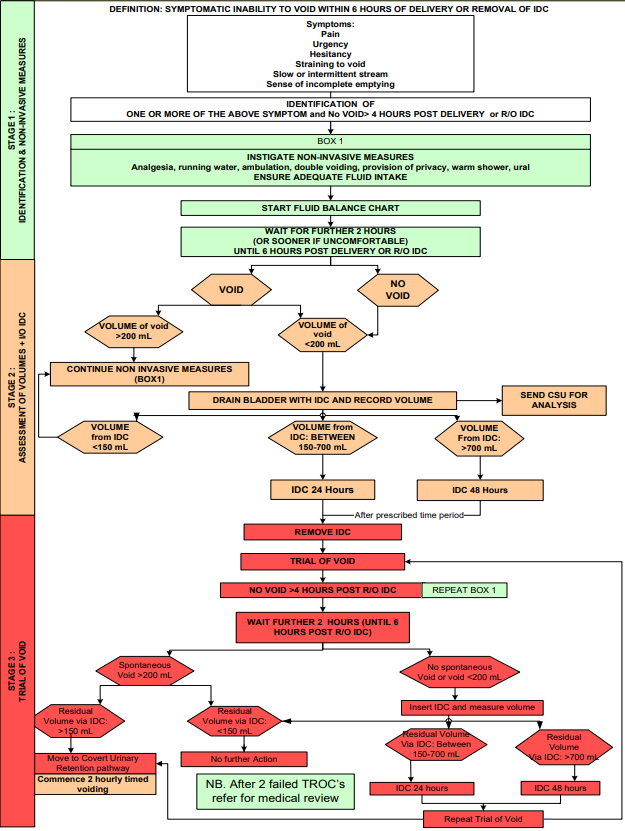
Figure 1: Postpartum overt urinary retention
The covert form can be identified by elevated post-voiding residual volume (PVRV) measurements, using ultrasound scanning or catheterization after urination [18]. It occurs when a woman passes small amounts of urine and has an elevated post-void residual urine volume greater than 150ml with no symptoms of UR (Figure 2), [21].
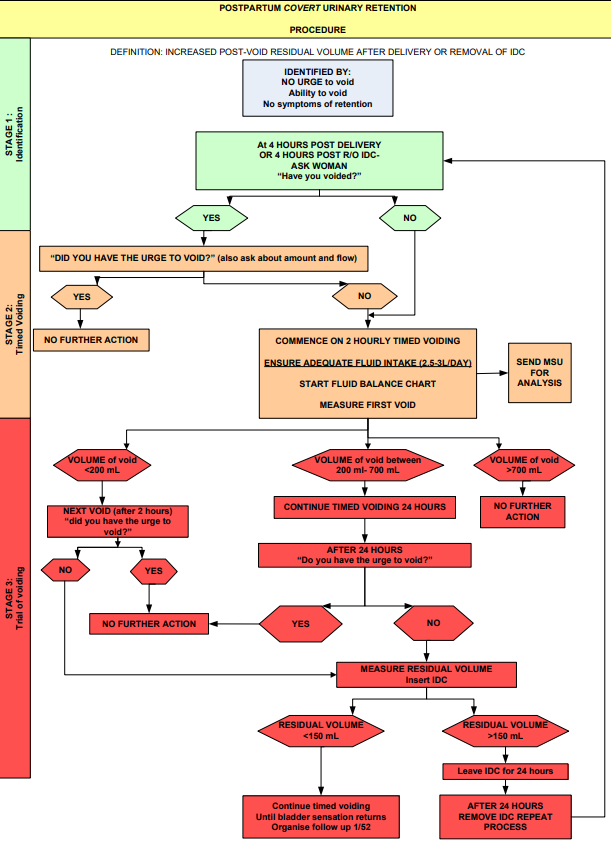
Figure 2: Postpartum covert urinary retention.
The pathophysiology of PUR is not well understood; however, several hypotheses exist regarding physiological, neurologic, and mechanical factors related to pregnancy and the immediate postpartum period [25]. The bladder is a hormone-responsive organ. Pregnancy-related changes, including increased progesterone, reduced bladder muscle tone, increased capacity, increased urethral length, and increased maximal urethral closure pressure may contribute to PUR development [40].
During pregnancy and immediately postpartum, increased progesterone levels inhibit smooth muscle tone and may contribute to detrusor inhibition [27]. Impaired detrusor contractility combined with a lack of urethral relaxation may explain a component of the urinary retention mechanism [9]. One study demonstrated that pregnancy induced a 50 percent decrease in bladder muscarinic receptor density, which correlated with a 50 percent decrease in the contractile response to bethanechol [43].
Another PUR mechanism involves pelvic, hypogastric, and pudendal nerve injury during delivery [2]. Neurologic consequences vary depending on the complex interactions of partial or complete injuries with the parasympathetic, sympathetic, and somatic nervous systems [67]. Sympathetic nerve injuries result in decreased bladder compliance and high storage pressures because of beta-adrenergic denervation, whereas parasympathetic nerve injuries produce a hypo contractile bladder with decreased sensation. These nerve injuries, which are typically transient in nature and resolve within three months postpartum, have been demonstrated through electrophysiological research [43].
During a vaginal delivery, ischemic nerve injury can occur from a prolonged second stage of labor, and direct partial or complete nerve transection can result from either spontaneous or operative birth trauma [55]. Denervation can occur during cesarean delivery in cases complicated by substantial hemorrhage or in those requiring a cesarean hysterectomy [55]. Regional analgesia acts as a potential iatrogenic contributor to PUR, directly affecting bladder sensitivity and contractility. It also temporarily disrupts afferent input arising from bladder stretch receptors, which may be damaged by overdistention intrapartum [46].
Periurethral and vulvar edema can lead to mechanical urethral obstruction and impaired voiding [9]. Pain associated with obstetrical lacerations may preclude relaxation of pelvic floor muscles, which is the first step in initiating a spontaneous void. Furthermore, patient discomfort with voiding in unfamiliar locations and lack of privacy are possible contributors to PUR [33].
Independent risk factors for PUR vary and are often limited by confounding factors. Frequently proposed risk factors include epidural anesthesia, operative vaginal delivery, prolonged labor duration, episiotomy, newborn macrosomia, nulliparity, and obstetric anal sphincter injury [5]. A systematic review of PUR risk factors found that operative vaginal delivery was the only clinical factor with a consistently strong association with PUR [39].
Operative vaginal delivery may result in direct pelvic floor and bladder trauma, edema that results in mechanical outlet obstruction, or impaired reflex and voluntary relaxation of the sphincter urethrae, periurethral muscles, and pelvic floor [4]. It is unclear whether operative vaginal delivery is an individual risk factor, or if it is confounded by other concurrent risk factors such as epidural, episiotomy, prolonged labor, and parity [43].
In a multivariate analysis, labor duration >700 minutes was the only factor that predicted PUR. Ultimately, multiple risk factors likely act synergistically to impair normal postpartum micturition processes > 700 minutes was the only factor that predicted PUR. Ultimately, multiple risk factors likely act synergistically to impair normal postpartum micturition processes [44].
The PUR was ascribed to maternal anxiety, nervousness, genital injuries, such as vulval and vaginal lacerations, and derangement of the neuromuscular innervation of the bladder. Some of these factors have been proven using urodynamics, electrophysiology, and histochemistry of the detrusor muscle. [30]
The evaluation of the patient with suspected urinary retention should begin with a detailed history to elucidate the precise etiology, as summarized in Table 1 [23]. The initial evaluation should also include a thorough medication history, including the use of over-the-counter medications and herbal supplements [58, 63].
| Potential etiology | History | Physical examination |
| Cystocele; rectocele; uterine prolapse | Pelvic pressure; palpation of a pelvic organ from the vagina | Prolapse of bladder, rectum, or uterus |
| Uterine fibroid, pelvic mass, or malignancy | Pelvic or lower abdominal pain, dysmenorrhea, bloating | Palpable uterus, ovaries, or adnexa |
| Vulvovaginitis | Vaginal discharge, vaginal itching, dysuria | Inflamed or erythematous vulva or vagina, vaginal discharge |
Table 1: History and physical examination findings that suggest etiologies of urinary retention [54].
Physical examination should include a complete abdominal assessment, including palpation and percussion of the bladder and abdominal/ pelvic organs; evaluation for flank tenderness; a complete pelvic examination in women; and a neurologic evaluation to assess strength, sensation, muscle tone, and reflexes relative to lower thoracic, lumbar, and sacral spinal levels [53, 54]
Testing should include a postvoid residual (PVR) urine evaluation, which is a simple, noninvasive, and cost-effective volume measurement of urine within the bladder that can be performed with ultrasonography [12]. The bladder can be percussed when it contains 150 mL of urine and is palpated with greater than 200 mL [65]. No evidence supports a specific PVR threshold for patients with chronic urinary retention; however, the American Urological Association has recommended using a value greater than 300 mL that has persisted for at least six months and has been documented on two separate occasions [1,57].
Postpartum evaluation of postpartum urinary retention
Patients should spontaneously void within 6 hours after the last bladder drainage or catheter removal [44]:
If PVR evaluation cannot be obtained or is thought to be inaccurate, patients with suspected urinary retention should be catheterized for bladder decompression and accurate measurement of stored urine [54].
Intermittent self-catheterization
When PUR is persistent, management with intermittent self-catheterization (ISC) or indwelling urethral catheter is indicated regardless of whether the patient is symptomatic [23]. This prevents further bladder injury by keeping the bladder decompressed while awaiting the return of normal bladder function [7]. The advantages of indwelling urethral catheter placement include complete bladder rest and lack of need for ISC teaching [6]. Disadvantages include increased infection risk, need for in-office voiding trials, and inability to monitor ongoing progress [44].
High fluid intake in mothers expressing milk coupled with postpartum diuresis and diminished bladder sensation may make it challenging to perform frequent self-catheterization and avoid overdistention [43]. To balance these challenges, we strongly recommend using an indwelling catheter for the first 5 to 7 days, followed by ISC if needed [42]. Whether to manage persistent PUR with ISC or with an indwelling urethral catheter is not well-studied, and no guidelines exist [24, 28].
Female urology referral
In some centers, urogynecology or female urology referral is placed when PUR is diagnosed or persists [34]. When these services are available, it is recommended that referral at the time of hospital discharge for women with unresolved PUR. These providers have AVT supplies, staff with expertise in teaching ISC, and the ability to perform additional testing. However, it is important to note that urodynamic testing and imaging studies are not routinely indicated for women with PUR and should be reserved only for women with atypical symptoms, a concerning history, or considerably prolonged PUR [37].
Acupuncture
Acupuncture has been studied for PUR treatment at the time of diagnosis in the immediate postpartum period. In a randomized trial of 55 women with PUR, 92% in the acupuncture group achieved spontaneous micturition within 1 hour following treatment [29].
Bethanechol chloride
Bethanechol chloride is a U.S. Food and Drug Administration-approved cholinergic medication for the treatment of acute postpartum nonobstructive urinary retention.38 Dosing begins at 5 to 10 mg, 3 times per day with dose escalation as needed. Side effects of bethanechol include flushing, tachycardia, diarrhea, vomiting, and urinary urgency [43].
Tamsulosin
Tamsulosin, an alpha-adrenergic receptor antagonist acting at the level of the bladder, neck, and urethra, is efficacious in preventing postoperative urinary retention in an Ur gynecological population [13].
Postpartum prevention and management
Prevention of PUR requires avoiding bladder overdistention during labor [31]. The American College of Obstetricians and Gynecologists recommended assessing all women for bladder emptying in the first 24 hours postdelivery to avoid PUR [25]. Normal urine output is defined as 0.5 to 1.5 mL/kg/h.27 We suggest inadequate urinary output be defined as 150 mL [26]. Either modality can be used to screen for an elevated PVR; however, precise bladder volumes should not be expected. For volumes ≥150 mL, a catheter should be used to assess the PVR accurately [14].
Figure 3 illustrates the postpartum bladder management protocol, developed by group consensus with the incorporation of a variety of protocols currently used nationally and internationally [62]. The algorithm begins with identifying overt or covert PUR, followed by step-by-step guidance for management and discharge disposition [43].
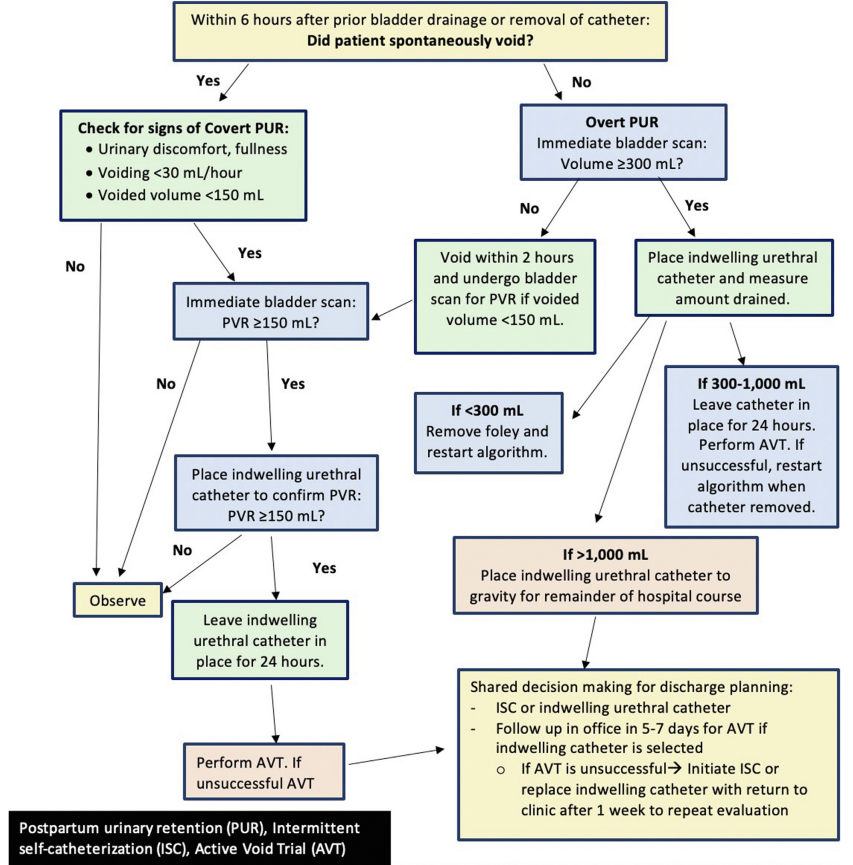
Figure 3: Postpartum bladder management protocol [43]
Postpartum voiding dysfunction following vaginal versus cesarean delivery
Labor is associated with pelvic floor disorders both voiding dysfunction and fecal incontinence [48]. Whether this is caused by pregnancy or delivery itself is unknown. The reported incidence of postpartum voiding dysfunction ranges between 1.7% and 43% following vaginal delivery [51]. Prolonged second stage, instrumental delivery, and high birth weight increase this risk [49].
Voiding assessment is a crucial part of postpartum care. This involves the determination of risk factors and early promotion of first urination. While most studies on postpartum voiding dysfunction were related to vaginal delivery, little is known about the effect of the mode of delivery (vaginal versus CD) on voiding dysfunction [69]. One study that compared postpartum PVRV in nulliparous following vaginal or CD, found that women after vaginal delivery had higher rates of PVRV compared to CD [3].
In elective CD, the operation is performed before uterine contractions and the fetal head is relatively high in the pelvis. Therefore, postpartum PVRV may be higher in the vaginal delivery group compared to CD. A recent study suggests that delivery adversely affects voiding function, and that vaginal delivery is associated with more severe bladder dysfunction compared to elective CD [52].
In conclusion, PUR is a complex condition with varying incidence and contributing factors. Understanding its pathophysiology, risk factors, and effective management strategies is essential for better outcomes in postpartum care.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
