
Case Report | DOI: https://doi.org/10.31579/2690-4861/500
1Faculty of Medicine, University of Balamand, Beirut, Lebanon.
2Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
3Department of Medicine, Lymphoma Service, Memorial Sloan Kettering Cancer Center, New York, USA.
4New York Proton Center, New York, NY 10035, USA.
†These authors contributed equally to this work
*Corresponding Author: Carla Hajj, Memorial Sloan Kettering Cancer Center, New York, NY 10027, USA.
Citation: Joseph Hajj, Melissa Hatem, Brandon Imber, Joachim Yahalom, Carla Hajj, (2024), A 50-year-old woman with chemo-refractory diffuse large B cell lymphoma of the head of the pancreas, cured with definitive radiation therapy, International Journal of Clinical Case Reports and Reviews, 18(4); DOI: 10.31579/2690-4861/500
Copyright: © 2024, Carla Hajj. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 July 2024 | Accepted: 15 July 2024 | Published: 29 July 2024
Keywords: diffuse large b cell lymphoma; chemotherapy; r-chop; pet; pancreatic cancer; radiation therapy; non-hodgkin lymphoma; chemo-refractory
Diffuse large B cell lymphoma (DLBCL) is the most common lymphoma, accounting for 30% of all non-Hodgkin lymphomas. It is most prevalent in elderly people and is usually associated with a poor prognosis. DLBCL is also classified as the most prevalent subtype of primary pancreatic lymphoma. Chemotherapy with combination drugs; rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone (R-CHOP) is the treatment of choice in the management of DLBCL. It proved effective outcomes in 50-60% of the cases. However, 10% of the patients are refractory and need more aggressive treatment modalities.
In this case report, we present a 50-year-old patient with localized DLBCL of the pancreas refractory to 6 cycles of R-CHOP chemotherapy and successfully treated with definitive radiation therapy.
The two main subtypes of lymphomas are Hodgkin and non-Hodgkin lymphomas. Both can present with B symptoms which include low grade fever, drenching night sweats and unintentional weight loss. When B symptoms are present, the likelihood of a poorer prognosis becomes higher [1]. Hodgkin lymphomas are usually localized and spread contiguously while non-Hodgkin lymphomas have a more advanced stage, do not spread contiguously, commonly have extra nodal involvement, and are associated with a worst prognosis. Reed Sternberg cells (CD15/CD30 positive and CD20/CD45 negative) are characteristic of Hodgkin lymphomas.
Diffuse large B- cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin lymphomas in adults (about 30%) [2], and is usually diagnosed in older patients, with a median age at presentation of 70 years [3]. The pathogenesis includes mutations in the BCL2 gene (an anti-apoptotic factor) and the BCL6 gene (a mediator of growth suppression) [4]. Many variants have been classified by the World Health Organization (WHO) and were mainly defined by anatomical site of involvement [5]. DLBCL is the most common subtype of primary pancreatic lymphoma (PPL), compromising 77-80% of the total cases [6,7]. The prognosis is variable and depends on the IPI (international prognostic index) score of the patient.
The standard of care treatment is R-CHOP: rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone. The co-expression of BCL2 and MYC, demonstrated by immunohistochemistry, has been associated with a worse prognosis in patients that were treated with R-CHOP [8,9]. After 1st line therapy, 50-60% of DLBCL patients achieve and maintain complete remission; around 30-40% relapse and 10% will be refractory [10,11].
We report a case of a 50 years old female patient who got diagnosed with localized DLBCL of the pancreas, refractory to 6 cycles of R-CHOP chemotherapy but successfully treated with radiation therapy.
The patient is a 50-year-old woman whose oncologic history goes back to July 2019 when she developed new onset of jaundice, pruritis, dark urine and clay-colored stools. She therefore underwent an ultrasound of the abdomen which showed mass around the head of the pancreas and a dilated common bile duct (CBD). A CT scan of the chest, abdomen and pelvis confirmed a 3.5 hypodense solid mass of the head of the pancreas and no other sites of disease. An MRI of the abdomen confirmed a 3.5 hypodense mass causing a mass effect on the CBD, in addition to enlarged peripancreatic lymph nodes, the largest measuring 2x2.5cm. An endoscopic ultrasound (EUS) showed again a localized pancreatic uncinate mass, measuring 43x28mm, in addition to enlarged nodes in the periportal area, with the largest node measuring 36x26mm. A fine needle aspirate (FNA) of the node was suggestive of a B cell lymphoma. A subsequent core biopsy of the pancreatic confirmed diffuse large B-cell lymphoma.
Germinal Center B-Cell like (GCB) subtype. A baseline PET scan showed FDG avid pancreatic head mass. A bone marrow biopsy was negative. The patient was treated with 6 cycles of R-CHOPx6, completed on 12/31/20. An interim and an end of treatment PET scans showed persistent focal FDG avidity within the pancreatic head, with an SUV of 24.5 (figure 1).
In February 2021, an EUS with FNA and core biopsy of the periportal lymph node confirmed persistent B-cell lymphoma of germinal center type after 6 cycles of R-CHOP.
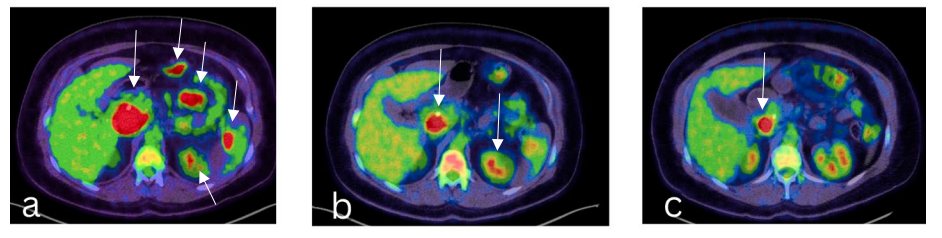
Figure 1: (a)-Baseline PET scan on 9/3/2020. (b) and (c)-PET scans on 11/10/2020 and 2/3/2021, respectively, showing partial response to R-CHOPx6 treatment; Images from our institutional radiology department.
The case was reviewed at the tumor board, and the consensus was to defer stem cell transplantation and proceed with definitive radiation treatment. The patient therefore received a total of 50Gy in 25 fractions (36Gy in 18fractions for the initial phase followed by a 14Gy cone down) between 04/28/21 and 06/02/21, in accordance with the recommendation of The International Lymphoma Radiation Oncology Group (ILROG) for the use of Radiation Therapy (RT) in hematological diseases [12] (figure 2). The patient was treated with deep inspiration breath hold (DIBH). Image-guidance was used with daily KVs, CBCTs and intrafractional monitoring. The patient was NPO 3 hours prior to her daily treatments.
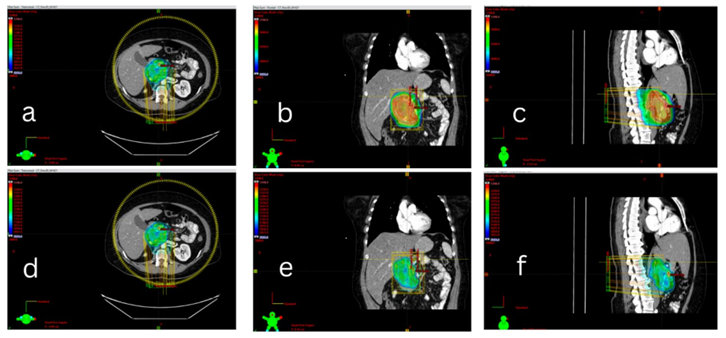
Figure 2: (a), (b) and (c)- 36 Gy coverage and (d), (e) and (f)- 50 Gy coverage; Images from our institutional radiology department.
A PET scan done in July 2021, approximately 6 weeks after the end of radiation therapy, showed a markedly decreased pancreatic lymphoma mass with residual small focus on FGD uptake slightly above liver activity, when compared to pet scan done on 04/16/2021. This focus was covered by the higher radiation dose (50Gy) and it was considered to be most likely inflammatory. No other FGD avid lesions were seen (figure 3a and 3b).
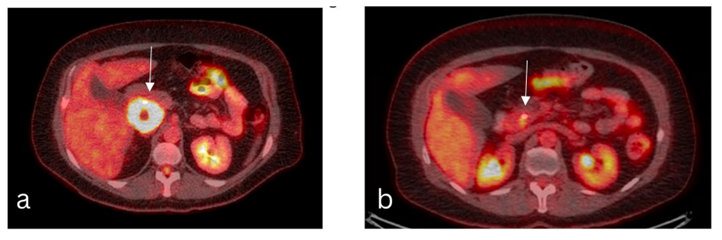
Figure 3: (a)-PET/CT simulation: 04/16/2021. Reference regions: SUVmax and mean in a reference region in the liver are 2.4 and 1.9. Pancreas: FDG avid pancreatic head mass (5.6x 5.1 cm, SUV 28.8) with central hypodensity/photopenia, possibly cystic/necrotic change or ductal dilatation. (b)-PET: 07/14/2021. Reference regions: SUVmax and mean in a reference region in the liver are 2.8 and 1.9. Pancreas: Markedly decreased size and FDG uptake of pancreatic head mass with ill-defined residual focal FDG uptake adjacent to the biliary stent, image 165, SUV 4.8, previously 5.6x5.1 cm, SUV 28.8; Images from our institutional radiology department.
Approximately 2 months later, in September 2021, another PET scan showed a completed response in the pancreatic head mass and regional lymph nodes: no definite evidence of FGD-avid neoplastic disease was seen; a decrease in the intensity of now ill-defined residual FGD uptake within the pancreatic head was noted, possibly post treatment inflammation.
Several follow up PET scans (every 3-4 months, last one in March 2024) and one CT chest-abdomen-pelvis in May 2022 were done showing sustained complete response in the pancreas and no new suspicious lesions (figure 4). In particular, no new lesions were visible on 3/20/2024, as the PET scan showed a persistent complete remission (figure 5). No acute, subacute or long-term side effects of radiation were reported by the patient.
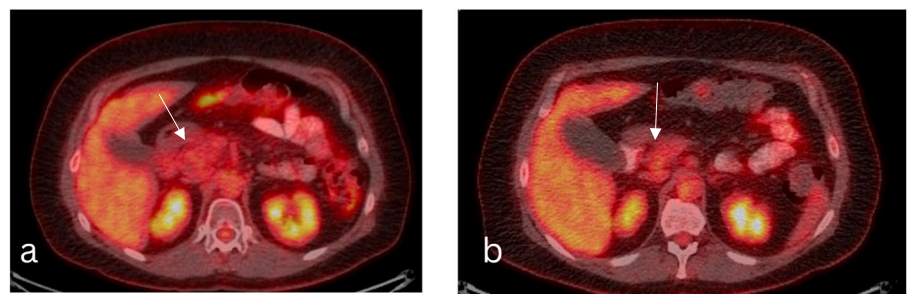
Figure 4: (a)-PET: 09/24/21. Reference regions: SUVmax and mean in a reference region in the liver are 3.3 and 2.4. Pancreas: Decreased intensity of now ill-defined residual FDG uptake within the pancreatic head, image 147, SUV 2.6, before SUV 4.8. (b)-PET: 03/16/2023. Reference regions: SUVmax and mean in a reference region in the liver are 2.9 and 2.5, prior 2.8 and 2.4. Pancreas: Unchanged mild patchy uptake in the pancreatic head at site of prior FDG avid lesion, image 153, SUV 2.4 previously SUV 2.6; Images from our institutional radiology department.

Figure 5: PET: 3/20/2024. Reference regions: SUVmax and mean in a reference region in the liver are 3.0 and 2.4. Pancreas: No abnormal uptake. No recurrent FDG avidity in the pancreatic head as was seen on PET April 16, 2021; Images from our institutional radiology department.
Pancreatic cancers are prevalent and associated with high mortality rates in the United States, accounting for one fourth of death related to cancer. Most pancreatic cancers are adenocarcinomas, thus making physicians less aware of the other types of pancreatic cancers[13]. Primary pancreatic lymphoma (PPL) is one of the rarest types of lymphoma resulting in only 1% of all extra nodal types of lymphoma and accounting for less than 0.7% of all types of pancreatic malignancies [14].
Since PPL is very rare and its clinical and imaging presentation can mimic pancreatic adenocarcinoma, physicians face a diagnostic and therapeutic challenge. Thus, a preoperative cytohistologic diagnosis is very important in case of PPL, to avoid unnecessary and morbid surgical interventions, such as a Whipple procedure or a distal pancreatectomy [7,13].
Sadot et al. from Memorial Sloan Kettering Cancer Center looked at the clinical features and outcome of PPL. A comparison between response rates of different modalities of treatment, including chemotherapy, chemotherapy with surgery, chemotherapy with radiation and surgery alone showed that the response rates of patients treated with chemotherapy only had the best clinical outcomes, with 85% CR/PR and 15% SD/PD, analogous to the response rates of patients diagnosed with nodal DLBCL and treated with either R-CHOP or CHOP. Of note, in the chemotherapy alone subgroup, 36% of patients were treated with R-CHOP and 10% with CHOP [7]. In summary, the most common type of PPL is DLBCL, and the best treatment modality is chemotherapy with R-CHOP or CHOP.
In the case of refractory or relapsed DLBCL, patients who are transplant eligible are treated by intensive salvage regimens, using high-dose chemotherapy and autologous stem cell transplant (ASCT) which only cures a restricted number of patients [15].
The PARMA trial, in which patients with chemo-sensitive refractory or relapsed non-Hodgkin lymphoma were randomized to either receive high dose chemotherapy followed by autologous bone marrow transplant (HD-ABMT) or conventional chemotherapy, showed that patients who received HD-ABMT had a greater OS (53% vs 32%) and a greater 5-year event survival (46% vs 12%) [16]. However, it was estimated that only half of the patients with relapsed/refractory (R/R) NHL would be qualified for transplant and half of those would have chemo-sensitive disease. In addition, in this trial, radiotherapy was used as part of the treatment for bulky disease that is >5cm, and the results revealed fewer instances of relapse noted when radiotherapy was used: relapses occurred at the primary site of disease at the time of the first relapse in 5 of the 12 patients who underwent irradiation and in 26 of the 42 who did not (p= 0.21).
On the other hand, transplant ineligible patients have been treated with palliative intent [15]. RT has long been considered for palliative care only in this setting. However, in some cases where the patient is transplant ineligible, or does not want transplant, radiation therapy can be administered either as effective palliation or with curative intent, as long as the tumor is localized.
In a review on the role of radiation therapy in patients with relapsed/refractory (R/R) DLBCL published in 2018, some case scenarios have been discussed by the International Lymphoma Radiation Oncology Group (ILROG), and one recommendation was that only on very rare occasions, in patients who have localized R/R disease, can radiation therapy be offered with curative intent, for example in locoregionally confined disease, with a proposed dose of 45-55Gy in 1.8Gy/fraction, reduction of treatment volume (or cone down) after 36Gy, and adjustment of final dose depending on the patient’s response [17].
Prior to the rituximab era, two randomized clinical trials, the Southwest Oncology Group Study (SWOG) 8736 and the Eastern Cooperative Oncology Group Study (ECOG) 1484, compared chemotherapy alone (CHOP) vs chemotherapy with radiotherapy in patients with non-Hodgkin’s Lymphoma [18,19]. The SWOG 8736 study concluded that 3 cycles of chemotherapy followed by involved-field radiotherapy are better than 8 cycles of chemotherapy alone when treating localized intermediate and high-grade non-Hodgkin’s Lymphoma in terms of overall survival (p=0.02) and progression-free survival (p=0.03) [18]. On the other hand, in the ECOG 1484 study, which compared observation vs low dose radiotherapy for patients who achieved complete remission after chemotherapy, no survival benefits were reported between the two groups, but in those who received radiotherapy, a prolonged 6-year disease-free survival (73% for RT group vs 56% for observation group) (p=0.05) and better local control were seen [19].
In the Groupe d’Etudes des Lymphomes d’Adulte (GELA) LNH 93-4 trial, the addition of radiation therapy to 4 cycles of R-CHOP was evaluated in patients with aggressive and localized Non-Hodgkin Lymphoma (ALNHL). The progression free survival was 61% in the R-CHOP arm, compared to 64% in the R-CHOP + RT arm (p=0.56), and the overall survival was 72% vs 68%, respectively (p=0.54) [20].
Additionally, in a prospective, randomized controlled phase 3 trial published in 2011, six hundred and forty patients with aggressive types of non-Hodgkin lymphoma primarily DLBCL as an integral part of combined-modality therapy were randomly assigned to receive radiation doses either of 40-45gy in 20-23 fractions or 30Gy in 15 fractions. The overall response rate was 91% in both groups (p=0.87). No significant difference was detected between the 2 groups in the rate of within-radiation field progression (HR=0.98, 95%CI=0.68-1.4, p=0.89), progression free survival or overall survival. Notably, a trend toward reduced toxicities was detected in the lower dose group, with only the decrease in erythema reaching statistical significance [21].
This case report contributes to the ongoing growing body of literature on the efficacy of radiation therapy in chemo-refractory, localized DLBCL cases.
In our patient, DLBCL did not respond to 6 cycles of R-CHOP chemotherapy, but achieved PET complete response to a definitive dose of radiation therapy without noticeable side effects. This paradigm offers valuable insights into improving the therapeutic index in patients with localized extranodal DLBCL using definitive radiation therapy, while avoiding more cytotoxic regimens with or without stem cell transplantation.
The presented case study has limitations that should be acknowledged. As a single case report, the findings may not be generalized to a broader patient population due to patient and disease variability. The decision to proceed to definitive radiation therapy in patients with chemo-refractory DLBCL needs to be personalized and agreed upon at multidisciplinary meetings by the tumor board.
We presented a case of a localized DLBCL of the pancreas that was refractory to 6 cycles of R- CHOP. The tumor board decision was to defer stem cell transplant and proceed with definitive radiation therapy. A total dose of 36/50 Gy in 25fx was delivered to the patient. No acute, subacute or long-term side effects of radiation were reported by the patient or the treating physician. The patient remains with no evidence of disease almost 3 years since the completion of radiation therapy. In selected cases, definitive radiation therapy in chemo-refractory localized DLBCL is a reasonable alternative to aggressive systemic therapies and/or stem cell transplant.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
