
case report | DOI: https://doi.org/10.31579/2692-9392/129
1Professor and Head/Senior Consultant Physician, Department of Medicine/ Department of Nephrology, Defence Services Medical Academy/ No. (1) Defence Services General Hospital (1000-Bedded)
2Consultant Physician, No. (1) Defence Services General Hospital (1000-Bedded)
3Consultant Radiologist, No. (1) Defence Services General Hospital (1000-Bedded)
4Consultant Hematologist, No. (1) Defence Services General Hospital (1000-Bedded)
5Consultant Pulmonologist, No. (1) Defence Services General Hospital (1000-Bedded)
6Pulmonology Fellow, No. (1) Defence Services General Hospital (1000-Bedded)
7Assistant Lecturer / Consultant physician, Defence Services Medical Academy
8Physician, No. (1) Defence Services General Hospital (1000-Bedded)
*Corresponding Author: Khin Phyu Pyar, Professor and Head/ Senior Consultant Physician, Department of Medicine/ Department of Nephrology, Defence Services Medical Academy/ No. (1) Defence Services General Hospital (1000-Bedded), Myanmar
Citation: Khin Phyu Pyar, Sai Aik Hla, Soe Min Aung, Soe Win Hlaing, Zar Ni Htet Aung. et all (2022). A 32-Year-Old Dental Surgeon Presented with Massive Hemoptysis, Fever and Hypotension As A Result of Bleeding from Bronchiectasis due to Pulmonary Tuberculosis (New Case) with Concurrent Covid-19 Infection Successfully Treated with Anti-Tubercular Therapy (Isoniazid, Rifampicin, Ethambutol and Pyrazinamide): A Case Report on two Epidemic Disease. J. Archives of Medical Case Reports and Case Study, 6(2); D
Copyright: © 2022 Khin Phyu Pyar, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 May 2022 | Accepted: 30 June 2022 | Published: 08 July 2022
Keywords: hemoptysis; COVID-19; tuberculosis; bronchiectasis
A dental surgeon had sudden onset of massive hemoptysis with hypovolemic shock during COVID-19 epidemic; her nasopharyngeal swab for SARS-CoV-2 PCR was positive. She noticed 2 days history of fever and cough; however, she had poor appetite for nearly two weeks. Resuscitation was done successfully with fluids and blood transfusion. Chest radiograph showed opacities in left lower zone; and, NECT chest revealed consolidation in left lower lobe and patchy opacities in right upper lobe with areas of bronchiectasis. Sputum for gene expert for drug resistant tuberculosis, Ziehl Neelsen stain for acid fast bacilli and Lowenstein Jensen media for culture could not be done as microbiological services were limitted in the peak of COVID-19 pandemics. Therefore, anti-tubercular therapy (isoniazid, rifampicin, ethambutol and pyrazinamide) was initiated mainly based on NECT chest without sputum confirmation; the patient made dramatic improvement. Two months later, she gained 10 lbs weight; and radiological improvement.
Covid-19 pandemic has had devastating effect on tuberculosis care; therefore, tuberculosis epidemic has been worsening (Pai et al., 2022). According to the World Health Organization’s 2021 Global TB report, the COVID-19 pandemic has reversed years of global progress in tackling tuberculosis and for the first time in over a decade, TB deaths have increased (World Health Organization, 2021). Here was a noticeable drop in tuberculosis case detection during the COVID-19 pandemic (Bardhan et al., 2021).
One report from meta-analysis revealed that people with tuberculosis are not more likely to get COVID‐19, but pre‐existing tuberculosis has a higher chance of developing serious complications from COVID‐19 (Gao et al., 2021). Regarding the treatment, the potential role of drugs prescribed during the initial phase to treat COVID-19 and their interaction with anti-TB drugs require caution (Visca et al., 2021). In countries where risk factors for mortality are highly prevalent among young individuals (smoking, alcohol and substance abuse, HIV co-infection, among others), particularly in the presence of drug resistance and difficult access to diagnosis (delayed diagnosis), the impact of mortality may be higher. We agree that, in resource-limited settings, poverty and malnutrition might play an important role in increasing morbidity and mortality (Tadolini et al., 2020). TB should be considered a risk factor for severe COVID disease and patients with TB should be prioritised for COVID-19 preventative efforts, including vaccination (The TB/COVID-19 Global Study Group, 2021). The study from China suggested that a moderate level of evidence suggests that COVID-TB patients are more likely to suffer severe disease or death than COVID-19 patients. Finally, routine screening for TB may be recommended among suspected or confirmed cases of COVID-19 in countries with high TB burden . Due to the ongoing pandemic, healthcare workers have been diverted to activities implemented for effective COVID-19 management, leaving a meager workforce to help deal with TB management (Song et al., 2019).
During COVID-19 pandemic, all patients with respiratory symptoms were presumed as COVID-19 infection; however, hemoptysis was relatively rare. The causes of hemoptysis in patients with COVID-19 infection are pulmonary embolism and infarction, secondary bacterial pneumonia, DIC and pulmonary oedema.
In pulmonary embolism and infarction, the sputum color is prune juice; and it is associated with chest pain which is pleuritic in nature. Pleural rub may be audible on auscultation. Chest radiograph may be normal. CT pulmonary angiogram is gold standard investigation; nevertheless, it is not easy to do in poor resource settings. High D dimer level is a good clue for diagnosis.
If the COVID-19 patient has secondary bacterial pneumonia, his sputum is mainly purulent which may be mix with blood. Patient may have neutrophil leucocytosis. Sputum for gram stain and culture may reveal organism though most of the microbiological lab are afraid of COVID-19 infection.
If hemoptysis is due to DIC, the patient may show other evidence of DIC like petechiae in skin and mucosal bleeding: epistaxis, gastrointestinal bleeding, hematuria etc. Blood tests may show anaemia, low platelet count, prolong prothrombin time and prolong APTT. The patient may have severe features of COVID-19 pneumonia like ARDS, low SaO2, hypotension and very high inflammatory markers such as CRP, ferritin, LDH, and liver enzymes.
Pulmonary oedema in patient with COVID-19 infection is poor sign; it results from acute coronary syndrome, myocarditis, acute renal injury and fluid overload. The sputum is typically pink frothy; patient is in severe dyspnoea. Physical examination reveals tachycardia, cyanosis, triple rhythm and fine basal crackles. Chest radiograph reveals upper lobe dilatation with hilar haziness; it is contrary to typical changes in COVID-19 pneumonia- mainly lower zone peripheral shadows. Blood for pro-BNP may be high.
A 32-year-old woman, a dental surgeon, had low grade fever and dry cough for 2 days. Then she noticed reddish blood in her sputum following some tickling sensation in throat in one evening. She continued to cough with increasing amount of fresh blood, 1,000 cc over an hour. Then, she felt giddy and also fainted. Her friends brought her to hospital at 02:00 hour. At emergency department, her blood pressure was 50/30 mmHg; pulse was thready 160/minutes. Extremities were cold and clammy. Resuscitation with saline and blood transfusion. Blood pressure became 100/60 mmHg, pulse rate 110/minutes after replacing 3.0 liters with saline and blood transfusion two units.
Blood for complete picture reveals as follows; hemoglobin 12.3 gm%, total WBC count 4.84 x 109 /L and platelet 164 x 109 /L. Absolute Neutrophils count was normal 4.19 x 109 /L; absolute Lymphocyte count was low 0.5 x 109 /L. CRP was high 18.25 mg/L (less than 5 mg/L). Liver enzymes were normal; AST and ALT were 17 IU/L and 21 IU/L respectively. Alkaline phosphatase was normal 63 IU/L. Serum creatinine was normal (0.7 mg%); electrolytes too (Na 137 mmol/L, K 3.7 mmol/L, Cl 99 mmol/L). Random blood sugar was normal. Retroviral serology was negative. Her nasopharyngeal swab for SARS-CoV-2 PCR was positive. She denied history of pulmonary tuberculosis; however, she had poor appetite for nearly two weeks.
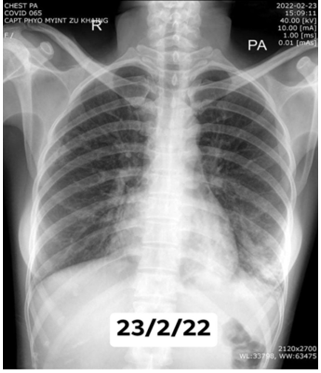
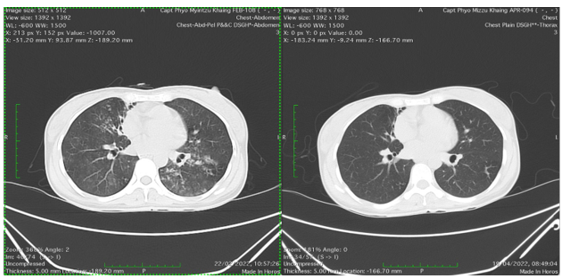
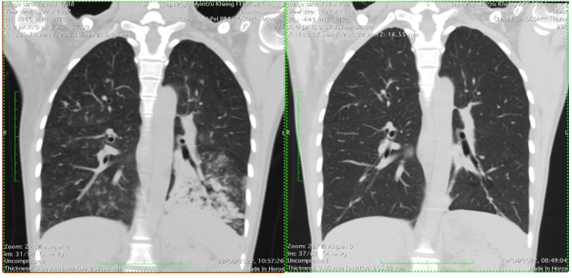
Chest radiograph showed mild patchy opacities in left upper zone and upper zones were clear. (Figure 1) NECT chest revealed consolidation in left lower lobe and patchy opacities in right upper lobe with bronchiectasis. (Figure 2, 3, 4, 5).


They were highly suggestive of tuberculosis. Sputum culture, Ziehl Neelsen stain for acid fast bacilli and Lowenstein Jensen media culture for acid fast bacilli, Gene expert tests for drug resistant tuberculosis were out of service in the peak of COVID-19 pandemics. Thus, empirical anti-tubercular therapy (isoniazid, rifampicin, ethambutol and pyrazinamide) was initiated without microbiological confirmation. Hemoptysis subsided gradually. Two months after anti-tubercular therapy, the patient gained 10 lb weight. Chest radiograph was almost normal. NECT showed marked improvement.
During COVID-19 pandemic, all patients with respiratory symptoms were presumed as COVID-19 infection; however, hemoptysis was relatively rare. The causes of hemoptysis in patients with COVID-19 infection are pulmonary embolism and infarction, secondary bacterial pneumonia, DIC and pulmonary oedema; they have peculiar clinical features.
In pulmonary embolism and infarction, the sputum color is prune juice; and it is associated with chest pain which is pleuritic in nature. Pleural rub may be audible on auscultation. Chest radiograph may be normal. CT pulmonary angiogram is gold standard investigation; nevertheless, it is not easy to do in poor resource settings. High D dimer level is a good clue for diagnosis.
If the COVID-19 patient has secondary bacterial pneumonia, sputum is mainly purulent which may be mix with blood. Patient may have neutrophil leucocytosis in full blood count. Sputum for gram stain and culture may reveal organism though most of the technicians from microbiological lab are afraid of COVID-19 infection.
If hemoptysis is due to DIC, the patient may show other evidence of DIC like petechiae in skin and mucosal bleeding: epistaxis, gastrointestinal bleeding, hematuria etc. Blood tests may show anaemia, low platelet count, prolong prothrombin time and prolong APTT. The patient may have severe features of COVID-19 pneumonia like ARDS, low SaO2, hypotension and very high inflammatory markers such as CRP, ferritin, LDH, and liver enzymes.
Pulmonary oedema in patient with COVID-19 infection is poor sign; it results from acute coronary syndrome, myocarditis, acute renal injury and fluid overload. The sputum is typically pink frothy; patient is in severe dyspnoea. Physical examination reveals tachycardia, cyanosis, triple rhythm and fine basal crackles. Chest radiograph reveals upper lobe dilatation with hilar haziness; it is contrary to typical changes in COVID-19 pneumonia- mainly lower zone peripheral shadows. Blood for pro-BNP may be high.
Common causes of massive hemoptysis are bronchiectasis, lung abscess, pulmonary aspergilloma; all cab be visualized in NECT chest.
During COVID-19 pandemic, National Health System mainly focuses on COVID-19 infection: awareness for early diagnosis, isolation and treatment at COVID-19 designated hospital. The aim is to give appropriate treatment to patients with COVID-19 infection. In addition, protection of health care personnel is uttermost important. Moreover, prevention of non-COVID inpatient cases from acquiring COVID-19 infection is also essential. Therefore, other common infectious diseases like tuberculosis were not in the first list; this case highlighted the importance of awareness of pulmonary tuberculosis in COVID-19 pandemic. We are facing the battle against the two epidemic diseases COVID-19 infection (new one) and pulmonary tuberculosis (old one); the main reason for presenting this case.
The clinical presentation of concurrent tuberculosis and COVID-19 infection made the differential diagnosis difficult. The patient had fever and cough for 2 days only; it pointed acute infection rather than chronic one. However, the patient had appetite loss for 2 weeks; the clue for tuberculosis. Moreover, the occupation being a dental surgeon was a high risk for pulmonary tuberculosis.
Diagnosing tuberculosis during the COVID-19 pandemic requires a high index of clinical suspicion because the two diseases have similar characteristics, such as fever and respiratory symptoms.In full blood count, the patient had significant lymphopenia; the possibilities were both severe COVID-19 infection and tuberculosis.
In chest Xray, there was patchy opacities in left lower zone; the likely aetiology was COVID-19 infection. It was against pulmonary tuberculosis; the common site was upper zone.
Nonetheless, NECT chest gave the final decision. The presence of multiple bronchiectasis indicated the possible source for massive hemoptysis. And having multiple patchy opacities in right upper lobe explained the most likely aetiology- tuberculosis. In addition, areas of consolidation in the left lower zone in the presence of apical lesion on right side supported the most likely aetiology- tuberculosis. In countries with a high tuberculosis burden, the possibility of a concomitant diagnosis of tuberculosis and COVID-19 should always be considered in order to ensure the appropriate management of both diseases.
Another learning point was that NECT chest was mandatory if the chest Xray was normal in patients with hemoptysis. It is important information in poor resource setting. Furthermore, the presence of multiple bronchiectasis indicated the possible source for massive hemoptysis as well as the chronicity of disease- tuberculosis; the patient had tuberculosis for several months though the history of appetite loss was only two weeks. Thus, it pointed out the importance of awareness of asymptomatic tuberculous infection in developing countries.
In the era of drug resistant tuberculosis (multi-drug resistant or extended drug resistant), doing sputum for gene expert test is essential. If possible, sputum culture for drug resistant tuberculosis should be done in all cases. COVID-19 pandemic has had a significant impact on the diagnosis and treatment of tuberculosis. This patient, being health care worker, was a likely case of drug resistant tuberculosis. Because of logistic problem, we did not have microbiological evidence. Nevertheless, the patient had both clinical and NECT chest improvement after two months of anti-tubercular therapy. It highlighted the importance of clinical and radiological acumen of treating physician.
Having multiple bronchiectasis near right cardiac border was commonly due to atypical mycobacterium tuberculosis which required different drug regimen as a treatment (Lee et al., 2013). The major cavities in NTM disease generally have thinner and more even walls than those in TB. According to Kim et al. (2017), “when cavities are associated with adjacent pleural thickening, ill-defined satellite tree-in-bud nodules, or fewer non-cavitary nodules ≥ 10 mm, these CT findings are highly suggestive of NTM disease rather than TB” (Kim et al., 2017). This patient had ill-defined satellite tree-in-bud nodules; however, having clinical and radiological improvement was against atypical tuberculosis; another reason for reporting case.
The combination of tuberculosis and COVID-19 has great potential for morbidity and mortality. Patients with tuberculosis and COVID-19 may be at a greater risk of poor outcomes and death than are those with COVID-19 alone (Dave et al., 2021). One study showed that the risk of death was 2.17 times higher in patients with tuberculosis and COVID-19 than in those with COVID-19 only (Sy et al., 2020). Therefore, early detection of the combination is important for the proper management of both diseases. In this patient, we detect the diagnosis early; moreover, the response to anti-tubercular therapy was very dramatic.
Prioritization of treatment in patients with tuberculosis and concomitant COVID-19 infection is not easy. If the patient had severe COVID-19 infection, anti-viral therapy and anti-inflammatory drugs (steroids) would be first choice; the untoward effects would be exacerbation of tuberculosis. On the other hand, If the patient had mild COVID-19 infection, he did not require anti-viral therapy and anti-inflammatory drugs (steroids); he might need symptomatic drugs like anti-pyretics. In this patient, COVID-19 infection was mild as evidenced by minimal chest radiographic changes with mildly raised CRP with normal liver enzymes; thus, anti-tubercular drugs became first treatment of choice.
Common things are always common even in COVID-19 pandemics. Awareness of pulmonary tuberculosis is important in patient with hemoptysis. A high index of clinical suspicion is essential as two diseases- pulmonary tuberculosis and COVID-19 infection have similar characteristics, such as fever, respiratory symptoms and lymphopenia. Good clinical acumen is necessary for treatment. NECT chest is mandatory inpatients with hemoptysis.
Acknowledgements
The authors would like to thank the patient for giving consent to this article. Also, to all doctors and nursing team for making great efforts in caring him. The authors acknowledged the following team; Professor Ohmar Hlaing and team for radiology support, Professor Myint Zaw, Professor Kyaw Zay Ya and Professor Ko Ko Lwin for administrative support.
Declaration of conflict of interest
The authors declared no potential conflicts of interests with respect to authorship and publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting cases.
Funding
The authors received no financial support for publication of this article.
Informed consent
The informed consent for publication in this article was obtained from husband of patient.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
