
Review Article | DOI: https://doi.org/10.31579/2690-1897/176
1 Department of Surgery, Royal Darwin Hospital, Darwin, Australia.
2 School of Medicine, Flinders’ University.
*Corresponding Author: David Fernando Toro Tole, Department of Surgery, Royal Darwin Hospital, Darwin, Australia.
Citation: Toro Tole DF, Joe Hedger, Rachel Yun, Amelie Maurel, (2024), A 20 Year Case Series of Anorectal Foreign Body Trauma in the Northern Territory of Australia, J, Surgical Case Reports and Images, 7(1); DOI:10.31579/2690-1897/176
Copyright: © 2024, David Fernando Toro Tole. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 February 2024 | Accepted: 19 February 2024 | Published: 28 February 2024
Keywords: anorectal trauma; general surgery; foreign body; surgery; rural and remote health
Backgrounds: Anorectal foreign body insertion is a practice reported as far back as the 16th century but practiced earlier. The incidence of associated anorectal trauma, particularly with a male predominance, has been increasing. The risk of delayed presentation in rural settings can impact surgical outcomes.
Methods: This is a case series of retained anorectal foreign body and resulting trauma in a tertiary hospital of the Northern Territory between 2003 and 2023. Data including demographics, foreign body, clinical presentation, surgical intervention, and complications were recorded.
Results: A total of 44 patients were identified. Majority of patients were male with a mean age of 37. and 14 patients living rural or remote. The primary method for management was transanal manual extraction (33 cases), sigmoidoscopy (11 cases) and laparotomy (3 cases). The main complications observed were perforation (3 cases), and Fournier’s Gangrene post anal sphincter repair. Delays in seeking medical attention were associated with increased rurality and further surgical implications.
Conclusion: The outcome of this study will be useful for health professionals to understand the potential challenges and complications associated with foreign body anorectal trauma in a rural setting with a delayed presentation time.
Anorectal trauma secondary to foreign body insertion is becoming more common, but precise epidemiological data are often lacking due to underreporting [1-2]. A higher incidence has been noted amongst males with a mean age of 48 years [3-5]. Retained foreign bodies, are usually those used for sexual and erotic stimulation, but also therapeutic purposes or assault [6]. A range of foreign bodies, including but not limited to light bulbs, bottles, sex toys, vegetables/fruits and screw drivers has been reported in anorectal trauma [1-6]. Early diagnosis and management is important given the risk of severe injury like perforation which can result in peritonism [1-6].
Delay in seeking medical attention is not uncommon due to personal and socio-cultural barriers [6]. Rurality can be a factor due to the increased travel time to access tertiary services. Reluctance to disclosure due to embarrassment can delay timely diagnosis and management. Management options include manual transanal extraction [1-7], showing a success rate ranging from 60% to 75% [1-8]. Unsuccessful bedside extraction should be re-approached with pudendal nerve block, spinal anaesthesia, sedation, or general anaesthesia. Unstable patients or those peritonitic, may warrant an exploratory laparoscopy or laparotomy [1-7].
Along with the rising trend in retained rectal foreign bodies, the presence of retained foreign bodies and anorectal trauma has been associated with increased healthcare expenditure, wasted theatre time, lost work days and overall warrants further investigation [1-9]. There is need for a growing body of evidence on the epidemiology and management of anorectal trauma and retained foreign bodies, as well as a better understanding of complications. This is particularly important in rural, remote, and very remote areas, where awareness of this can assist with decision-making to transfer or escalate care.
The aim of the investigation is to further describe the incidence and complications of anorectal trauma by foreign body insertion, and the treatments associated particularly in a rural/remote setting of Australia. This description can then be applied to further rural and remote regions of the world, and help to make more informed clinical decisions.
This is a retrospective case series identifying anorectal trauma at a single tertiary centre of the Northern Territory of Australia. The investigation started by collecting all Royal Darwin Hospital admissions coded for anorectal trauma from June 1st 2003 to June 1st 2023 to describe a 20 year picture. Patients included in the study were those who presented with a complaint of or a foreign body in their anus, rectum, or sigmoid colon to Royal Darwin Hospital. Patients were excluded if their anorectal trauma was due to mechanism other than foreign body insertion. Cases were identified using ICD codes, and data extracted from hospital records included demographics, relevant medical history, clinical presentation, motive for insertion, attempt at self-removal, investigations, surgical intervention, and outcome. This data was then processed into Microsoft Excel, which was used to conduct further statistical analysis.
Analysis was conducted using Microsoft Excel (Redmond USA).
Sociodemographic Characteristics
Over the 20-year period, 44 patients presented with foreign body anorectal trauma. Most patients were male (84%) with age distribution of 10 to 75 years and mean age of 37 years (Table 1). The highest incidence was among patients 36 to 45 years (27%). Patients presenting to the Emergency Department predominantly reported a lost foreign body as their primary concern (66%). Four patients were under the influence of alcohol, two cases in patients known to have schizophrenia, one case associated with child behavioural problems and one case in a patient with a traumatic brain injury.
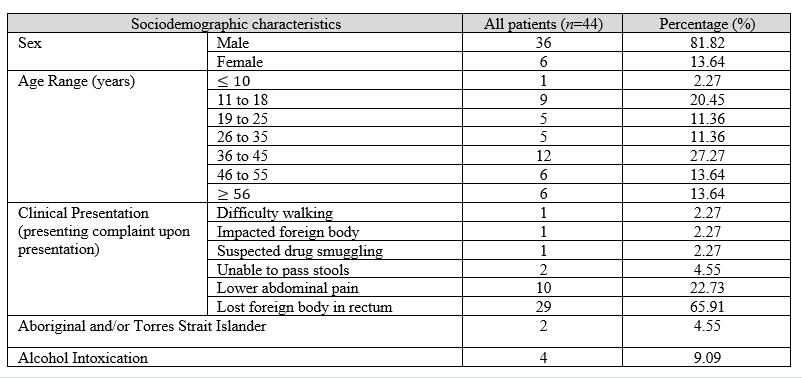
Table 1. Sociodemographic characteristics of patients presenting with foreign body anorectal trauma
The most common motive was sexual pleasure (89%), whilst others were self-management of constipation, accidental, and drug smuggling. The type of foreign body objects found exhibited significant variability. Most of the objects were sex toys (36%), inorganic household items including bottles (27%), organic household items (14%), and 1 case of the tip of an enema syringe (2%). Unfortunately, due to damage to item and patient not wanting to disclose, 6 patients had “Unknown” foreign bodies causing trauma, representing 14% of total patients (Table 2). The most common presenting complaint was an earnest admission of losing a foreign body in rectum (66%), followed by lower abdominal pain (23%) with the least common presentations being suspected drug smuggling, impacted foreign body, and difficulty walking (2
This case series study holds significance as it marks the first of its kind in the Northern Territory, a predominantly rural location. In the cases observed over 20 years, most patients were male identifying, with a mean age of 37 years, aligning with the consistent pattern observed elsewhere [4,10,11]. The average age of this cohort (37 years) is a decade younger than what is reported in other studies (48 years) [3-5]. This left skewed age distribution may be attributed to a higher prevalence in younger individuals in the Northern Territory population, which according to the Australian Bureau of Statistics (2016) has a median age of 32 [12]. A prominent feature was 30% of patients living rural or remote. Out of the six patients who presented with a perforation, four of them were rural, with a delayed presentation time greater than 24 hours. This has been observed in other studies with a rural focus [11].
The variety of foreign body objects was consistent with the diversity reported in the literature. Sex toys were the most commonly inserted items. As anticipated among most cases, the predominant motive behind foreign body insertion was for sexual gratification accounting for 87% of cases. A growing societal acceptance of anal pleasure has likely contributed to males being more willing to enjoy anal pleasure with a sex toy regardless of sexuality [13,14]. Despite the increasing recognition, patients are still reluctant to disclose foreign body use. This is supported by the data on delay to presentation after 12 hours, attempt at self-removal prior to presentation and higher likelihood of presentation overnight (34% of cases). We identified other motives for foreign body use including enema use for constipation and drug smuggling. However, the use of foreign bodies has been reported elsewhere as a consequence of rape or sexual assault [15]. Hence, health care professionals should be mindful of the motive, and maintain a high level of suspicion in cases with an incongruent history.
In the Northern Territory, most cases were managed by transanal extraction under general anaesthesia in theatre. This assists in reducing sphincter spasm as it induces relaxation allowing for improved chances of transanal retrieval and shorter operating time [1]. Only 10 cases required further procedures including colostomy and perforation repair, including the need for a conversion to a laparotomy. It appears the potential extent of injury is unbeknownst to the public [16]. Awareness and public education, including the appropriate and careful use of foreign bodies will assist in reducing the likelihood of these traumatic injuries occurring.
To our knowledge, there are no existing similar studies published in the Northern Territory. While this study represents the very first of its kind in the region, it is crucial to recognise the limitations of establishing significant correlations within this dataset due to there being a limited number of cases. Hence, the findings of the study should be approached with careful consideration. This leads to our recommendation of a review of the data in decades to come to help facilitate a larger sample size of cases and results, describing a more robust picture of anorectal trauma. The major limitation of small sample size in this study leaves what is a small picture that can be used in a clinical setting, and hopefully with further research this can be rectified.
In conclusion, this study serves to provide the epidemiological information and surgical implication on patients presenting to Northern Territory hospitals with anorectal trauma due to foreign bodies. Whilst there is an increasing acceptance for self-pleasure and increasing incidence of foreign body insertion, many patients remain hesitant to seek professional help. More severe surgical implications were associated with the delay in presentation of time. Our recommendation for bettering care of anorectal trauma is to encourage a healthy and safe clinical environment to help prevent stigma and facilitate earlier presentation to care from patients. Once a patient does present, our data shows that transanal extraction under general anaesthesia represents a very capable method of removing foreign bodies without exacerbating trauma. There is still evidence to suggest that there is a need for more awareness within health care professionals to ensure that patient-centred care is delivered, and with further research conducted with a larger sample size more distinct treatment for specific episodes can be elaborated on.
Ethics approval and consent to participate.
This is a case report that does not require a formal ethical committee approval in the Northern Territory of Australia.
Data is within the tertiary care centre Royal Darwin Hospital and requires a request of access to the centre.
The authors declare that they have no competing interests.
Funding statement.
This research was not funded.
Author contributions.
DTT – writing – original draft; investigation
JH – writing – original draft; investigation
RY – writing – original draft; investigation
AM - writing - review and editing; supervision
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
