
Editorial Note | DOI: https://doi.org/10.31579/2637-8892/033
Erasmus Medical Centre, Radiology and Nuclear Medicine, Optical Molecular Imaging, Netherlands.
*Corresponding Author: Vincent van Ginneken, Erasmus Medical Centre, Radiology and Nuclear Medicine, Optical Molecular Imaging, Netherlands
Citation: Vincent van Ginneken & Clemens Löwik (2018) Extension of the “Fetal Origin Hypothesis of Barker” towards the “Fetal Origin Hypothesis of Mental Diseases”,J Psychology and Mental Health Care, 2(3) DOI: 10.31579/2637-8892/033
Copyright: © Vincent van Ginneken et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 May 2018 | Accepted: 18 June 2018 | Published: 01 July 2018
Keywords: hypothesis; physiological; endocrine; cardiovascular diseases
In this editorial we will first describe most common information about the intriguing “traditional” fetal origin hypothesis of Barker for physiological, endocrine and cardiovascular diseases (CVDs). The ‘developmental origins of adult disease’ hypothesis, often called the ‘Barker hypothesis’, states that adverse influences early in development, and particularly during intrauterine life, can result in permanent changes in physiology and metabolism, which result in increased disease risk in adulthood.
In this editorial we will first describe most common information about the intriguing “traditional” fetal origin hypothesis of Barker for physiological, endocrine and cardiovascular diseases (CVDs). The ‘developmental origins of adult disease’ hypothesis, often called the ‘Barker hypothesis’, states that adverse influences early in development, and particularly during intrauterine life, can result in permanent changes in physiology and metabolism, which result in increased disease risk in adulthood. This hypothesis originally evolved from observations by Barker and colleagues that the regions in England that had the highest rates of infant mortality in the early twentieth century also had the highest rates of mortality from coronary heart disease decades later [1]. As the most commonly registered cause of infant death at the start of the twentieth century was low birthweight, these observations led to the hypothesis that low birthweight babies who survived infancy and childhood might be at increased risk of coronary heart disease later in life. In this editorial we want to extend the hypothesis that the nutritional status of the future mother determines the "quality" of the brain of the foetus and the morbidity of mental illness in later life like early dementia.
With roughly 1 billion obese people globally, 1 billion acutely hungry and 2 billion malnourished, we predict that, following our hypothesis in future generations, more mental illness will occur at earlier ages. It is our prediction it will affect the population structure from a pyramid Gauss-curve towards a kite-shaped population structure. In other words, who pays us pension?
So, there is increasing suggestion that the seeds of adult Type 2 diabetes are sown in early life and may be initiated by genetic and environmental events operating in early life. This is based on:
a). The known association between fetal growth and adult diseases [1];
b). Transmission effects at the insulin gene, together with the evidence for excess Type 2 Diabetes in the mothers of offspring also exhibiting the pathogenesis of Type 2 Diabetes;
c). The known associations between fetal growth and adult diseases.
Ad a). The theory of fetal origins or prenatal programming of later at adult age life developing diseases was based on in utero nutritional deficiencies. Dr. David Barker [1] initial observation was that low birth weight (LBW) infants had an increased risk for coronary heart disease, stroke, Type 2 diabetes, insulin resistance, increased blood pressure, hyperlipidemias, increased fibrinogens or Metabolic Syndrome. He hypothesized that Metabolic Syndrome originated through fetal adaptations to undernutrition. These adaptations alter growth trajectories or programming at the expense of tissue development and physiological processes [2]. This hypothesis was originally put forward by [1] and stated that environmental factors, particularly nutrition, act in early life to program the risks for adverse health outcomes in adult life.
Ad b). In case of genetically determined insulin resistance this could result in low fetal growth and insulin resistance later on: “Fetal Insulin Hypothesis”.
Ad c). Size relationships are particularly strong because insulin resistance is programmed in late gestation when disproportionate fetal growth is manifest. Consequently, those populations with a high prevalence of Low Birth Weight (LBW) infants are most at risk for the development of “diabesity” (Type 2 Diabetes in combination with Obesity) when they adopt Westernized diets and lifestyles [2].
This hypothesis has been supported by a worldwide series of epidemiological studies that have provided evidence for the association between the perturbation of the early nutritional environment and the major risk factors (hypertension, insulin resistance, and obesity) for cardiovascular disease, diabetes, and the metabolic syndrome in adult life.
[3 & 4] reviewed four clear examples of epidemiological studies, which supported the "Fetal Origin Hypothesis of Barker"[1]. This hypothesis stated that fetal under-nutrition in middle to late gestation, which leads to disproportionate fetal growth, programs later coronary heart disease [1] but also hypertension, and T2DM in adult life [5]. Those four clear examples reviewed by [4] were:
a). In monozygotic twin pairs who were discordant for diabetes, the diabetic twin had a significantly lower birth weight than the normo-glycemic co-twin.
b). Individuals exposed in utero to famine during the Dutch Hunger Winter have shown directly that poor maternal nutrition, especially during the last trimester of pregnancy, leads to growth restriction of the fetus and is associated with poor glucose tolerance and Insulin Resistance (IR) in 50 years-old offspring.
c). In two independent studies on South-African children and Indian children those children born with a low birth weight, but who underweight rapid childhood weight gain, had the worse glucose tolerance, Insulin Resistance (IR) and were thus proposed to be the most susceptible to the development of T2DM in adulthood.
d). Infants, "small for gestational age" (SGA) in comparison to infants "appropriate for gestational age" (AGA) demonstrated that the SGA infants had a rapid postnatal catch up growth but at an age of three years were more Insulin Resistant than AGA infants [reviewed by: 4].
Later this hypothesis was extended to "Fetal Origins of Adult Disease" hypothesis which established a relationship between an adverse intrauterine environment and offspring disease in adult life [6]. Later the "Thrifty Phenotype Hypothesis” [7] explained not solely the association between insufficient in uteru nutrition and cardiovascular diseases decades later [1] but also the later development of Type 2 Diabetes (T2DM) [6]. During development of the fetus in an adverse uterine environment due to "fetal programming" [8], the imbalance between the early and postnatal environments may then conflict with the programming that occurred during fetal life and predispose the offspring to the subsequent development of metabolic diseases in adulthood [9]. This "Thrifty Phenotype Hypothesis” states that during periods of inadequate nutrition, the fetus directs fuel for growth to the most essential organs, for example, the brain, while other organs are deprived of nutrients and are underdeveloped [10]. Intrauterine growth retardation would permanently alter the development and metabolic functions of organs, for example, the pancreas leading to cell dysfunction [11]. These alterations would be beneficial to survival in a poor nutritional environment, but nutritional abundance might lead to metabolic problems, such as Obesity susceptibility [12] and insufficiency in insulin secretory capacity and insulin resistance (IR) [10].
As a consequence, in the offspring Metabolic Syndrome (Obesity, hypertension, T2DM) will develop as a result of in utero environmental alterations [8,10] and implicate enhanced appetite, and adipogenesis as contributory factors (reviewed: 8 & 12]. The subsequent offspring Obesity in association with an increased appetite is described to the effect of "fetal programming" on leptin concentration, a satiety hormone [8,13] but as other hypothalamic neuropeptide appetite regulating factors like neuropeptide Y (NPY) and agouti-related protein (AgRP) [14]. The ability of these environmental factors on the fetus to promote a phenotype or disease state mentioned above (e.g. insulin resistance (IR), glucose intolerance, T2DM, Obesity, hypertension, coronary artery diseases and mental disorders like schizophrenia), not only in the individual exposed but also in subsequent progeny for successive generations is termed transgenerational inheritance [15]. These epidemiological studies support the "Fetal origins Hypothesis" followed by the "Thrifty Phenotype Hypothesis”. These state that fetal under-nutrition in middle or late gestation is programmed to exhibit a "thrifty phenotype" resulting in offspring with Metabolic Syndrome (obesity, hypertension, T2DM) as a result of in utero environmental alterations and implicate enhanced appetite and adipogenesis as contributory factors. It is suggested via epigenetic inheritance systems starvation of the parents
and obesity results in Type 2 diabetes [16].

Figure 1: 'Fetal' or 'early' origins of adult disease hypothesis. (Source: [1] Barker (1995)).
A study of Valdez turned out that reduced fetal growth and a low birth weight have been associated with an increased risk of cardiovascular disease, Type-2 diabetes and features of the metabolic syndrome developing later on [17]. In another study it turned out that children with a low birth weight showed significant more hyper-insulinemia and insulin resistance compared to controls with normal birth weight [18]. A probable explanation could be the ‘thrifty phenotype’ theory [7]. The theory suggests that low birth weight, due to intra-uterine undernutrition, might have the consequence of developmental adaptations in certain tissues (for example endocrine pancreas, adipose tissue and muscle fiber) predisposing individuals to cardiovascular and metabolic disturbances in adult life.
Not only low birth weight can induce insulin resistance, but also the other way in case of genetically determined insulin resistance. This means that genetically determined insulin resistance could result in low fetal growth and insulin resistance later on. This principle is known as the “Fetal Insulin Hypothesis” [19].
Several studies have been performed on the effects of maternal intrauterine undernutrition on offspring birth weights in a cohort of women born between August 1944 and April 1946 in Amsterdam, The Netherlands. This period included "the Dutch Hunger Winter", a war-induced famine. Undernutrition was defined separately for each trimester of pregnancy as an average supply of less than 1,000 calories per day from government food rations [20].
Maternal birth weight itself was decreased after third trimester intrauterine exposure but not after first trimester exposure. The authors suggest that there may be long-term biological effects, even into the next generation, of maternal intrauterine undernutrition which do not correspond to the effects on the mothers' own birth weights [20]. This was later confirmed in studies on impaired insulin secretion by comparing the glucose tolerance in people who had been prenatally exposed to famine compared with people unexposed to famine [21,22] stated in their review that exposure to famine during gestation resulted in increases in impaired glucose tolerance, obesity, coronary heart diseases, atherogenic lipid profile, hypertension, microalbuminuria, schizophrenia, antisocial personality and affective disorders. However, in other studies no statistically significant differences were observed between participants exposed and unexposed to famine in utero in the mean profile of cortisol response to psychological stress protocol [23]. Also, greater prevalence of metabolic syndrome [24], the HPA axis activity at adult age [25] and increased arterial vessel wall stiffness [26] were unaffected. Differences between studies possibly can be ascribed to the period of maternal undernutrition during gestation. [27] found more coronary heart disease, raised lipids, and altered clotting and more obesity after exposure to famine in early gestation compared to those not exposed to famine. Exposure in mid gestation was associated with obstructive airways disease and microalbuminuria. While decreased glucose tolerance was found in people exposed to famine in late gestation. This study shows that maternal undernutrition during gestation has important effects on health in later life, but that the timing of the nutritional insult determines which organ system is affected [27].
That the timing of undernutrition during the gestation period may be important for Homo sapiens may be explained by a study which found differences in brain development between rodents and humans. In the normal adult rodent and primate, arcuate nucleus (ARH) neurons function as conduits for transmitting metabolic hormonal signals into the hypothalamic circuitry that modulates feeding and energy expenditure. [28] have shown that ARH projections do not fully develop until the 3rd postnatal week in the rodent. This is in stark contrast to the nonhuman primate (NHP) in which ARH projections develop during the 3rd trimester of pregnancy. This species difference suggest that maternal diet and health are likely key factors for the development of ARH projections in the primate, whereas the postnatal environment (i.e., diet) would be more important in the rodent [28].
In contrast to the 'Dutch famine' studies were the effect of starvation was studied on the offspring, other authors investigated the effect of maternal adiposity on fetal development. [29] found that the body composition of Indian babies was influenced by maternal adiposity before pregnancy and by aspects of maternal nutritional intake and circulating nutrient concentrations during pregnancy. Increased nutrition in the face of a genetic predisposition increases maternal insulin resistance in late pregnancy and promotes fetal adiposity even in absence of marked hyperglycemia [29]. In the study of [30], -investigating historical data in families of an isolated parish village in North-Sweden the researchers found that seasonal overfeeding has transgenerational effects resulting in cardio-vascular disease and diabetes in the descendants of the second or third generation.
There are no strong paternal determinants of adiposity at birth [29]. In contrast, in the study of [31] it was demonstrated that these aspects can also become transgenerational via the male line depending if food abundance occurs during the prepubertal period. So, undernutrition and overfeeding can result in an increased risk of cardiovascular disease, Type-2 diabetes and features of the metabolic syndrome in the second or third generation. This implies a new insight in the interplay between inheritance and environment in health and development.
For the richest economies like the US - although these countries are “developed” - the “Hunger-Obesity” paradox exist. This means that people from low income groups in these developed countries, ( “the poor”, often related to social status and ethnic group) have a certain coping strategy to buy unhealthy High-fat food, which is the most satiating, to prevent hunger [32, 33]. Epidemiological studies have largely contributed to our understanding of the influence of disturbed intrauterine nutritional environment of the fetus and the consequences of these events on the health of the offspring. Intrauterine development of the fetus is related to birth size [34] and in this way can be correlated with pathogenic factors like e.g. insulin resistance (IR), glucose intolerance and T2DM in later life [4,35], increased incidence of obesity [35], hypertension and coronary artery diseases [8,36] and mental disorders like schizophrenia.
As a consequence, in the offspring Metabolic Syndrome (Obesity, hypertension, T2DM) will develop as a result of in utero environmental alterations [8,10] and implicate enhanced appetite [13], and adipogenesis as contributory factors [8, 12].
In addition, psychosocial factors like stress results in elevated stress hormone levels like catecholamines and corticosteroids. From these anti-insulin counter-regulatory stress hormones the catecholamines are released from the adrenal medulla in response to a stressor and respond in a rapid increase in cardiac output, increased physical activity and a rapid mobilization of substrates via biochemical pathways. In contrast the corticosteroids like cortisol (humans) or corticosterone (mouse) are released by the adrenal cortex and produce a slower, more sustained response, increasing the amount of glucose in the blood plasma [37]. Despite that the expectations for the regulation of Obesity where high for the in 1994 discovered hormone satiety hormone leptin, which proved to be missing in hereditary ob-ob mice [38], for humans a leptin deficiency has not proved to be a causative factor in human Obesity [39].
However, in contrast to the previous study with humans, according to the "Fetal Programming Hypothesis” [8] the offspring is for leptin associated with an increased appetite [13]. With respect to neural regulation of appetite in humans recently 10 neurophysiological pathways have been identified that can lead people to make food choices subconsciously or, in some cases, automatically. These pathways include reflexive and uncontrollable neuro-hormonal responses to food images, cues, and smells; mirror neurons that cause people to imitate the eating behavior of others without awareness; and limited cognitive capacity to make informed decisions about food [40]. So, it is not only the abundance and supply of foodstuff in combination with a sedentary lifestyle [41] but also at least 10 neurophysiological pathways that lead to increased eating behavior (Figure 2).
Figure 2: At least 10 neurophysiological pathways that lead to increased eating behavior.
The physiological development while the prenatal phase – especially that of the brain – is of particular importance for any prenatal psychology. In the first eight weeks after insemination the developing child is called embryo. After the inner organs have developed (from the ninth week on) it is called fetus. The basis of perception, experience, and behavior is the brain. While in gestation, a giant neuronal net is developing, delivering the condition for any mental process. About half of the developing neurons become destroyed again while the development of the brain because of the "programmed cell-death“(apoptosis). At birth the infantile brain contains 100 billion neurons – as many as in the brain of an adult. At birth, every cortical neuron is connected with about 2500 neurons; after a year, with about 15 000 [42]. Synapses develop, and are destroyed, over the whole life span, - a process called neuroplasticity.
In 1992 the work Piontelli a study in her book ‘From Fetus to Child: An Observational and Psychoanalytic Study’ was a breakthrough in prenatal/postnatal physiology because it uses equally the methods of academic psychology together with the hermeneutics of psychoanalysis, what makes it unique in the scientific landscape. In obtaining her dataset she examined the behavior of 11 rife fetuses using sonography. The fetuses showed a very complex behavioral repertoire and were quite different concerning their forms of activities. They reacted to stimuli in complex ways. Piontelli’s study suggested that certain prenatal experiences determined later mental life. Psychological traits, for instance enhanced oral activity, were recognizable in the prenatal phase, and also after birth. The researchers interpreted her observations in psychoanalytical terms. They saw a remarkable continuity between pre- and postnatal mental development [43,44].
[22] stated in their review that exposure to famine during gestation resulted in many physiological changes related to the metabolic syndrome [45] but also to mentally related processes like schizophrenia, antisocial personality and affective disorders. These were the first authors which related famine of the mother during gestation with mental disorders of the offspring.
So, we strongly believe in an extension of the foetal origin hypothesis for mental diseases because the human brain develops mainly in contrast the womb whereas for rodents the brain development of the pub mainly determined by environmental factors [28].
We live in a world with nearly one billion obese- [46, 47] one billion starvation- and two billion malnourished-people [48] and the status of nutrition in the womb determines according to “The Foetal Origin Hypothesis of Barker” [1] the physical health of the second and even third generation.
The most important message of this editorial that we hypothesize that also the mental health of the foetus is determined by the Body Mass Index (BMI) of the mother (obese or starvation) and/or the quality of the food (which when essential elements in nutrition are lacking is termed malnourishment), so the second or even third generation can suffer from serious mental disorders due to early nutritional condition of the mother. Because the Dutch brain bank donors are anonymous -also the Dutch famine mothers- we were unable to link their birthplace to their mental disorder.
That is why we based our hypothesis "The Foetal Origin Hypothesis of Mental Diseases" mainly on one well documented mental disorder: schizophrenia. This is a mental disorder characterized by abnormal social behaviour and failure to understand reality. Common symptoms include false beliefs, unclear or confused thinking, hearing voices that others do not, reduced social engagement and emotional expression, and a lack of motivation [49]. People with schizophrenia often have additional mental health problems such as anxiety, depressive, or substance-use disorders (50]. The causes of schizophrenia include genetic factors [51] but also poor nutrition during pregnancy [49]. Some epidemiological studies support this perception. Evidence from the 1944–1995 Dutch Hunger Winter and the 1959–1961 Chinese famines suggests that those conceived or in early gestation during famines, have a 2-fold increased risk of developing schizophrenia in adult life. This was confirmed in the study of [52] among those conceived or in early gestation at the height of famine with risk related to severity of famine conditions. [53] Investigated several candidate micronutrients as potential risk factors for schizophrenia such as folate, essential fatty acids, retinoids, vitamin D, and iron and concluded based on their mechanisms they all could contribute to this mental disorder in the population. In the study of [54] vitamin A -which is considered for gene expression and regulation, cell differentiation, proliferation and migration by the early embryo and foetus- has been linked to schizophrenia [55]. Studied using LC-MS techniques the lipid composition at molecular level in post mortem material of schizophrenic patients. Significantly lower amounts of phosphatidylcholine and phosphatidylethanolamine were found in post mortem brain tissue from schizophrenic patients than in those from control groups. In addition, strong reductions of total PUFAs and saturated fatty acids were found in schizophrenic brains, relative to control brains. Specifically, the reduced PUFAs were largely attributable to decreases in arachidonic acid (AA) and, to a lesser extent, its precursors, linoleic and eicosadienoic acids (Figure 3). There are no significant differences between the control groups with and without other mental disorders. The present findings suggest that deficits identified in peripheral membranes may also be present in the brain from schizophrenic patients. Such a deficit in membrane AA may contribute to the many biological, physiological, and clinical phenomena observed in schizophrenia [55].
In addition, elongase desaturase series, from which enzym activities can be calculated based on product-to-precursor ratios of individual measurement of fatty acids (FA) like we performed earlier [56] and depicted in figure 3.

Figure 3: Biosynthesis of long-chain omega-6 and omega-3 polyunsaturated fatty acids from dietary commodities following an elongase-desaturase series in mammals. Enzym activities can be calculated based on product-to-precursor ratios of individual measurement of fatty acids [56].
Also, in our attempts to characterize “diabetic encephalopathy” via the lipid profile of post mortem patients for Type-2 diabetes (T2DM) in human brain and plasma of the elderly with LCMS-techniques [57] we observed that the saturation index of the Cholesterylester for 16:0 was significantly higher in white matter of T2DM patients in comparison to white matter of the control group (P≤0.05) which was earlier observed in schizophrenic post mortem brain subjects [55]. So, we can cautiously conclude that FA are one or many nutritional constituents that determine the health of the brain and that the syndrome schizophrenia fits within “The Foetal Origin Hypothesis of Mental Diseases”.
Finally, the mechanism of epimutations in the germline that become permanently programmed can allow transmission of transgenerational phenotypes (e.g. T2DM) a process called epigenesis [58, 59 Figure 4]. Epigenesis is defined as heritable changes in gene expression that does not alter DNA sequence but are mitotically and transgenerational inheritable.
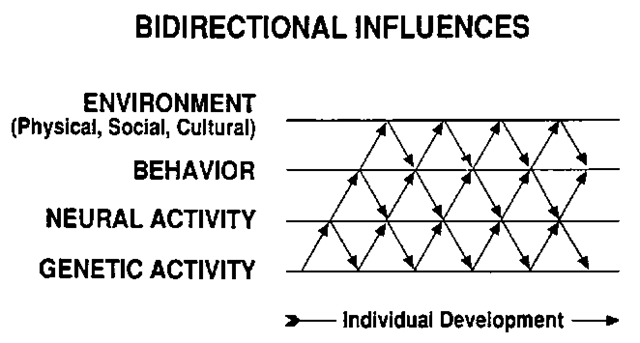
Figure 4: Epigenesis: epimutations in the germline.
It provides a framework for explaining individual variations and the uniqueness of cells, tissues, or organs despite identical genetic information. The main epigenetic mediators are
histone modification, DNA methylation, and non-coding RNAs [60]. However, the exact mechanism of epigenesis during starvation or T2DM is, as far as we know, until this moment unknown.

Figure 5: Due to an increased elderly population in Japan the projections of population structure are depicted for 2055 reflecting a skewed Gauss curve. This will have its impact for the population structure, care system and pension provision.
The consequences of “The Foetal Origins Hypothesis for Metabolic Syndrome Symptoms” [1], but also for mental health of the second and third generation will directly affect the dynamics and population structure of a certain region or country. Here is in figure 5 are the population projections depicted for the Japanese population -reflecting a Gauss curve like a kite- which is an indication for an “unhealthy” population structure.
This typical kite form for mental diseases can be explained in two ways. On the one hand, the population is getting older, which is accompanied by many brain diseases [61]. On the other hand, according to our posed “Foetal Origins Hypothesis of Mental Diseases”, these mental diseases will appear here as an increasingly younger age.
Politicians in our Western democracies often think only in the short term, for example, about a term of 4 years until the next elections and often after a few years they disappear into the forgetfulness of a well-paid mayor of a peasant village or hamlet. But it is the task of international intergovernmental organizations such as WHO, FAO, UNESCO or even the United Nations to monitor the development of population populations by region. As stated propositions: "The Foetal Origins Hypothesis of the Metabolic Syndrome" and “The Foetal Origins Hypothesis of Mental Disorders" are very carefully considered, in this way much misery can be saved in future generations.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
