
Case Report | DOI: https://doi.org/10.31579/2768-2757/078
1 Cardiovascular and Thoracic Surgery
2 Medicine
3 Anaesthesia
4 Pathology
*Corresponding Author: Prerna Singh, Cardiovascular and Thoracic Surgery.
Citation: Ankit Jain, Prerna Singh, Arindam Roy, V K Gupta, Rohan Gupta, et al, (2023), Atypical Type A Thymoma – A Rare Presentation: A Case Report. Journal of Clinical Surgery and Research, 4(3); DOI:10.31579/2768-2757/078
Copyright: © 2023, Prerna Singh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 May 2023 | Accepted: 19 May 2023 | Published: 31 May 2023
Keywords: polymastia; supernumerary; breast
Introduction: Thymomas are the most common tumor of the mediastinum with varied presentations. Here we present our experience with this tumor in a patient who was treated successfully at our department.
Case Presentation: We present a case of 29-year-old male who presented to us with intermittent cough and dull aching chest pain. Biopsy revealed moderate pleomorphism with focal areas of haemorrhage. Immunohistochemistry was suggestive of Type A thymoma. Patient underwent en-mass removal of the thymoma via midline sternotomy. Patient had a smooth post operative recovery.
Conclusion: Multidisciplinary approach is needed both for diagnosis as well as successful management of patients with thymoma.
Type A Thymoma is low grade malignant tumor. They are included in a family of aggressive tumors (1). We present this rare case which was managed successfully in our department.
A 29-year-old male presented in outpatient department with complaints of intermittent cough with dull aching chest pain. Patient was evaluated at some Pulmonary clinic where CT (Computerized Tomography) guided lung biopsy was taken, which revealed moderate pleomorphism, mitosis present, focal hemorrhage. To differentiate better immunohistochemistry was done, which was positive for Pan CK, LCA and Ki67. It was negative for CK7, CK20, Chromogranin. CECT (Contrast Enhanced Computerized Tomography Chest) suggestive of Anterior mediastinal mass (Figure 1) 6.7x6.0x9.0 cm with SUV max 2.6 and abutting the SVC & RA. PET-CT (Positron Emission Tomography) suggestive of no distant metastasis (Figure 2). Tumor markers CA 19-9, AFP, B-HCG 1.4, CA 125 was within normal limit. Diagnosis of Type A Thymoma was established. He was planned for elective surgery. A Midline Sternotomy was performed and tumor was resected en-mass. It measured approximately 12x8 cm with areas of hemorrhage. It did not invade pleura, pericardium, heart and great vessels. Postoperative recovery was uneventful (Figure 3). He was asymptomatic at 3 months of follow up.
Macroscopically it was a well encapsulated greyish brown soft tissue mass of size 11.6x 6 cm. microscopic examination showed tumor cells arranged in diffuse solid sheets and vague storiform pattern. Pleomorphism was present with ovoid to spindle shape hyperchromatic nucleus and mitotic figures less than 4 mitosis/mm2.
About 40% of mediastinal tumors are asymptomatic. Symptoms are generally due to stretching or compression on surrounding structures by the tumor. Local tumor growth causing compression to SVC may cause facial puffiness & headache. Impingement to right atrium may cause atrial fibrillation, chest pain and syncope. Pressure on trachea may cause respiratory distress and to esophagus may cause gastrointestinal symptoms such as vomiting. According to histological criteria of WHO Thymoma are classified as:
Type A (Spindle Cell)
Type AB (Mixed)
Type B1 (Lymphocyte Rich)
Type B2 (Cortical)
Type B3 (Epithelial)
Type C (Thymic Carcinoma) (2)
where Type A Thymoma is regarded as benign tumor.
Atypical type A Thymoma was added to WHO classification in 2015 with following pathological finding:
Literature suggests distant metastasis and tumor recurrence is 43% in case of Atypical Type A Thymoma (1). According to literature, patients with Type A Thymoma survival rate is 100% at 10 years of follow up (3) They are rare in first 2 decades of life. About 50% of the diagnosis are incidental in nature (4). Multidisciplinary involvement is beneficial for the management. We proceeded with midline sternotomy in view of achieving safe resection of the tumor from the vitals structures such as SVC and RA (5). In cases with clear fat planes uni-portal VATS has been advocated. In our patient, the mass was abutting the SVC & RA.
Although CECT provides the detailed anatomical delineation of the tumor, histological diagnosis helps in decision making for further management. Relationship between SUV max and WHO classification suggest that SUV max of 3.43 and 4.43 is low risk and high risk thymomas respectively (6). MRI helps to differentiate between benign and malignant tumors (7). Since facility of MRI was not available at our institute, a PET-CT was performed. Complete radiological and tumor markers assessment is necessary to differentiate it from other mediastinal tumors like Myasthenia Gravis, non seminomatous mediastinal germ cell tumor (NSGCT), lymphoma. Although identifying the nature of the lesion by tissue biopsy remain controversial (8), benefits of recognizing the lesion before surgery helps to give Neo-adiuvant chemotherapy making lesion amenable for resection.
In our case the patient had already undergone a CT guided biopsy. Differentiating from other pathological condition, remains a challenge for pathologist particularly when there is extensive necrosis (9). In our case since there was minimal necrosis so, Spindle Cell Carcinoid becomes less obvious. Also, the absence of positive neuroendocrine marker makes it more unfavourable. Atypical Thymoma type A is usually well circumscribed. Absence of invasion to adjacent organ with easy resectability is more in line with the diagnosis.
Anesthesiological consideration is of utmost important as any injury to SVC during resection can be fatal thus vascular access in low extremity is important and can be lifesaving. In cases where vascular injury has occurred, Cardiopulmonary bypass and Perfusionist should be readily accessible to provide a rescue. Where SVC is suspected to be involved an extra caution is must as additional monitoring modality like Near Infrared Spectroscopy, Transcranial Doppler is recommended (10).
Post-operative follow up should not be limited to chest imaging but also to extra thoracic. cavity is necessary. So, we have planned the patient to undergo PET CT annually three consecutive years and there by deciding later.
Patients with mediastinal mass should undergo CT guided biopsy followed by surgery for better diagnosis and management. We recommend multidisciplinary approach to provide disease free survival.
Abbreviations: TB:Tuberculosis, ATT:Anti-Tubercular Drugs, CECT: Contrast Enhanced Computerised Tomography, SVC: Superior Vena Cava, RA: Right Atrium, PETCT: Positron Emission Tomogarphy Computerised Tomography, AFP: Alfa Feto-Protein, CA125: Cancer Antigen125,Beta- Human Chorionic Gonadotropin CK: Cytokeratin LCA: Leukocyte Common Antigen SVC: Superior Vena Cava
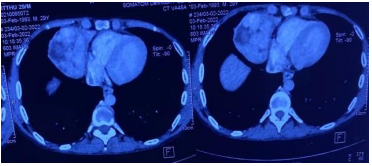
Figure1: Preoperative CT Scan images showing anterior mediastinal mass, thymoma
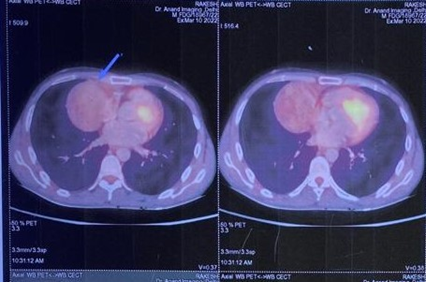
Figure 2: PET scan of the patient done pre operatively
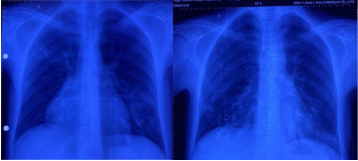
Figure 3: Pre and post operative Chest Xray of the patient
The authors received no financial support for the case report.
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this case report.
Since this is a case report, ethical approval was not required by the Institutional Ethics Committee.
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
All relevant data is with the authors and shall be provided as and when asked.
Not applicable
Study concept: Ankit Jain, Arindam Roy
Data Collection: Ragi Jain, Mona Bargotya
Writing and Corresponding Author: Prerna Singh
Revising and critical review: V K Gupta, Rohan Gupta
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
