
Review Article | DOI: https://doi.org/ 10.31579/2640-1045/031
*Corresponding Author: Elm Rogers ;Department of Medicine, Division of Endocrinology
Citation: Elm Rogers, Kassa A Lochnan; Reproductive Endocrinology: Pregnancy and Postpartum Thyroid Disorders in Women, Doi 10.31579/2640-1045/031
Copyright: © 2018. Elm Rogers , This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 10 April 2018 | Accepted: 25 April 2018 | Published: 10 May 2018
Keywords: spontaneous miscarriage; gestational diabetes; postpartum thyroiditis
Reproductive Endocrinology is a medical specialty for infertility, menopause, and other issues with reproductive hormones. Reproductive endocrinologists are OB/GYN (obstetrics and gynecology) doctors with special training to help both men and women with problems related to reproductive hormones.
Sometimes, this specialty is called reproductive endocrinology and infertility because much of their work focuses on helping women to become pregnant and carry a baby to term.
Reproduction is a fundamental aspect of life in all species. In a biological sense, it can be argued that reproduction is the essence of life. Passing on ones genes to the next generation and constantly optimizing the gene pool available for each individual and the species as a whole are vital for continuation and endurance of the species. Reproduction and hormones are intimately connected; thus, hormones are a prerequisite for reproduction and govern nearly all aspects of successful creation in both females and males. Therefore, to numerous scientists, reproductive endocrinology is one of the most fascinating disciplines in science, and it is a pleasure that now finally there is a scientific journal dedicated specifically to reproductive endocrinology.
The development of multiple follicles via stimulation with exogenous FSH preparations has invariably been accompanied with supra-physiological levels of estradiol and progesterone as each follicle contributes to the overall concentration observed in circulation. Many effects of estradiol in the body are obviously reinforced by these high levels, including a risk of inducing a pituitary premature LH surge and also negative effects on the receptivity of the endometrium. Recent years have shown that the endometrium is inappropriately affected by high levels of estradiol and the progesterone during the early luteal phase. It has, somewhat surprising, now been shown that—if an efficient program for freezing oocytes and embryos is available—results of a freeze-all strategy with replacement in a subsequent natural cycle leads to higher reproductive outcomes, probably due to a more appropriate stimulation of the endometrium. This has raised questions on whether it is possible to reduce the output or the effect of estradiol during the follicular phase by for instance co-administrating aromatase inhibitors or estrogen receptor antagonists to avoid the estrogenic effect on the endometrium.
There is now also a move toward new strategies for ovarian stimulation, more in accordance with the gonadotropin actions of the natural cycle. One such option is to mimic the natural menstrual cycle and use either exogenous LH or hCG for stimulation of follicular growth in the second half of the follicular phase until ovulation induction where LH receptors are expressed on the granulosa cells and exogenous LH or hCG may substitute for exogenous FSH.
In the vast majority of cases, the pituitary is fully capable of producing all the FSH and LH that is required for stimulation of multiple follicular development—we need to be able to control its release, and a number of new combinations of old and new drugs are now becoming interesting and will probably be part of new stimulation regimes. It is also of interest to follow the development of new hormones for stimulation with a prolonged half-life and a pharmacokinetic profile that resembles more the release of the hormones in the natural cycle.
Pregnant Woman with Thyroid Disease
Pregnancy has a profound impact on the thyroid gland. During a normal pregnancy the thyroid increases in size, produces 50% more T4 and T3, requires 50% more iodine, and the normal TSH range is compressed with a lower limit of normal at both ends of the spectrum. It is therefore not surprising that pregnancy has been considered a physiological stress test for the thyroid gland (1). However, what has been striking is the research over the last 20 yr linking thyroid hormonal abnormalities and thyroid autoimmunity to a wide range of adverse pregnancy, maternal, and offspring outcomes including spontaneous miscarriage, gestational hypertension, preeclampsia, gestational diabetes, postpartum thyroiditis, and decreased IQ in the offspring.
The rapidly evolving literature on the interaction between the thyroid and pregnancy was the impetus for an update of the 2007 Endocrine Society Guidelines (ES-G) (2). Included in the 2012 ES-G (3) are 27 articles published since the completion of the 2007 ES-G. Using a comprehensive and scholarly process, and the product of an international committee of experts in the field, the 2012 ES-G provide 52 recommendations for the care of the pregnant woman with thyroid disorders. The authors of the 2012 ES-G should be applauded for the high quality of the recommendations and their ability to synthesize data in a complex and rapidly evolving field.
Women with thyroid disorders in pregnancy should be followed up by their GP in the postpartum period. Postpartum thyroiditis may present months after delivery.
Normal thyroid function is essential for fetal development. A deficiency or an excess of thyroid hormone can occur in pregnancy. Thyroid dysfunction can cause problems for both the mother and baby.Sometimes the hypothyroidism or hyperthyroidism is subclinical.
Table 1
Prevalence of thyroid disorders in pregnancy
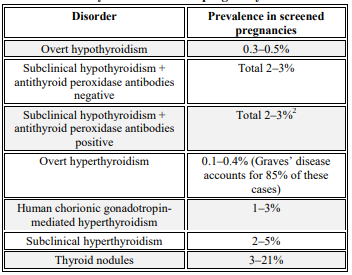
Universal screening in pregnancy is currently not recommended, but is recommended for women with a higher risk of thyroid dysfunction.
Physiology
During pregnancy the thyroid gland undergoes hyperplasia and increased vascularity. Circulating iodine is reduced and thyroid-binding globulin increases.
The rising concentration of beta-human chorionic gonadotrophin (HCG) in the first trimester can directly stimulate the thyroid stimulating hormone (TSH) receptor as HCG has structural similarities to TSH. This in turn leads to increased free triidothyronine (fT3) and free thyroxine (fT4), suppressing TSH secretion. A serum TSH below 0.1 mIU/L may be present in 5% of women by the 11th week of pregnancy.
Iodine supplementation
Women have an increased iodine requirement during pregnancy and lactation due to increased thyroid hormone production, increased renal iodine excretion and fetal iodine requirements. The National Health and Medical Research Council recommends pregnant and breastfeeding women take a daily supplement of iodine 150 micrograms. The recommended total daily intake of iodine in pregnancy is 250 micrograms.
Women with hypothyroidism
For women with overt hypothyroidism who are planning pregnancy, guidelines recommend optimisation of TSH before conception. Thyroid dysfunction in pregnancy is clinically important as insufficient thyroxine is associated with an increased risk of premature birth, low birth weight and miscarriage
After conception, an increase in thyroxine as soon as possible is recommended with the goal of normalising the TSH concentration. An easy approach is to increase the total weekly thyroxine dose by an extra two tablets per week or by 20–30% of the baseline dose when pregnancy is confirmed.
Serum TSH should be monitored every four weeks in the first trimester to ensure the woman is euthyroid, and then six to eight weekly therafter.Thyroid function tests should be rechecked four weeks after any dosage adjustments to ensure euthyroid levels are maintained. Aim to maintain TSH in the range 0.5–2.5 mIU/L.
Hypothyroidism diagnosed during pregnancy
A new diagnosis of overt hypothyroidism should warrant immediate thyroxine replacement and further investigation for the presence of thyroid auto-antibodies:
antithyroid peroxidase antibodies (antiTPO)
antithyroglobulin antibodies (TgAb)
thyrotropin receptor antibodies (TRAb) (if there is a history of treated Graves’ disease).
Participants:
The Chair was selected by the Clinical Guidelines Subcommittee (CGS) of The Endocrine Society. The Chair requested participation by the Latin American Thyroid Society, the Asia and Oceania Thyroid Society, the American Thyroid Association, the European Thyroid Association, and the American Association of Clinical Endocrinologists, and each organization appointed a member to the task force. Two members of The Endocrine Society were also asked to participate. The group worked on the guidelines for 2 yr and held two meetings. There was no corporate funding, and no members received remuneration.
Iodine Nutrition during Pregnancy
Women of childbearing age should have an average iodine intake of 150 μg/d. During pregnancy and breastfeeding, women should increase their daily iodine intake to 250 μg on average. USPSTF recommendation level is A; evidence is good.
Iodine intake during pregnancy and breastfeeding should not exceed twice the daily recommended nutritional intake for iodine, i.e. 500 μg iodine per day. USPSTF recommendation level is I; evidence is poor.
To assess the adequacy of the iodine intake during pregnancy in a population, urinary iodine concentration should be measured in a cohort of the population. Urinary iodine concentration should ideally range between 150 and 250 μg/liter. USPSTF recommendation level is A; evidence is good.
POSTPARTUM THYROIDITIS
There are insufficient data to recommend screening of all women for PPT. USPSTF recommendation level is I; evidence is poor
Women known to be thyroid peroxidase antibody positive should have a TSH performed at 3 and 6 months postpartum USPSTF recommendation level is A; evidence is good.
The prevalence of PPT in women with type 1 diabetes is 3-fold greater than in the general population. Postpartum screening (TSH determination) is recommended for women with type 1 diabetes mellitus at 3 and 6 months postpartum. USPSTF recommendation level is B; evidence is fair.
Thyroid dysfunction during pregnancy and the postpartum period is a common obstetric problem primarily managed by GPs. At-risk women are screened, but universal thyroid function screening is currently not recommended during pregnancy or postpartum.
Thyroxine is used for treating overt hypothyroidism and is recommended in antibody positive subclinical hypothyroidism. For hyperthyroidism, propylthiouracil is the preferred antithyroid drug in the preconception and first trimester to reduce the risk of teratogenicity. Carbimazole may be used in the second trimester.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
