
Review Article | DOI: https://doi.org/10.31579/2640-1045/018
*Corresponding Author: Avimelech Adedeji, Division of Diabetology and Endocrinology Israel.
Citation: Avimelech Adedeji ,Alice Borishade, Diabetic Ketoacidosis: A Review of Risk Associated Morbidity and Mortality. J. Endocrinology and Disorders. Doi:10.31579/2640-1045/018
Copyright: © 2018. Avimelech Adedeji. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 January 2018 | Accepted: 12 January 2018 | Published: 19 January 2018
Keywords: diabetic ketoacidosis, diabetes, insulin, rehydration, hypoglycemia, hypokalemia, metabolic acidosis, protocol.
Diabetic ketoacidosis (DKA) is a rare yet potentially fatal hyperglycemic crisis that can occur in patients with both type 1 and 2 diabetes mellitus. Due to its increasing incidence and economic impact related to the treatment and associated morbidity, effective management and prevention is key. Elements of management include making the appropriate diagnosis using current laboratory tools and clinical criteria and coordinating fluid resuscitation, insulin therapy, and electrolyte replacement through feedback obtained from timely patient monitoring and knowledge of resolution criteria. In addition, awareness of special populations such as patients with renal disease presenting with DKA is important. During the DKA therapy, complications may arise and appropriate strategies to prevent these complications are required. DKA prevention strategies including patient and provider education are important.
Diabetic ketoacidosis (DKA) is characterised by the triad of hyperglycemia, ketosis, and metabolic acidosis. This results from a relative or absolute deficiency of insulin and an excess of counter-regulatory hormones including glucagon, cortisol, catecholamines, and growth hormones leading to hyperglycemia, glycosuria, dehydration, and hyperosmolarity of varying severity. lycosuria induces an osmotic diuresis, which results in significant deficits in fluid and electrolytes including sodium, potassium, calcium, magnesium, chloride, and phosphate [3]. Dehydration and hyperglycemia results in hypertonicity and an efflux of water from the intracellular space to the hypertonic extracellular space. There is also a potassium efflux from the intracellular space, aggravated by acidosis, lack of effective insulin action, and breakdown of intracellular proteins [3].
Diabetic ketoacidosis more often complicates type 1 rather than type 2 diabetes mellitus and carries the risk of significant morbidity and mortality [1, 4, 5]. Despite evolving practice, there are increasing numbers of hospital admissions for DKA and hyperosmolar hyperglycaemic state (HHS) [1, 6, 7]. DKA is associated with mortality rates as high as 5–9% in the elderly and in patients with severe comorbidities [1, 8]. Though mortality from DKA is more often attributable to severe underlying illness and comorbidities [1], DKA itself is a hypercoagulable state resulting in potentially fatal complications including stroke, myocardial infarction, and disseminated intravascular coagulation [9, 10]. Management involves rehydration, correction of electrolyte derangements; particularly hypokalaemia, administration of insulin, correction of metabolic acidosis, and treatment of precipitants such as infection, pancreatitis, trauma, and myocardial infarction [11–13].
Aims of Review
This review is intended to assist those writing and utilising DKA management protocols in adults to appreciate deficits in current knowledge and to draw attention to areas that may benefit from future research.
We reviewed the original studies considering key elements of inpatient management of DKA including the choice of intravenous fluids and rates of replacement; insulin infusion rates, and routes of administration; potassium replacement rates; and the role of bicarbonate and phosphate replacement.
Hydration
Patients with DKA experience osmotic diuresis, resulting in hyperosmolar intracellular dehydration [14]. Fluid deficits may be up to 10% of total body weight [1, 5]. There is also an accumulation of β-hydroxybutyrate and acetoacetate, which results in a high anion gap metabolic acidosis [1]. Prompt rehydration is vital to restore circulating volume and tissue perfusion, clear ketones, and correct electrolyte imbalances [1, 5, 14]. Independent of insulin therapy, hydration alone restores circulatory volume and tissue perfusion; improves glycaemic control and acid base balance, and reduces counterregulatory hormones.
However, specifically hydroxyethyl starch crystalloids were associated with a significant increase in mortality and acute kidney injury, and it was concluded that they should be avoided [14–19]. It is important to note that none of the included studies specifically considered these fluids in the setting of DKA.
During the recovery phase of DKA, hyperchloraemia tends to develop because of preferential excretion of ketones during rehydration and improved renal perfusion, resulting in a raised anion gap metabolic acidosis [14]. It is proposed that rehydration with normal saline may contribute to hyperchloraemia and a hyperchloraemic metabolic acidosis with a persisting base deficit and may cause renal vasoconstriction and decreased glomerular filtration rate [14, 27]. Alternatively, this acidosis may represent a physiological response to resolving DKA rather than a result of the hydration fluid itself [17, 20–23, 28].
The only other RCT was also small, studied different crystalloids in DKA, comparing patients who received Ringer’s lactate (a balanced electrolyte solution) (n = 28) with patients who received normal saline (n = 29). In this study, Ringer’s lactate offered no significant superiority in time to normalisation of pH and took a significantly longer time to achieve a blood glucose concentration ≤14mmol/L [26]. A proposed mechanism for this delay in control of blood glucose level was that lactate from Ringer’s solution provided excess substrate for ongoing gluconeogenesis [26]. Using the 2006 (and then the 2009 post hoc) American Diabetes Association (ADA) definitions for resolution of DKA, fluid selection made no statistically significant difference in time to resolution [26].
Potassium Replacement—Dose and Rates
Patients with DKA are often found to initially have mild to moderate hyperkalaemia, despite a total body deficit of potassium [1]. The initiation of insulin causes an intracellular shift of potassium and lowers the potassium concentration potentially resulting in severe hypokalaemia. Hence patients with serum potassium levels <3>
Insulin Administration
Once hypokalaemia is corrected and hydration commenced, insulin should be administered to halt lipolysis, ketogenesis, and correct hyperglycaemia. Regular insulin is favoured over insulin analogues. The current mainstay of insulin therapy in DKA is continuous intravenous infusion for its rapid onset and ease of dose titration [1, 2]. Some institutions require intravenous insulin infusions to be managed in the intensive care setting and thus some advocate for the use of subcutaneous or intramuscular injections in order to avoid an intensive care admission [1, 46–48].
Insulin—Role of Initial Intravenous Insulin Bolus
An initial intravenous insulin bolus has been considered in multiple small trials.
A small prospective analysis in 1995 found patients who received an insulin bolus had a significantly higher incidence of hypoglycemia but no difference in hypokalaemia [57].
In contrast, a prospective observational cohort study in 2007 (n = 157) found no statistical difference in the incidence of hypoglycaemia, rate of glucose reduction, or length of hospital stay [63] and concluded that an initial bolus of intravenous insulin offered no significant clinical benefit or harm. The study was limited by lack of randomisation; standardised treatment protocols and used administration of 50
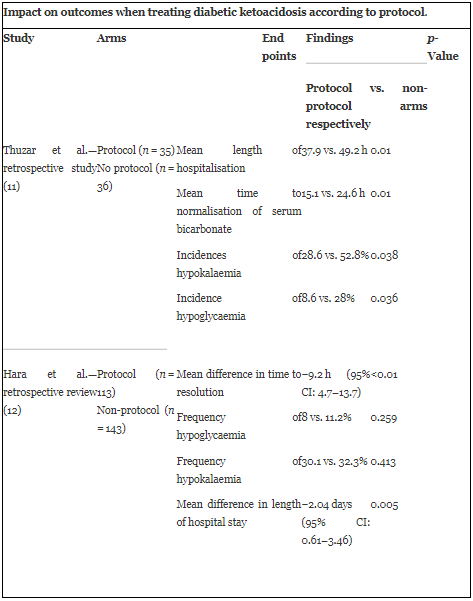
Regarding protocol impact on DKA treatment outcomes, a retrospective study compared patients managed with and without local protocol, found that patients treated with a local protocol had a significantly shorter mean time to normalisation of serum bicarbonate, lower incidences of hypokalaemia, and lower incidence of hypoglycaemia, and no significant difference in total insulin dose (Table1 ).
On review, the strength and breadth of original evidence is limited. Current weak evidence suggests crystalloids are preferred over colloids. There is no clear evidence for superiority of a given crystalloid nor for a given rate of rehydration.
Low-dose insulin has limited evidence for superior safety over high-dose insulin. Administering bolus insulin prior to low-dose insulin infusions <0>
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
