
Research Article | DOI: https://doi.org/10.31579/2640-1045/094
*Corresponding Author: Sonallah Ibrahim, Department of Endocrinology,Egypt.
Citation: Sonallah Ibrahim, Mohammad Sharkawi, Ahmed Mourad.Classification of Neuroendocrine Tumors: Consensus Guidelines for the Management and Treatment. J. Endocrinology and Disorders. 1 (2): DOI:10.31579/2640-1045/094
Copyright: © 2017. Sonallah Ibrahim. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 March 2017 | Accepted: 19 April 2017 | Published: 27 May 2017
Keywords: neuroendocrine tumors; thyroid cancer; adrenal gland tumors; gastroenteropancreatic
Neuroendocrine tumors (NETs) are neoplasms that arise from cells of the endocrine (hormonal) and nervous systems. Many are benign, while some are malignant. They most commonly occur in the intestine, where they are often called carcinoid tumors, but they are also found in the pancreas, lung and the rest of the body.
Although there are many kinds of NETs, they are treated as a group of tissue because the cells of these neoplasms share common features, such as looking similar, having special secretory granules, and often producing biogenic amines and polypeptide hormones.
Neuroendocrine tumors (NETs) arise in most organs of the body and share many common pathologic features. However, a variety of different organ-specific systems have been developed for nomenclature, grading, and staging of NETs, causing much confusion. This review examines issues in the pathologic assessment of NETs that are common among primaries of different sites. The various systems of nomenclature are compared along with new proposal for grading and staging NETs. Although differences persist, there are many common themes, such as the distinction of well-differentiated (low and intermediate-grade) from poorly differentiated (high-grade) NETs and the significance of proliferative rate in prognostic assessment. A recently published minimum pathology data set is presented to help standardize the information in pathology reports. Although an ultimate goal of standardizing the pathologic classification of all NETs, irrespective of primary site, remains elusive, an understanding of the common themes among the different current systems will permit easier translation of information relevant to prognosis and treatment.
Types of neuroendocrine tumors
There are many types of neuroendocrine tumors. This section focuses on 3 specific types: pheochromocytoma, Merkel cell cancer, and neuroendocrine carcinoma. Other types of tumors that begin in hormone-producing cells are described in their own sections on Cancer.Net, including pancreatic neuroendocrine tumors, thyroid cancer, adrenal gland tumors, and pituitary gland tumors.
Pheochromocytoma. Pheochromocytoma is a rare tumor that begins in the chromaffin cells of the adrenal gland. These specialized cells release the hormone adrenaline during times of stress. Pheochromocytoma most often occurs in the adrenal medulla, the area inside the adrenal glands. This type of tumor increases the production of the hormones adrenaline and noradrenaline, which increase blood pressure and heart rate. Even though a pheochromocytoma is usually benign, it may still be life-threatening because the tumor may release large amounts of adrenaline into the bloodstream after injury. Among people with pheochromocytoma, 80% have a tumor in 1 adrenal gland, 10% have tumors in both glands, and 10% have a tumor outside the adrenal glands.
Merkel cell cancer. Merkel cell cancer is a highly aggressive, or fast-growing, rare cancer. It starts in hormone-producing cells just beneath the skin and in the hair follicles. It is usually found in the head and neck region. Merkel cell cancer may also be called neuroendocrine carcinoma of the skin or trabecular cancer.
Neuroendocrine carcinoma. Around 60% of neuroendocrine tumors cannot be described as anything other than “neuroendocrine carcinoma.” Neuroendocrine carcinoma can start in a number of places in the body, including the lungs, brain, and gastrointestinal tract.
NOMENCLATURE ISSUES
Classification
The World Health Organization (WHO) classification scheme places neuroendocrine tumors into three main categories, which emphasize the tumor grade rather than the anatomical origin.
well-differentiated neuroendocrine tumours, further subdivided into tumors with benign and those with uncertain behavior
well-differentiated (low grade) neuroendocrine carcinomas with low-grade malignant behavior
Poorly differentiated (high grade) neuroendocrine carcinomas, which are the large cell neuroendocrine and small cell carcinomas.
The systems of nomenclature reflect differentiation and grading features of NETs. In essentially all systems, a sharp division is made between well-differentiated and poorly differentiated tumors, with the latter group being clearly designated as high-grade neuroendocrine carcinomas (neuroendocrine carcinoma, grade 3), including small-cell carcinoma and large-cell neuroendocrine carcinoma variants. Combined (mixed) forms with elements of non-neuroendocrine carcinoma (usually adenocarcinoma or squamous cell carcinoma) are also well recognized. The distinction of well-differentiated from poorly differentiated NETs is probably one of the most important pathologic assessments related to these neoplasms, as the biologic behavior of the well-differentiated group is often rather indolent, whereas poorly differentiated neuroendocrine carcinomas are very highly aggressive; therapy also differs significantly between these 2 categories of tumors. The term carcinoma also has been applied to well-differentiated tumors, however. In some systems (particularly the prior 2001 and 2004 versions of the WHO classifications of digestive and pancreatic NETs, carcinoma was used in the place of tumor for neoplasms with obvious evidence of malignant behavior, such as vascular invasion, gross local invasion, or metastases. Others have argued to use the term carcinoma for all NETs to specify that all are regarded to be malignant. However, the use of the same term for all grades of NETs implies a relationship between the well-differentiated and poorly differentiated groups that does not exist in most instances. It is most important to recognize that the unqualified terms neuroendocrine carcinoma and neuroendocrine tumor, without reference to grade or differentiation, are inadequate for prognostication or therapy and considered inappropriate in pathology reports.
The issue of functionality of NETs also impacts on nomenclature. Functioning NETs are defined based on the presence of clinical symptoms due to excess hormone secretion by the tumor and include functioning carcinoid tumors and a variety of other functioning NETs arising in the pancreas or elsewhere. Terms reflecting the clinical syndromes may be applied to these NETs, such as insulinoma, glucagonoma, and gastrinoma, although the term carcinoid tumor is used for tumors with or without the carcinoid syndrome. Although there are prognostic implications to some of the functional categories (eg, insulinomas are generally very indolent), the biologic behavior of most functioning NETs is still defined by the grade and stage of the tumor (although the clinical consequences of the hormone hypersecretion can be significant). Furthermore, the functional status of the tumor is defined by the clinical findings, not by the pathologic appearance or immunohistochemical profile. Thus, the pathologic diagnosis of functioning NETs should be the same as for analogous nonfunctioning NETs of the same anatomic site, with the descriptive functional designation appended to the diagnosis when there is knowledge of a clinical syndrome
GRADING ISSUES
Neuroendocrine lesions are graded histologically according to markers of cellular proliferation, rather than cellular polymorphism. The following grading scheme is currently recommended for all gastroenteropancreatic neuroendocrine neoplasms by the World Health Organisation
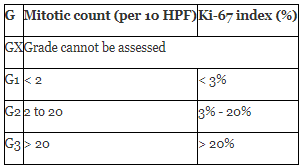
If mitotic count and ki67 are discordant, the figure which gives the highest grade is used.
G1 and G2 neuroendocrine neoplasms are called neuroendocrine tumors (NETs) - formerly called carcinoid tumours. G3 neoplasms are called neuroendocrine carcinomas (NECs).
It has been proposed that the current G3 category be further separated into histologically well-differentiated and poorly-differentiated neoplasms to better reflect prognosis.
The proliferative rate has been repeatedly shown to provide significant prognostic information for NETs, and most systems of grading rely extensively on the proliferative rate to separate low-, intermediate-, and high-grade tumors. Some systems (such as the WHO classification for lung and thymus) include the presence of necrosis as a feature to distinguish intermediate grade from low grade within the well-differentiated group.The proliferative rate can be assessed as the number of mitoses per unit area of tumor (usually expressed as mitoses per 10 high-power microscopic fields or per 2 mm2) or as the percentage of neoplastic cells immunolabeling for the proliferation marker Ki67.The WHO classification of lung and thymus tumors relies only on the mitotic rate,whereas the system recently proposed for gastroenteropancreatic NETs by the European Neuroendocrine Tumor Society (ENETS) and also now recommended by the WHO uses either mitotic rate or Ki67 labeling index. A comparison of the most widely used grading systems is shown in As can be seen, the cut-points to distinguish the 3 grades vary somewhat among the different systems, and definitive clinical data to determine the optimal cut-points do not exist. In fact, some studies suggest that the optimal cut-points may differ between organ systems.For these reasons, it is recommended to specify the actual proliferative rate in the pathology report, in addition to designating a grade based on a system that is specifically referenced.
STAGING ISSUES
Currently there is no one staging system for all neuroendocrine neoplasms. Well differentiated lesions generally have their own staging system based on anatomical location, whereas poorly differentiated and mixed lesions are staged as carcinomas of that location. For example, gastric NEC and mixed adenoneuroendocrine cancers are staged as a primary carcinoma of the stomach.
TNM staging of gastroenteropancreatic Grade 1 and Grade 2 neuroendocrine tumors is as follows:
Stomach
Duodenum / Ampulla of Vater
Jejunum and Ileum
Colon and Rectum
Pancreas
A few years ago, no formal TNM-based staging systems existed for NETs. Data submitted to the Surveillance, Epidemiology, and End Results (SEER) program of the National Cancer Institute separated tumors into localized, regional, and distant stages based on the presence of lymph node or distant metastases, but substratification of the extent of the primary tumor was not performed. Recently, TNM staging systems have been proposed. The American Joint Committee on Cancer has recently published a new TNM staging manual that includes NETs of all anatomic sites,and the ENETS has previously published recommendations for TNM staging of gastroenteropancreatic NETs.There are some differences between these systems, particularly for primary tumors of the pancreas and the appendix, but there is also considerable overlap. Additionally, the staging criteria for both systems rely predominantly on the size of the tumor and the extent of invasion into similar landmarks as used for the staging of non-neuroendocrine carcinomas of the same sites. It is recommended that the extent of involvement of these structures be specifically indicated in the pathology reports in addition to providing a TNM stage using a system that is specifically referenced.
Until very recently, the WHO classifications for NETs of the tubular gastrointestinal tract (2000) and pancreas (2004) used a hybrid classification system that incorporated both staging information (size and extent of tumor-limited to the primary site versus having metastases) and grading information (proliferative rate) into a single prognostic prediction system, with a different name being applied to the tumors in each prognostic group.Although this system did allow prognostic stratification of NETs, it did not allow for grading information to be applied to advanced stages of disease, preventing prognostication once metastases occurred and therefore limiting information for therapeutic decision making.Furthermore, the implications of this classification were that the name for a NET limited to the primary site was different than that to be used for the same tumor once metastases occurred in the future, a relatively common occurrence for some NETs. Because of these limitations, the most recent WHO classification that applies to all gastroenteropancreatic NET has abandoned the hybrid classification system in favor of separately grading and staging the tumors This will bring the WHO system more closely in line with other widely used systems.
OTHER PATHOLOGY INFORMATION
A variety of other pathologic findings may be of use in the prognostication and management of patients with NETs. Immunolabeling for general neuroendocrine markers (chromogranin A and synaptophysin) may not be needed in histologically typical resected primary tumors, but it is very useful to confirm the nature of the tumor based on biopsy specimens in many cases. Immunolabeling for specific peptide hormones is only useful in highly defined circumstances, however. Adverse prognostic factors not included in grading and staging, such as vascular or perineural invasion, should be documented. Adequacy of surgical resection should be indicated, and the number of involved lymph nodes (and the total number of nodes examined) should also be stated. Histologic abnormalities of the neuroendocrine cells in the surrounding tissues (such as neuroendocrine hyperplasia in the lung or stomach) should be described. A variety of prognostic or treatment-related biomarkers has been investigated, and some may have significant utility in the future, but currently, none is recommended to be routinely used outside of specific research settings. Finally, markers of primary origin now exist for metastatic NETs of unknown origin. For well-differentiated NETs, thyroid transcription factor-1 (TTF1) labeling favors pulmonary origin, CDX2 expression is typical of intestinal or pancreatic primaries, and PDX1 or Isl1 are most commonly expressed in pancreatic NETs.
Management and Treatment
Indications for Targeted Therapies
Based on the aforementioned phase 3 clinical trials, sunitinib and everolimus are Food and Drug Administration approved and recommended for patients with progressive metastatic pancreatic NETs. Everolimus was also studied in metastatic functional (ie, hormone secreting) carcinoid tumors in a large phase 3 clinical trial. Although this study did not meet its primary endpoint of PFS, there was a trend toward longer PFS in the treatment arm.
Indications for Cytotoxic Therapies
Cytotoxic therapies such as streptozocin, 5-fluorouracil, or temozolomide should be considered in the palliation of patients with advanced pancreatic NET and symptoms related to tumor bulk. There are no prospective randomized data for a temozolomide-based regimen; however, a single-institution series showed promising activity, and randomized clinical trials using temozolomide are planned. Cytotoxic therapies are currently listed as “consider” for pancreatic NET. There is currently no known role for cytotoxic therapies in advanced carcinoid.
Serum Biomarkers in Diagnosis and Surveillance
Plasma chromogranin A (CgA) and 24-hour urinary 5-hydroxyindoleacetic acid (5-HIAA) levels can be elevated as surrogate markers of possible progression or response. 5-Hydroxyindoleacetic acid is not as useful in patients with foregut (bronchial or gastric) or hindgut (rectal) NETs or in most patients with pancreatic NETs that do not secrete serotonin. Chromogranin A is a 49-kd protein that is contained in the neurosecretory vesicles of the NET cells and is commonly detected in the plasma of patients with endocrine neoplasms. Elevated plasma CgA levels have been associated with poor overall prognosis in patients with NETs.Additionally, early decreases may be associated with favorable treatment outcomes in some studies. The committee “recommends” following CgA levels in patients with advanced disease in patients who have elevated CgA levels at diagnosis and “considers” following CgA in resected disease.
Despite the inability to establish a single system of nomenclature, grading, and staging for NETs of all sites, there are common features to form the basis of most systems. Documentation of these features will allow greater reliability in the pathology reporting of these neoplasms. Hopefully, future clinicopathologic studies will help further define the optimal criteria to subclassify NETs.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
