
Research | DOI: https://doi.org/10.31579/2693-4779/051
*Corresponding Author: Richmond Ronald Gomes, Associate Professor, Medicine, Ad-din Women's Medical College Hospital, Dhaka, Bangladesh.
Citation: S Islam, R RGomes, FM M Hasan. (2021). Evaluation of Clinical Presentation and Associated Comorbid Conditions in Patients with Spontaneous Intracerebral Hemorrhage in a Tertiary Care Hospital in Bangladesh. Clinical Research and Clinical Trials. 4(1); DOI: 10.31579/2693-4779/051
Copyright: © 2021 Richmond Ronald Gomes. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 June 2021 | Accepted: 25 June 2021 | Published: 19 July 2021
Keywords: spontaneous, intracerebral hemorrhage, osmotherapy,seizure,glasgow coma scale
Spontaneous intracerebral hemorrhage (ICH) has remained the least treatable form of stroke despite recent improvements in medical treatment. Treatment usually supportive and medical such as ventilatory support, blood pressure reduction, osmotherapy, fever control, seizure control and nutritional support and treatment of co morbidconditions. This study was carried out to see demographic variability, clinical presentation, causes and outcome of spontaneous intracerebral hemorrhage.
Methods and materials: This was a cross sectional observational prospective in study on 50 spontaneous ICH patients admitted in Medicine department of Khulna Medical College Hospital from November 2020 to April, 2021.
Result: The study showed that spontaneous ICH was most common in between 41-70 years. Their age frequency were 14 (28%) in 41-50 years, 15 (30%)in 51- 60 years, 12 (24%) in 61-70 years, 5 (10%) in 71- 80 years and 4 (8%) in more than 81 years age group. Among the patients, 64% (32) were male and 36% (18) were female. No of smoker male was 25(50%) and female was 1(2%) and no of nonsmoker male was 7(14%) and female was 17(34%). Headache was present in 56% (28) and absent in 44% (22) of patients. Vomiting was present in 54% (27) and was absent in 46% (23)of patients.Seizure was present in 16% (8) and was absent in 54% (42) of patients. Diabetes mellitus was present in 22% (11) of patients and absent in 78% (39) patients. Range of blood pressure –<140/90 in 24%(12), Systolic BP:140-159/Diastolic BP:90-99 (mm Hg) in 10%(5), Systolic BP:160-179/Diastolic BP:100-109 (mm Hg) in 22%(11),Systolic BP:180 or more/Diastolic BP:110 or more (mm Hg) in 44%(22) patients. Dyslipidemia was present in 30% (15) & absent in 70% (35) patients. Glasgow Coma Scale Score was 8 or less in 42% (21) and 9 or more in 58% (29) patients. Conclusion: Spontaneous ICH is common in Indian subcontinent. As death occur due to ICH itself, associated co morbidities or due to complications, management in stroke care unit, High dependency unit and Intensive care unit is required.
Cerebrovascular diseases are the third leading cause of death after heart disease and cancer in developed countries. They also come first in terms of causing death and disability in neurologic diseases in adults [1]. Nontraumatic intracerebral hemorrhage is bleeding into the parenchyma of the brain that may extendinto the ventricles and, in rare cases, the subarachnoid space. Spontaneous intracerebral hemorrhage is second most common causes of stroke following ischemic stroke.Depending on the underlying cause of bleeding; intracerebral hemorrhage is classified as either primary or secondary. Primary intracerebral hemorrhage accounting for 78%-88% of all cases, originates from the spontaneous rupture of small vessels damaged by chronic hypertension or amyloid angiopathy [2]. The worldwide incidence of intracerebral hemorrhage from 10-20 cases per 100000 population, [3, 4] and increases with age [3,5]. Intracerebral hemorrhage is more common in men than women, particularly those older than 55 years of age, [5, 6] and in certain populations, including blacks and Japanese [3, 7].
Hypertension is the most important risk factor for spontaneous intracerebral hemorrhage.[8] Intracerebral hemorrhage commonly affects cerebral lobes, basal ganglia, the thalamus, the brain stem (predominantly the pons), and the cerebellum [9] as a result of ruptured vessels. Extension into the ventricles occurs in association with deep, large hematomas.The classic presentation of intracerebral hemorrhage is sudden onset of a focal neurological deficit that progress over minutes to hours with accompanying headache, nausea, vomiting, decreased consciousness and elevated blood pressure. Computed tomography is the key part of the initial diagnostic evaluation. First, it clearly differentiates hemorrhage from ischemic strokes. In addition computed tomography demonstrates the side and location of the hemorrhage and may reveal structural abnormality as well as structural complications such as herniation, intraventricular hemorrhage or hydrocephalus.[10] Initial management should first be directed toward the basics of air way, breathing, and circulation, and detection of focal neurologicaldeficits [10].
Other supportive medical care includes reduction of the intracranial pressure by diuretics (Mannitol 20% and furosemide, use of anticonvulsants (Diazepam, Midazolam or Phenobarbital) and control of hyperthermia (In order to decrease the neural metabolism) achieved by: external refrigeration, cold saline, sedation, and mechanical ventilation [11]. The optimal level of patients’ blood pressure should be based on individual factors such as chronic hypertension, elevated intracranial pressure, age, presumed cause of hemorrhage, and interval since onset [12]. In general recommendation for treatment of elevated blood pressure in patients with ICH are more aggressive than those for patients with ischemic stroke [19]. Antihypertensive agents recommended for treatment of blood pressure in ICH: nitroprusside, labetalol, enalapril, esmolol, hydralazine [10]. In one fourth of patients with intracerebral hemorrhage who are initially alert, a deterioration in the level of consciousness occurs within first 24 hours after onset of hemorrhage [13,14]. Expansion of the hematoma is the most common cause of underlying neurologic deterioration within the first three hours the onset of hemorrhage. Worsening cerebral edema is also implicated in neurologic deterioration that occurs within 24-48 hours after the onset of hemorrhage [14].
This cross sectional, observational, prospective study was carried out in Medicine department of Khulna Medical College Hospital from November, 2020 to April 2021. Total 50 cases of spontaneous ICH were selected. Diagnosis was made by CT scan of brain. Data were processed and analyzed using SPSS (Statistical Package for Social Science) 17.0.
Inclusion criteria:
Exclusion criteria:
Table-1 showing age distribution of patients with spontaneous ICH. It was most common in between 41-70 years. Their age frequency 14 (28%) were in 41-50 years, 15 (30%) were in 51- 60 years, 12 (24%) were in 61-70 years, 5 (10%) were in 71- 80 years, 4 (8%) were more than 81 years old.
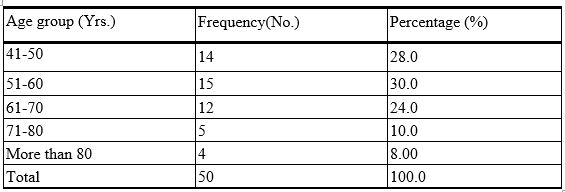
Figure-1 showing spontaneous ICH is more common in male than female. Among 50 cases, 64%(32) were male whereas 36%(18) were female.
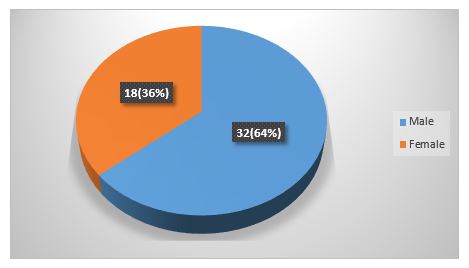
Figure-2 demonstrates that spontaneous intracerebral hemorrhage was found in farmer/ day labor 26% (13), businessman 24% (12), housemaker 36% (18), and service holder14% (7).
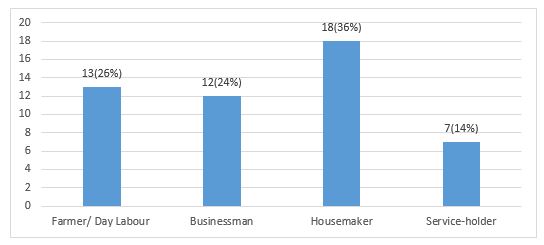
Table-2 demonstrates that spontaneous ICH is common in poor and middle class family. Among the patients, poor (monthly income less than 10000 taka) is 40% (20), middle class (monthly income 10000-50000 taka) is 58% (29), high class((monthly income more than 50000 taka)is 2% (1).
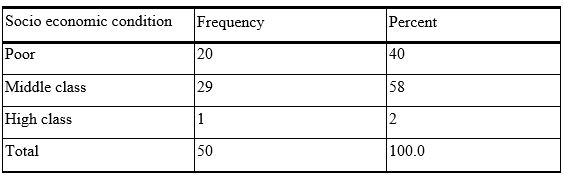
Figure-3 represents spontaneous ICH more common in smoker. Among 50 cases male smoker 25 (50%) and female 1 (2%) and nonsmoker male 7 (14%) and female 17 (34%).
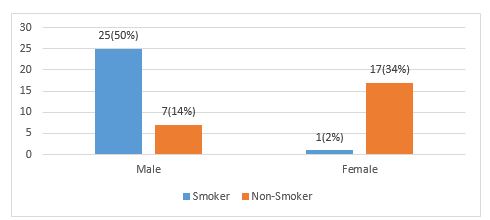
Figure-4 showing many patients with spontaneous ICH presented with headache. Headache was present in 56% (28) and was absent in 44% (22) patients.
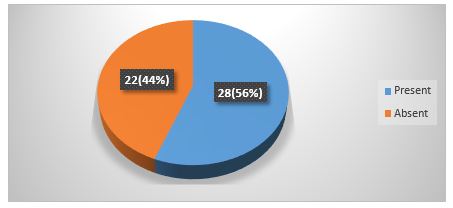
Figure-5 showing many patients with spontaneous ICH presented with vomiting. Vomiting was present in 54% (27) and was absent in 46% (23) patients.
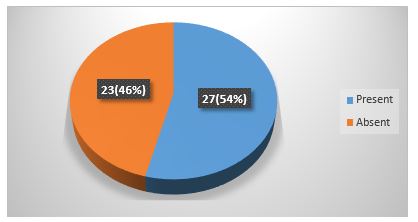
Figure-6 showing many patients with spontaneous ICH presented with seizure. Seizure was present in 8 (16%) and was absent in 42 (84%) patients.

Table-3 shows GCS Score distribution. GCS Score was 8 or less in 42% (21), 9 or more in 58% (29) cases.
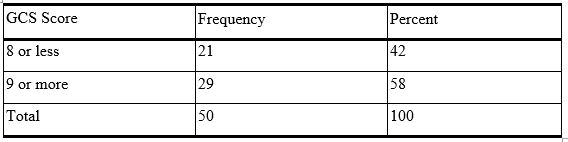
*GCS-Glasgow coma scale
Table -4 presents that number of disorientated patients with spontaneous intracerebral hemorrhage. Among the cases orientation absent in 76% (38) and orientation present in 24% (12).
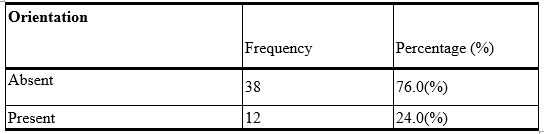
Table-5 showing that sensory deficit was present in 46% (23) and absent in 54% (27) patients.
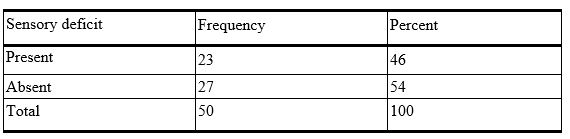
Table-6 presents diabetes mellitus among 50 cases. Diabetes mellitus was present in 22% (11), absent in 78% (39) cases.
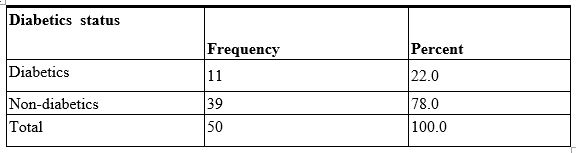
Table-7 presents blood pressure distribution: SBP: Less than 140/DBP: Less than 90 (mm Hg) in 24%(12),SBP:140-159/DBP:90-99 (mm Hg) in 10%(5),SBP:160-179/DBP:100-109 (mm Hg) in 22%(11),SBP:180 or more/DBP:110 or more (mm Hg) in44%(22)

*SBP- Systolic blood pressure.
^DBP- Diastolic blood pressure.
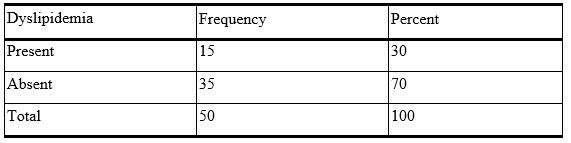
Table-8 showing dyslipidemia was present in 30% (15) & absent in 70% (35) patients.
Spontaneous ICH is a third leading cause of death worldwide. It also common in developing country like Bangladesh.In our study, age of the patients with spontaneous ICH was above 40 years. It most commonly occurred in 40-70 years age group with 82% (41) and number of patients above 70 years of age with spontaneous ICH was 18% (9). Doctor M et al (2013) [15] in their study found the maximum number of cases i.e. 38 (76%) were between the age groups 45 to 74 years and age ranged from 35 to 74 years. A.k.Thacker et al reported, out of 50 cases of ICH, 39 (78%) were in the age group of 41-70 years and age ranged from 16-85 years. KafleR [16], Age distribution of patient’s presentation with spontaneous intracerebral bleeding was as follows. Less than 20 years of age: 1 patient. 20-29: 1 patient .30-39: 2 patients. 40-49: 11 patients. 50-59:19 patients. 60-69: 29 patients. 70-79: 20 patients. Above 80 years: 17 patients. In study by Bhatia R et al (2013) [17]. The mean age was 57.32 ± 12.84 years and 140 (65.4%) were males. Hsiang et al. (2009) [18] in a study of 60 consecutive Chinese patients showed that unlike the western studies, the majority of their patients were about a decade younger. Ong and Raymond, (2002) [19] in a study found the median age was 65 years. Juvela et al (1995) [20] conducted a prospective study of 156 consecutive patient with an age range of 16 to 60 years. Study by Adnan et al. (1997) [21] showed that compared with woman, men had a younger age of onset. All studies have shown a steep rise in incidence with increasing age.
In this study, spontaneous ICH is more common in male 64% (32) than female 36% (18). In study by Ong and Raymond, (2002) [19] showed that male to female ratio was 1:0.77. Adnan et al. (1997) [21] in a study showed that compared with woman, men had a younger age of onset (54 versus 60 years; p<0>
In the study regarding the occupation of the patients having Spontaneous ICH, farmer/day labour was 26% (13), businessman was 24% (12), and house- wife was 36% (18), and service holder was14% (7). Giulia et al. (2009) [23] found men with low SEP(socioeconomic position) with an ischemic event were more likely to be hospitalized for a new stroke than men with high SEP. Women with low SEP with hemorrhagic stroke were more likely to be hospitalized for cardiovascular disease compared with women with high SEP.
In our study, we found that spontaneous ICH was common in poor and middle class family. Among the patients, poor was 40% (20), solvent 58% (29), very good 2% (1). In a study by Giulia et al. (2009) [22] showed that stroke incidence strongly differs between socioeconomic groups reflecting a heterogeneous distribution of lifestyle and clinical risk factors. Strategies for primary prevention should target less affluent people.
In this study, we found that spontaneous ICH was more common in smoker. Among 50 cases, male smoker were 25(50%) and female 1(2%) and nonsmoker male was 7(14%) and female was17 (34%).Kafle R D [16], showed that 21 percent of patients were smoker. In study by Zaharia et al (2005) [11] found that, cigarette smoker (13.1%). Doctor et al (2013) [15], showed in their study, history of smoking was present in 24 cases (48%), all were male and 17 patients (34%) were currently smoking. Craig S. Anderson reported history of smoking in 29% of patients and ex-smoking in 19% of patients out of 60
Spontaneous ICH is a major cause of morbidity and mortality among stroke patients. Hypertension is the most common cause of spontaneous ICH;others are smoking, dyslipidemia, diabetes mellitus and family history of stroke. Mainstay of treatment is supportive, including airway maintenance, diabetes control, blood pressure control, treatment and prophylaxis of convulsion, temperature control, nutritional support, careful fluid therapy and rehabilitation is also needed for improved mortality and morbidity.
Limitation of Study: The present study did not represent the actual scenario of spontaneous ICH in Bangladesh because the study was conducted in one tertiary level hospital (Khulna Medical College and Hospital (KMCH). Sample size and duration of the study was short. Actual measurement of intracranial pressure was not possible. Advanced investigation facilities (Cerebral angiogram, MRI of brain) were limited. There was no advanced life support available.
There were no conflicts of interests
Ethical Clearance Appropriately taken
Funding Self-funded
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
