
Case Report | DOI: https://doi.org/10.31579/2690-4861/291
1 Department of High-risk pregnancy and Perinatology, Kimshealth, Trivandrum. India.
2 Department of Interventional Radiology, Kimshealth, Trivandrum.India.
3 Department of Obstetrics and Gynecology, Kimshealth, Trivandrum. India.
*Corresponding Author: Nina Navakumar, Department of High-risk pregnancy and Perinatology, Kimshealth, Trivandrum. India.
Citation: Navakumar N., Manish K. Yadav, Girija G., P K Syamaladevi, Vidyalekshmy R., (2023), 2 Case Reports of Uterine Artery Pseudoaneurysm Diagnosed in Pregnancy and Postpartum – Successfully Embolised. International Journal of Clinical Case Reports and Reviews. 13(1); DOI: 10.31579/2690-4861/291
Copyright: © 2023 Nina Navakumar, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 January 2023 | Accepted: 20 January 2023 | Published: 31 January 2023
Keywords: uterine artery; pseudoaneurysm; acute abdomen; hydronephrosis; postpartum hemorrhage; uterine artery embolization
Pseudoaneurysm is an extraluminal collection of blood with a turbulent flow that communicates with flowing arterial blood through a defect in the arterial wall. Uterine artery pseudoaneurysm (UAP) is considered a rare case that occurs in 2–3/1,000 deliveries. Here we discuss 2 cases – first case is UAP diagnosed antenatally in a woman with acute abdomen and hydronephrosis, second case presented as secondary delayed postpartum haemorrhage. Sonography revealed UAP, and the diagnosis was confirmed by angiography. The defects were. treated by uterine artery embolization. UAE is to be considered a life-saving procedure obviating need for hysterectomy and improves maternal outcome.
A pseudoaneurysm is defined as an extraluminal collection of blood with a turbulent flow that communicates with flowing arterial blood through a defect in the arterial wall.1 Some authors have reported that a uterine artery pseudoaneurysm (UAP) occurs in 2–3/1,000 deliveries [2,3]. After hematoma formation, there is central liquefaction that leaves a cavity with turbulent blood flow, as a result of persistent communication between the parent artery and the hematoma. The absence of a 3-layer arterial wall lining the pseudoaneurysm differentiates it from a true aneurysm, which is less common than a pseudoaneurysm [4]. Pseudoaneurysm of the uterine artery is an uncommon cause of delayed postpartum hemorrhage following caesarean or vaginal delivery and is potentially life threatening. Typically, the lesions are discovered because the patients have symptoms related to delayed rupture of the pseudoaneurysm, causing hemorrhage [5]. A pseudoaneurysm may be asymptomatic, may thrombose, or may lead to distal painful embolization. The risk of rupture is proportional to the size and intramural pressure. Diagnosis is usually based on both Doppler sonography and arteriography [6]. Transcatheter uterine artery embolization (UAE) has emerged as a highly effective technique for controlling obstetric and gynaecologic hemorrhage, including that from pseudoaneurysms. Ciebiera et al suggested that the UAP should be adequately treated because it is a potentially life-threatening lesion [7].
We report 2 cases of uterine artery pseudoaneurysm
1-Acute abdomen and right hydronephrosis antenatally – right uterine artery pseudoaneurysm
36-year-old multigravida, previous caesarean section referred with complaints of lower abdominal pain and right hydronephrosis at 19 weeks of gestation; on ultrasound evaluation was found to have right uterine artery pseudo aneurysm measuring 5.4x5 6 cm with internal Doppler flow which was confirmed with MRI pelvis and abdomen. She was hemodynamically stable with non tender abdomen. She underwent right uterine artery pseudo aneurysm endovascular embolisation with nested fibre coils. Post procedure she had increasing abdominal distension with haemoglobin drop of 2 gpercentage and large right sided pelvic hematoma (Figure 2). She was managed conservatively with blood transfusion and supportive care. She was followed up with serial growth scans and screened for hypertension. She delivered a live term baby of weight 2.8 kg by caesarean section and had uneventful post-operative period

Figure 2: Post procedure she had increasing abdominal distension with haemoglobin drop of 2 g% and large right sided pelvic hematoma
2 - Massive secondary PPH - left uterine artery pseudoaneurysm
25-year-old a woman with previous LSCS and dilatation and curettage presented 39 days post-cesarean with massive secondary PPH. She had severe anemia (3.8gpercentage) and received multiple blood transfusion and supportive care. On further evaluation she was diagnosed with left uterine artery pseudoaneurysm by colour Doppler ultrasound which was confirmed with CT angiography of pelvis and abdomen with pathology identified in its intramural branch (Figure 1). She was managed with left uterine artery embolization by coils obviating need for hysterectomy and laparotomy.
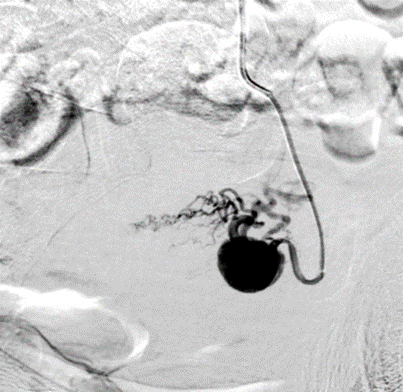
Figure 1: Pseudoaneurysm of left uterine artery – CT angiogram pelvis image – angiographic contrast image
In 1979, Brown et al., reported the first case of selective arterial embolization used successfully to treat an extrauterine pelvic hematoma after three failed surgical attempts to control the bleeding.8 Here we describe 2 cases which shows the role of interventional radiology in the form of uterine artery embolization for obstetric and medical / surgical emergency in pregnancy and postpartum obviating need for exploratory laparotomy, hysterectomy, ICU stay, increased hospital stay, massive blood transfusion and its complications. Angiographic embolization has the advantages of decreased morbidity, ability to localize the bleeding site and provide a more distal occlusion than surgical ligation, and preservation of future fertility compared to hysterectomy. Our both cases though in pregnancy or postpartum presented in acute condition and warranted immediate management and tertiary level care requiring trained personnel and facilities. UAP may be asymptomatic but usually presents with secondary postpartum hemorrhage (PPH) or delayed vaginal bleeding. In our first case we describe uterine artery pseudoaneurysm presented as unilateral hydronephrosis and acute abdomen, which shows its varied presentation in pregnancy and need high index of clinical suspicion. When the more common causes of secondary postpartum haemorrhage have been excluded, pelvic angiography may be performed to rule out pseudoaneurysm. From our second case we infer that in the pregnancy after previous surgical procedures to the uterus, uterine artery pseudoaneurysm should be considered in the differential diagnosis of symptomatic hydronephrosis.
UAP is due to blood flowing into periarterial tissues after a wall defect. This creates a perfused sac, which communicates with the artery lumen. If the blood is fully covered by the adventitia or the surrounding tissues, a pseudoaneurysm is formed. Blood fills the sac during systole and flows away during diastole. Dar et al stated that UAP usually develops after invasive procedures such as cesarean section, myomectomy, dilatation, and curettage [9]. Regarding the diagnosis of UAP, Chaudhry and Chaudhry reported that uterine artery aneurysm should be among the differential diagnoses that are considered in pregnant women who present with pelvic and vaginal masses, vague bladder symptoms, or radiating pelvic pain. Some authors have reported that a UAP usually presents with vaginal bleeding, and its diagnosis includes a gray-scale U/S and color Doppler [11]. They added that, on duplex color Doppler, pseudoaneurysms appear as a saccular arterial out pouch or an abnormal dilatation of an artery, with surrounding hematoma. The efficacy and safety of selective arterial embolization of uterine arteries was evaluated by Pelage et al., in women with delayed secondary postpartum hemorrhage. In their series of 14 women, pseudoaneurysms of the uterine artery were found in 2 women [12]. Immediate resolution of external bleeding was observed after embolization. In this series, no complications related to this invasive treatment were found. Other authors have described complications, including muscle pain and bladder necrosis [13].
In a small series of women,who underwent embolotherapy for obstetric hemorrhage, all 3 women who attempted conception after embolization were successful. Of the 3 women, 2 underwent bilateral uterine artery embolization [14]. Karmous et al have suggested that pseudoaneurysm has a characteristic sonographic appearance consisting of a pulsating anechoic or hypoechoic well-defined cystic structure with or without associated pelvic hematoma or free fluid. In the neck of the pseudoaneurysm, the “yin-yang” pattern may be potentially identified on duplex Doppler because the arterial blood flows like a jet (forward flow) into the aneurysm cavity during systole, then reverses (backward flow) into the original artery during diastole. Ciebiera et al stated that the diagnosis of UAP can be obtained by color and spectral Doppler sonography and confirmed by angiography. Karmous et al reported two cases of UAP; they used color Doppler in their diagnosis and conducted angiography as part of the treatment procedure for the first case. They treated the second case with based only on color Doppler imaging findings. In the current case study, standard procedures were followed for diagnosis and treatment. Also, the color Doppler findings were confirmed with angiography. Yeniel et al15 reported a case of a 28-year-old patient who had a UAP. In this case, they failed to detect the UAP, which may have been due to depending only on gray-scale U/S and Doppler as their diagnostic method. In this case, the UAP was detected after an emergency laparotomy. A catheter was inserted through the right femoral artery, and the angiogram images showed a focal dilatation of the right uterine artery. The findings showed a typical feature of a UAP Digiacinto et al 16 concluded that follow-up CT is used to confirm the diagnosis identified on the sonogram. They stated that while CT is useful in identifying and diagnosing UAP, percutaneous angiography is considered the gold standard to diagnose a pseudoaneurysm and plays a role in the treatment as well. The differential diagnosis of UAPs includes acquired and congenital arteriovenous malformations, consisting of a web of mixed arteries and veins.
Regarding the treatment of UAP, there are different options in clinical applications. Some authors have shown that clinical treatments of UAP include transcatheter arterial embolization, uterine artery ligation,17 ultrasound guided thrombin injection, and hysterectomy. Kwon et al 18 mentioned that uterine artery embolization (UAE) using N-butyl-2-cyanoacrylate is safe and effective in patients with PPH who show evidence of extravasation or pseudoaneurysm. Takahashi et al 19 studied three cases of UAP resulting from vacuum delivery, vacuum delivery with placental removal, and dilatation. They made the diagnosis for these three cases using color Doppler and found that all three patients recovered spontaneously, without UAE. The current case study disagrees with this hypothesis because the aforementioned case series indicated that all three patients experienced slight bleeding. They also did not confirm the case series diagnoses with angiography. Gurses et al studied a case of a 21-year-old with UAP, which was easily diagnosed with duplex Doppler and treated with embolization. This conclusion supports the current case study report. Soyer et al provided a similar conclusion; they reviewed seven case studies and showed that transcatheter arterial embolization is an effective and secure technique for the treatment of severe postpartum hemorrhage due to uterine or vaginal artery pseudoaneurysm.
Uterine artery pseudoaneurysm should be kept as one of the differential diagnoses when a woman presents with acute abdomen, obstetric hemorrhage or with pressure symptoms and timely diagnosis with colour Doppler ultrasound and transcatheter arterial embolization to be considered in a tertiary care centre. Uterine artery embolization appears to be a lifesaving safe and effective method to treat pseudoaneurysm during pregnancy and postpartum without compromising maternal and fetal optimal outcome.
Conflict of Interest: No
Funding: No funding
Ethical Study: This study has been conducted according to the ethical standards of our institution.
Authors Contribution: All authors equally contributed to this study.
Consent: Informed consent has been taken from the patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
