
Case Report | DOI: https://doi.org/10.31579/2692-9406/054
*Corresponding Author: Aiman Rahmani, Pediatric Intensive Care Unit, Department of Critical Care, Tawam Hospital, Al-Ain-Abu Dhabi, UAE.
Citation: Nidal O. Al-Hashaykeh, Mona M. Faramawy, Khaled H. Atwa, A Rahmani. (2021) Effective, timely use of Intravenous Immunoglobulins for management of Pediatric multisystem inflammatory syndrome associated with COVID-19 (PMIS-COV19) in a 9 years old boy: Case report. Biomedical Research and Clinical Reviews. 3(5); DOI: 10.31579/2692-9406/054
Copyright: © 2021 Aiman Rahmani, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 February 2021 | Accepted: 26 March 2021 | Published: 29 March 2021
Keywords: intravenous immunoglobulins; pediatric multisystem; inflammatory syndrome; COVID-19
Coronavirus disease 2019 (COVID-19) is arguably the most socially and economically disruptive pandemic since the 1918 influenza pandemic. Although pediatric COVID-19 shares features with the adult disease, there are several differences. Children produce virus in amounts at least equal to adults, if not higher and can transmit the virus just as adults can. School-aged children are generally less severely affected than infants or adults, but some children without significant underlying disease become ill or die in a disease process analogous to the one most commonly seen in adults as severe pulmonary disease and respiratory failure. Children and adults appear to have different humoral immune responses to COVID-19.
Coronavirus disease 2019 (COVID-19) is arguably the most socially and economically disruptive pandemic since the 1918 influenza pandemic. Although pediatric COVID-19 shares features with the adult disease, there are several differences. Children produce virus in amounts at least equal to adults, if not higher[1] and can transmit the virus just as adults can [2]. School-aged children are generally less severely affected than infants or adults, but some children without significant underlying disease become ill or die in a disease process analogous to the one most commonly seen in adults as severe pulmonary disease and respiratory failure [3–6]. Children and adults appear to have different humoral immune responses to COVID-19 [7, 8]. A Pediatric multisystem inflammatory syndrometemporally associated with SARS-CoV-2 infection (PMIS-COV19)was first recognized in the U.K and was noted to share many signs and symptoms of Kawasaki disease (KD), Kawasaki disease shock syndrome (KDSS) and toxic shock syndrome (TSS) [9]. PMIS-COV19is a dangerous systemic infection characterized by extreme inflammation, fever, abdominal symptoms, conjunctivitis, and rash. Children will typically show signs and symptoms of PMIS-COV19three to four weeks after COVID-19 infection. Many will progress rapidly into shock and cardiorespiratory failure [10]. In this case report, we are describing a 9 years old boy, who presented to our pediatrics critical care unit 4 weeks after being reported positive for SARS-CoV-2 infection. His symptoms were matching the literature description of the newly reported PMIS-COV19and was managed accordingly. The key element in our approach was the timely and early administration of IVIG which had a significant positive impact on his clinical course and outcome.
Case Report:
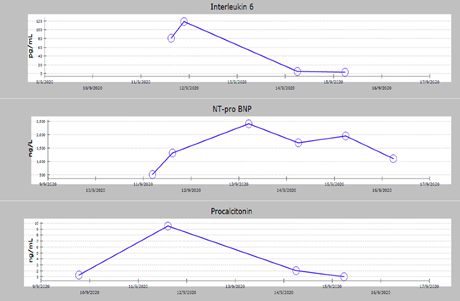
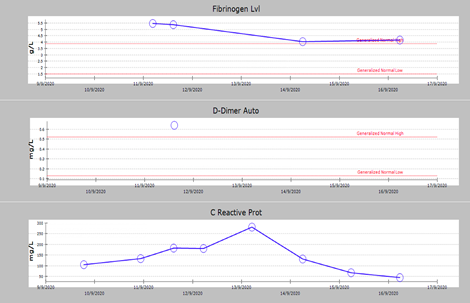
A 9 years old boy previously healthy, had a positive a SARS-CoV-2 infection confirmed by PCR testing 4 weeks before presenting to our hospital. The positive results were then followed by 2 negative SARS-CoV-2 PCR results 24 hours apart. The patient presented to our ED with persistent high grade fever (40ºC) for 5 days, tachycardia, sore throat, generalized macular skin rash, bilateral non-purulent conjunctivitis, abdominal pain, nausea and vomiting for 2 days duration. His clinical presentation was matching the literature description of PMIS-COV19 with no signs of respiratory distress. Initial CT abdomen was consistent with early bowel inflammatory process at ileocecal junction with no lymphadenopathy. Subsequent workup for PMIS-COV19 results revealed lymphopenia, mild hyponatremia, raised fibrinogen, high levels of NT-pro BNP, Ferritin (< 500), LDH and inflammatory markers including CRP, procalcitonin, ESR, triglycerides and IL-6. Blood serology for SARS-CoV-2 antibodies were detected. Viral serology blood PCR for EBV, CMV, adenovirus and enteroviruses were not detected. Cardiac ECHO reported as; trace MR, otherwise normal cardiac structures and functions, normal coronary artery dimensions with normal z- score. At this point the clinical and para clinical testing results were consistent with PMIS-COV19 based on the flowing criteria:
- Persistent fever more than (39ºC)
- Sick looking, lethargy.
- Skin rash.
- Non-purulent conjunctivitis.
- Abdominal symptoms.
- Tachycardia with or without shock.
- Evidence of SARS-CoV-2 antibodies positive.
- Laboratory: elevated inflammatory markers.
The patient was started immediately on IVIG as 2 gm/kg followed by methylprednisolone and aspirin. Antibiotics were commenced initially and stopped after all the bacterial cultures were reported no growth. His fever, skin rash, and conjunctivitis dramatically subsided after completing the IVIG. His abdominal symptoms improved and resolved within 48 hours coinciding with normalization of his blood workup parameters. During his stay he did not require any respiratory or inotropic support. Patient was discharged home on oral steroids and aspirin after10 days of hospitalization without any complication, with follow up in the pediatric cardiology and infectious disease clinics.

Discussion
Since the first reports of an unusual inflammatory illness in children that emerged in the months following the onset of COVID-19, there have been additional reports from many countries of children with fever and inflammation, for which no cause could be identified. These reports were first in health alerts and web exchanges between professional groups and then as case reports and small case series in rapid publications [11-13]. As these cases have emerged in temporal association with the pandemic, a link with SARS-CoV-2 is likely [9]. Patients with PMIS-COV19 predominantly had fever with gastrointestinal, cardiovascular and mucocutaneous manifestations, which were consistent across studies despite the different inclusion criteria. Respiratory manifestations, which are predominant manifestations in adults with COVID-19 infection, were described in a minority of pediatric patients with PMIS-COV19. All studies reported highly elevated levels of inflammatory markers suggesting that hyper inflammatory state is a primary hallmark of PMIS-COV19 [14]. Early reports support the use of IVIG in the treatment of PMIS-COV19 patients [11, 15, 16]. PMIS-COV19 cases exhibit greater prevalence of multisystem involvement, notably cardiac abnormalities such as myocarditis and shock [17]. In all reported studies so far, the proportion of patients with positive SARS-CoV-2 serology testing was substantially greater than those with positive SARS-CoV-2 RT-PCR tests. These findings as well as increased inflammatory markers are consistent with the hypothesis that PMIS-COV19 results from a post-infectious inflammatory process [17,18,19]. Multiple reports describe a 4 to 6 weeks delay between the proliferation of local COVID-19 cases and the surge in PMIS-COV19 cases [18,20,21] whereas Feldstein et al described a median of 22 days between onset of COVID-19 symptoms and PMIS-COV19 hospitalization [14,20].
Conclusion
PMIS-COV19 is a new pediatric disease that is most likely linked to SARS-CoV-2 infection. Although being relatively uncommon, it can lead to serious complications or life threatening illness.
In this case report, we aimed to emphasize the importance of timely and early initiation of appropriate management with specific attention to IVIG to improve outcomes. Educating the public about the symptoms of PMIS-COV19 and encouraging them to seek medical advice as early as in doubt, especially while we are still living in the era of active pandemic, is of great importance. Future studies and case series can shed additional light on PMIS-COV19 to improve prospects for prevention and treatment of this severe pediatric condition.
Abbreviations
COVID-19: coronavirus disease 2019
CRP: C-reactive protein
ED: Emergency department
IL-6 : Interleukin-6
IVIG : Intervenus Immunoglobuline
MR; Mitral regurgitation
NT-pro BNP: Natriuretic Peptide
PCR: (reverse-transcription polymerase chain reaction)
PMIS-C19: Pediatric multisystem inflammatory syndrome post Covid19
SARS-Co-V-2: severe acute respiratory syndrome coronavirus 2
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
