
Case Report | DOI: https://doi.org/10.31579/2690-4861/087
*Corresponding Author: Dr. Sandhya Govindarajan, Speciality Registrar, Department of Paediatrics and Neonates, North Manchester General Hospital, M8 5RB.
Citation: S Govindarajan, S Chakrabarti. (2021) Subcutaneous fat necrosis (SCFN) secondary to therapeutic hypothermia with persistent leucocytosis in a neonate. International Journal of Clinical Case Reports and Reviews. 6(2); DOI:10.31579/2690-4861/087
Copyright: © 2021 Sandhya Govindarajan, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 October 2020 | Accepted: 30 December 2020 | Published: 08 January 2021
Keywords: subcutaneous fat necrosis; therapeutic hypothermia; leucocytosis
We report a term male neonate, born to consanguineous parents through a difficult labour who needed resuscitation at birth, followed by ventilation for respiratory distress. In view of suspected Hypoxic Ischemic Injury, he was started on whole body cooling for 72 hours. He was treated as suspected sepsis with 5 days of intravenous antibiotics. On day 6, he was noted to have hard, painless skin nodules of his back and left arm which was clinically diagnosed as subcutaneous fat necrosis. His serum calcium and phosphate levels remained normal throughout hospital stay. His full blood counts and bone profile were monitored regularly. During follow-up at 6 weeks, his white cell counts continued to be high with 69% lymphocytes. To our knowledge, this is the first case of SCFN of a neonate associated with persistent leucocytosis. Haematological and metabolic complications should be closely monitored in a neonate with subcutaneous fat necrosis.
1. Respiratory support – Opti flow, Ventilation and low flow oxygen.
2. Therapeutic hypothermia.
3. Intra venous antibiotics for suspected sepsis for a total 5 days.
4. Physiotherapy for Erb’s palsy (Right side).
5. Phototherapy for jaundice.
6. IV fluids and feed establishment.
Outcome and Follow-Up
Enteral feeds were started by day 5 of life and fully established by day 7 of life. He was fully breast fed and discharged on day 17 of life with a multidisciplinary follow up with neurosurgical, endocrine, physiotherapy, urology, paediatrics and dermatology teams. Follow up by telephonic consultation (in view of COVID-19 pandemic) at 4 months of age revealed that the hard nodules noted during the neonatal period had almost resolved. He continues to remain under follow up with paediatric team.
Therapeutic Hypothermia (TH) or whole-body cooling remains a standard form of therapy for neuroprotection in term infants with hypoxic ischemic brain injury. Therapeutic hypothermia [1], birth asphyxia [1], large for gestational age [2,3], hypoglycaemia[1], perinatal distress [3], difficult/traumatic labour[4] and meconium during labour[5],maternal cocaine/cigarette use[6],preeclampsia[6] and maternal calcium channel blocker use[6] have all been reported in literature as a cause of subcutaneous fat necrosis (SCFN) in the first month of life. SCFN of a neonate has been associated with various haematological and metabolic complications. Although physiological leucocytosis is a common occurrence in neonatal period due to surge in cytokine secretion (Granulocyte Colony Stimulating Factor [7] in the immediate postpartum period, the levels normalise after 1 month of life. The reference leucocyte count from 1-23 months ranges from 6.0-14.0 x 109 cells/mm3 [8]. In our patient, the leucocytes count continued to remain high (figure 3) with higher percentage of lymphocytes (69%) after 6 weeks of life without any intercurrent illness.
We present a term male neonate, second born, by spontaneous vaginal delivery with a birth weight of 4310g to consanguineous parents. Baby’s mother had gestational diabetes was on metformin, gestational hypertension not on any medications, hypothyroidism on levothyroxine and anaemia on iron and folic acid. Antenatal screening including blood tests such as Rubella, VDRL, Hepatitis B antigen, Hepatitis C antigen, HIV, syphilis, hemoglobinopathy screen were negative. Antenatal ultrasounds showed normal anomaly scan and growth >95th centile in the growth scan. Mother was admitted to labour ward at 39 weeks+ 2 days for induction of labour in view of baby being large for gestational age. Artificial rupture of membranes performed and clear liquor noted. 5 hours after induction baby’s head was delivered. Baby was noted to have shoulder dystocia. McRoberts’s manoeuvre and suprapubic pressure applied and posterior arm delivered first followed by rest of the body. Baby needed resuscitation at birth with intermittent positive pressure ventilation. APGAR scores were 7 at 5 minutes and 8 at 10 minutes of age. Cord gases showed an arterial pH of 7.06 and Base excess of -6.50. Baby developed mild respiratory distress and blood gas showed an initial pH of 7.22 (reference 7.35 – 7.45), pCo2 of 6.90 (reference 4.6-6.4kPa), base deficit of -6.4 (reference -2mmol/L to +3mmol/L) suggestive of mild respiratory acidosis. Hence the baby was admitted to the neonatal unit and started on Opti flow at 1 hour of age. He continued to have respiratory distress and desaturations and blood gas at 2 hours of age showed worsening of respiratory acidosis (partially compensated) with pH 6.92 (reference 7.35 – 7.45,pCo2 of 14.70(reference 4.6-6.4kPa), HCO3 15.4 (reference 21-28mmol/L), base deficit of – 10.0 (reference -2mmol/L to +3mmol/L) and lactate of 6.40 (</=2 mmol). Hence, he was intubated and started on Cerebral function Analysing Monitor (CFAM). A decision to start baby on therapeutic hypothermia was made in view of suspected Hypoxic Ischemic Injury (HIE) and he was transferred to a higher centre. Blood tests on day 2 of life revealed a white cell count of 23.7 x 109 (reference 9.1-34.0 x 109 cells/mm3[8]) and a platelet count of 126 x 109 /L (reference 84-478 x 109/L[8]) and a mildly elevated C – reactive protein levels of 10.9mg/L (reference 0 -10 mg/L). He was treated with intravenous (IV) Benzyl Penicillin and Gentamycin for suspected sepsis. Cranial ultrasound done on day 2 of life was normal. He received therapeutic hypothermia for 72 hours. He was kept nil by mouth during therapeutic hypothermia and was on IV fluids with fluid restriction. He was extubated on day 2 of life and was on low flow oxygen for 4 days. IV antibiotics were stopped on day 5 since his blood cultures were sterile. He was self-ventilating in air from day 6 of life. On routine examination on day 6 of life, he was found to have small, painless, hard nodules of his back and left arm which was found to be subcutaneous fat necrosis secondary to therapeutic hypothermia (figure 1). No evidence of clinical or electrical seizure activity noted during hospital stay. Once fully rewarmed, he was started on enteral feeds and was fully fed by 7 days of life. He was noted to have asymmetrical microcephaly with head circumference just below second centile. Toxoplasma, Rubella, Cytomegalovirus and Herpes simplex antibodies (TORCH screen) were negative. MRI head done on 1 month of life showed no evidence of HIE changes but a small subdural hematoma on the left side. There were no neurosurgical concerns over the hematoma and was decided to follow up in the outpatient clinic. He was also noted to have right sided Erb’s palsy secondary to shoulder dystocia. Ultrasound right shoulder and X ray of the right shoulder were found to be normal and was started on physiotherapy. He had a brief period of physiological neonatal jaundice and was treated with phototherapy. Direct agglutinin test was negative. On further examination, he was noted to have bilateral undescended testes for which ultrasound pelvis was done which showed possible pelvic testis on the right side. Left side testis was not identified in the scan. He had an XY karyotype with low testosterone and normal 17 -hydroxy progesterone levels. He remained in the neonatal unit for 20 days and was discharged with follow up.

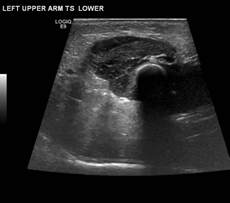
Ultrasound of the skin nodule showed diffuse edema, no evidence of collection and normal appearance of underlying muscles (figure 2). His full blood counts showed a white cell count of 23.7 x 109 (reference 9.1-34.0 x 109 cells/mm3 [8]), platelets of 126 x 109 /L (reference 84-478 x 109/L [8]) on day 2 of life. His platelets reached a nadir of 123 x 109 (reference 84-478 x 109/L [8]) on day 5 of life. Although his platelets count increased to 166 by 10 days (reference 150-400 x 109/L [8]), his white cell count continued to remain on the higher range of normal limit with high percentage of lymphocytes (>50%), even after completion of 5 days antibiotics for suspected sepsis. Repeat white cell count at 6 weeks of age done as a routine was found to be high 19.4 x 109 cells/mm3 (reference 6.0 – 14.0 x 109 cells/mm3[8]) (figure 3) with 69% (25%-33%) lymphocytes. His serum calcium levels were found to be 2.63 mmol/L (reference 2.20-2.70mmol/L) after 1 week of life and was never found to be >3mmol/L (hypercalcaemic range). His serum phosphate levels were normal throughout. His Vitamin D and parathyroid levels were not performed due to normal range of serum calcium and phosphorus. His full blood counts and bone profile were monitored serially in view of subcutaneous fat necrosis. His genetic studies were found to be normal.

SCFN of a neonate is an uncommon, transient and spontaneously resolving panniculitis, usually affecting term neonates with perinatal complications [9] first described in 1926. The pathogenesis of SCFN remains unresolved. It has been postulated that any perinatal/neonatal distress may interfere with normal blood supply to the fat tissue, creating an environment of hypoxia and hypothermia, which is believed to result in inflammation and necrosis. [6] Also, the hypodermis of the newborn has a higher proportion of saturated fats (i.e., stearic and palmitic acids), which have a higher melting point (64 °C) making them more likely to crystallize under colder conditions [10]. Evidences also suggest that there might be pathophysiological connection between brown adipose tissue and SCFN in neonates [11]. Perinatal stress including difficult labour, large for gestational age and therapeutic hypothermia are all considered to be risk factors for development of SCFN in our neonate.
Metabolic consequences like moderate to severe hypercalcemia [1], metastatic calcifications (disseminated sub cutaneous calcifications, nephrocalcinosis and myocardial calcifications) [6], hypocalcaemia [12], hypoglycaemia [13], hyperkalaemia [14] hypertriglyceridemia [1,10] have been reported to be associated with SCFN. Although the pathophysiology of hypercalcemia in SCFN remains unclear, a widely accepted theory proposes that the elevated 1, 25-Hydroxyvitamin D3 secreted from the granulomas of the skin lesions can stimulate intestinal calcium uptake [6] and decreased clearance of calcium by the kidneys [3] results in hypercalcemia. It is postulated that perinatal asphyxia causes transient functional hypoparathyroidism resulting in hypocalcaemia in new-borns with SCFN [12]. It is suggested that neonates with SCFN should have serial serum calcium determinations for up to 6 months after the appearance of skin lesions in order to prevent severe complications of hypercalcemia [9]. The pathogenesis behind SCFN and hyperkalaemia is not known till date. The initial hypoxic injury [6] combined with maternal diabetes are likely to be cause of hypoglycaemia in neonates with SCFN.Mobilization of fatty acids from the adipose tissue might cause hypertriglyceridemia in neonates with SCFN [10].
Haematological problems like thrombocytopenia [1] and thrombocytosis [15] have been encountered previously with this condition. Hypoxic insult [6], sequestration of platelets in the subcutaneous tissue [16] and increased prostaglandin E levels [5] have been implicated as possible causes of thrombocytopenia while reactive inflammatory response [15] is proposed as a possible cause of thrombocytosis in neonates with SCFN.
While the above-mentioned complications were not encountered in our patient, it was found that the total leucocyte count continued to remain on the higher limit of normal during the neonatal period (figure 3) with higher percentage of lymphocytes. Follow up routine blood tests at 6 weeks showed high white cell count (19.4) with 69% lymphocytes suggesting persistent leucocytosis. There were no intercurrent illnesses recorded in this period. Although physiological leucocytosis is a normal finding in neonates, the white cell count returns to baseline by 1 month of age and the reference white cell count from one month to 23 months ranges from 6.0-14.0 x 109 cells/mm3[8]. We propose that a reactive inflammatory response could have been a likely cause for high white cell count in our patient.
A study by Tognetti L et al. [17] show that ultrasonographic study of SCFN revealed flogistic fat involvement with calcifications, while ultrasound of the skin nodule in our patient only showed diffuse edema with no evidence of collection. Skin biopsy of SCFN nodule usually shows inflammatory histiocytic reaction with fat tissue necrosis. Extensive granulocytic infiltrate including macrophages, giant cells, eosinophils, and lymphocytes are usually present [18]. Although skin biopsy was not performed in our patient, there are evidences to suggest that SFCN of a neonate is a clinical diagnosis and skin biopsy is helpful in atypical cases [19]. This literature combined with the presence of risk factors and resolution of the nodule at the end of 4 months supports a clinical diagnosis of SCFN in our patient.
Learning Points/Take Home Messages
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
