
Case Report | DOI: https://doi.org/10.31579/2690-4861/088
*Corresponding Author: Gurwant Kaur, Assistant Professor, Penn State Milton S. Hershey Medical Center, Hershey, PA.
Citation: Y Leyfman, A Tsay, A Zebi, S Baghli, Kaur. (2021) Acute Kidney Injury in a Case of Multiorgan Failure, Disseminated Intravascular Coagulation and Purpura Fulminans. International Journal of Clinical Case Reports and Reviews. 6(2); DOI:10.31579/2690-4861/088
Copyright: © 2021 Gurwant Kaur, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 October 2020 | Accepted: 29 December 2020 | Published: 08 January 2021
Keywords: purpura fulminans; multiorgan failure; acute kidney injury; dic
Introduction
Purpura fulminans (PF) is a life-threatening syndrome consisting of Disseminated Intravascular Coagulation (DIC), thrombotic occlusion of small- and medium-sized blood vessels with skin necrosis. Although there are few studies in the literature, only a minority of them discuss renal manifestations.
Case Report
We present a case of a 57-year-old Caucasian female with acute kidney injury (AKI) in the setting of multiorgan failure (MOF), DIC and PF. She presented with fever, exudative drainage from her port site, and skin changes concerning for bacteremia. Empiric antibiotics were started after blood, urine, and wound cultures were obtained. None of the cultures grew any organisms. Fever resolved after port removal. She exhibited thrombocytopenia, leukopenia, and neutropenia. Urinalysis showed hyaline casts and a fractional excretion of urea (FeUrea) ≤35% indicating a pre-renal state. Her hospital course was complicated by atrial fibrillation, acute hypoxic respiratory failure requiring mechanical ventilation, and hypovolemic shock requiring pressor support. Further, complicated by multiorgan failure including non-oliguric AKI and heart failure with reduced ejection fraction (HFrEF) of ≤65%. Acute skin findings included dusky, purple macules and patches involving all digits of both hands as well as gangrenous changes on the face and toes. It prompted further investigation by Hematology and Dermatology. Skin biopsy showed early leukocytoclastic vasculitis changes. Her laboratory markers were suggestive of DIC and Purpura Fulminans.
Purpura fulminans (PF) is a rare and life-threatening syndrome. This was first described by Octave Guelliot in 1884. This presents as intravascular thrombosis and hemorrhagic infarction of the skin and soft tissue that rapidly progresses to multiorgan failure [1]. PF manifests as either a hereditary or acquired deficiency of Proteins C (PROC gene mutation) or S (PROS1 gene mutation). This results in a pro-coagulable state leading to thrombotic occlusion of small and medium-sized blood vessels and manifests as Disseminated Intravascular Coagulation (DIC) and [2-4]. Protein S deficiencies are also caused by liver disease [5].
Although the presentation can vary, patients present with erythematous purpuric macules with blue-black hemorrhagic necrosis typically along the peripheral portions of the skin [5]. Thrombosis of the small vessels leads to hemorrhagic cutaneous necrosis, hypotension, DIC and purpura [1, 6]. Prolonged thrombosis of the small and medium-sized blood vessels will result in full-thickness skin and soft-tissue necrosis of the deeper tissues with MOF of lungs, kidneys, central nervous system, and adrenal glands [7, 8]. This possesses a high mortality rate of close to 50% with most survivors requiring an amputation of the affected extremities [9, 10].
PF can be seen in the setting of sepsis, DIC, or malignancy. There is scarcity of studies on PF in the literature. However, there are few observed cases that can document the extent of this condition in relation to kidney injury. Herein, we present a case of 57-year-old female who exhibited kidney injury in the context of this condition.
A 57-year-old Caucasian female was referred to the Emergency Department by her family physician for concerns of a Mediport infection. She experienced fevers, chills, nausea, and vomiting over the course of 24 hours. Her Mediport was placed 6 days prior to presentation for relapsed vs. residual acute myeloid leukemia (AML). The port was draining purulent material.
Her past medical history included hypertension, a hip fracture requiring total hip replacement and hypercalcemia. She was diagnosed with AML in May 2018. She received a fully matched living related allogenic stem cell transplant (SCT) from her sister in August 2018. Her induction therapy included Fludarabine/Busulfan (Flu/Bu2) followed by methotrexate and Neupogen. Her post- SCT course was complicated by non-oliguric acute kidney injury (AKI) and hepatic graft-versus-host disease (GVHD). Her baseline serum Creatinine (Cr) prior to SCT was 0.6 mg/dL and it trended to a maximum of 3.2 mg/dL. AKI was pre-renal in nature due to poor oral intake and was treated with conservative management. Her current immunosuppression included Prednisone and Tacrolimus. Family history is not significant for cancers, bleeding disorders or kidney disease.
Hospital Course
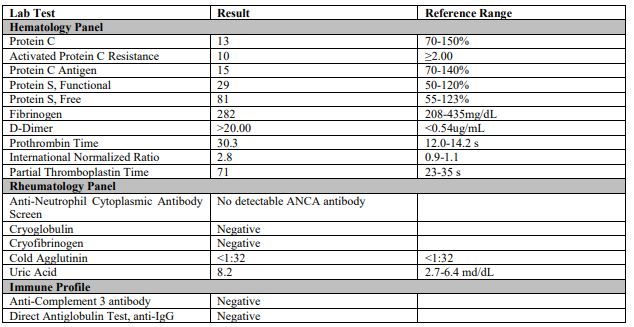
She presented with fever of 37.9°C, heart rate of 64 beats per minute, and 20 breaths per minutes. Her blood pressure was 153/75 mmHg. On physical exam, she was breathing comfortably on room air. She had minimal dried yellow-green drainage around her port site. The overlying skin was erythematous and tender to palpation. All other physical examinations were unremarkable. Her laboratory data is outlined in Table 1. Chest X-ray was unremarkable. Patient was started on empiric intravenous antibiotics (Piperacillin-Tazobactam and Vancomycin) for concerns of a port infection. Trimethoprim-Sulfamethoxazole (TMP-SMX), Acyclovir, and Posaconazole were started as prophylaxis coverage. Blood, urine, and wound cultures remained negative. She had initial resolution of fevers after Mediport removal. Later, she began to have confusion along with intermittent fevers. Magnetic resonance imaging (MRI) of brain and lumbar puncture were unremarkable as well. However, she continued to have recurring and persistent fevers; she was diagnosed with influenza B and was started on oseltamivir.
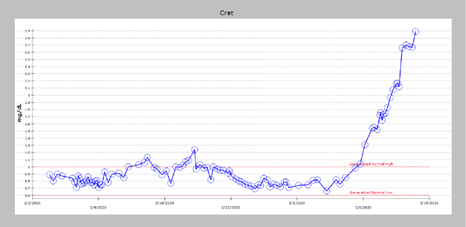
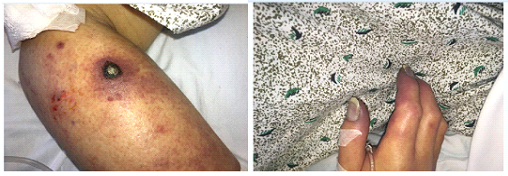
On hospital day 36, she became hypoxic with new oxygen requirement and new onset atrial fibrillation (AF) with rapid ventricular rate (RVR). She needed end tracheal intubation with pressor support. Nephrology was consulted for non-oliguric AKI with an up trending serum Cr of 1.55 mg/dL (baseline Cr as 0.9 mg/dL) as shown in Figure 1. During her intensive care unit (ICU) stay, she was noted to have necrotic nodule as shown in Figure 2a. The surrounding area had dusky macules and patches involving bilateral hand digits Figure 2b). Differential diagnoses included angioinvasive fungal infection, DIC, or Antineutrophil cytoplasmic antibodies (ANCA) related vasculitis. Also, she had notable gangrenous changes on her nose, fingers, and toes.
She continued to have worsening of serum Cr reaching 2.6 mg/dL, and her serum lactate was 9.2mmol/L. Renal replacement therapy (RRT) was not initiated given goals of care discussion with her family. The patient eventually passed away despite implementing life saving measures to prevent DIC in the setting of PF and DIC.
Pathogenesis
There are five different subtypes of PF.
1. The most common form is acute or severe sepsis caused by gram negative organisms, including Neisseria meningitidis, Streptococcus pneumonia and Hemophilus influenza [3, 11]. Asplenic patients are at an increased risk [12]
2. The idiopathic or autoimmune form presents with autoantibodies against protein C or S after infections like chicken pox.
3. The acquired form is due to a depletion or decreased synthesis of protein C typically in the presence of vitamin K antagonists, severe liver failure, or complications of prematurity.
4. The congenital form is an autosomal dominant condition with a loss of function due to mutations in protein C, protein S, or antithrombin 3.
5. This subtype is a combination of sepsis and congenital defects that occurs due to mutations in Protein C [13].
Endo- and exotoxins released by gram negative organisms activate tumor necrosis factor-α (TNF-α) and interleukin 2 (IL-2). This results in the consumption of proteins C and S [14, 15]. A deficiency in proteins C and S results in a pro-coagulable state and contributes to the thrombosis of small and medium sized blood vessels.
On presentation, she had thrombocytopenia, leukopenia with neutropenia, mild hypokalemia, and elevated liver enzymes. Her urinalysis showed hyaline casts and fractional excretion of urea (FeUrea) was ≤35% (Table 1). A transthoracic echocardiogram (TTE) showed a reduced left ventricular ejection fraction (LVEF) of 45%. A repeat TTE two weeks later showed mildly improved LVEF 50% and new findings of right ventricular (RV) dilation. CT thorax revealed right upper lobe ground glass opacities suggestive of inflammatory or infectious process. A bronchoalveolar lavage (BAL) was negative for bacteria, aspergillosis, nocardia, legionella, anaerobes, and acid-fast bacilli. Cytomegalovirus was negative. A coagulation panel on Day 36 (Table 1) demonstrated elevated D-dimer, PT, PTT, INR, and fibrinogen with thrombocytopenia— a presentation aligned with DIC. Protein C and S were low. She had negative serum ANCA, cryoglobulin, and cryofibrinogen. Cold Agglutinin was within normal limits, which ruled out an infectious cause (Mycoplasma pneumoniae or other primary atypical pneumonia causing pathogens). Uric acid was elevated, which could support tumor lysis syndrome (TLS) in the setting of AML. Anti-IgG direct antiglobulin test (DAT) and antibody screen were negative for autoimmune hemolytic anemia (Table 2). Skin biopsy showed early leukocytoclastic vasculitis changes. A new necrotic nodule on the patient’s right forearm revealed vascular occlusion with negative fungal stains suggestive of PF.
In this case, AKI was largely multifactorial. There was no evidence of acute tubular necrosis (ATN) given lack of urinary granular casts or tissue diagnosis/kidney biopsy; but was highly possible in later course with oligoanuria. Her sub-nephrotic range proteinuria was likely tubular in nature as well. A kidney biopsy was not feasible given critical clinical situation of the patient. Hence, it is hard to prove toxic ATN from medications. Also, she was maintained on reasonable vancomycin levels. Multiple factors contributing to AKI in this case included chemotherapy with underlying immunosuppressed status secondary to AML, use of immunomodulators, sepsis/septic shock (culture negative), antibiotics and decreased effective circulating volume in phase of AF with RVR. Septic shock with MOF along with worsening lactic acidosis preceded the worsening of AKI.
PF is a condition with a poor prognosis and high mortality rate of over 40%, where supportive care is the mainstay of treatment [1, 5, 18]. Studies have suggested anticoagulation to halt necrosis, and replacement of blood and blood products (coagulation factors, and platelets) to control DIC progression. In advanced cases, like ours, it is also recommended that patients be given fresh frozen plasma and protein C concentrate to improve survival rates. However, our patient’s clinical course was too advanced to halt disease progression[13, 19]. Early surgical debridement of necrotic areas has been shown to decrease mortality [20, 21].
This case demonstrates the importance of early diagnosis and intervention in advanced life-threatening conditions, like PF, due to its rapid course and poor clinical outcome.
The authors declare that they have no competing interests.
Author’s Contributions
YL was responsible for reviewing the literature, summarizing and organizing the data, and writing the Abstract, Introduction, and Discussion of the manuscript. AT was responsible for gathering the data, summarizing the patient’s clinical course, organizing the data, contributing to the Discussion, and writing the case presentation of the manuscript.
AZ and SB were responsible for editing the discussion.
GK was responsible for reviewing and editing the entire manuscript multiple times. GK also provided critical thinking and finalized the manuscript. All authors read and approved the final manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
