
Case Report | DOI: https://doi.org/10.31579/2690-4861/084
*Corresponding Author: Mahasine ELHARRAS, Cheick Khalifa International University Hospital, Mohammed VI University of Health Sciences (UM6SS), Mohamed Taib Naciri avenue, Hay Hassani, ZC: 82403, Casablanca, Morocco.
Citation: M.El Harras, S.Abdeladim, I.Bensahi, A.El Ouarradi, S.Oualim, M.Sabry. (2020) The Left Ventricular Aneurysm: The Cardiologist Prevent, the Surgical Team Treats. International Journal of Clinical Case Reports and Reviews. 4(5);DOI: 10.31579/2690-4861/084
Copyright: © This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 October 2020 | Accepted: 02 December 2020 | Published: 22 December 2020
Keywords: left ventricular aneurysms; pseudo aneurysm; coronary artery disease; ventricular thrombi; systemic embolization
Left ventricular aneurysms, both true and pseudo aneurysm, are a consequence of coronary heart disease. Trans thoracic echography is the gold standard in the assessment of the left ventricular aneurysm; the most frequent complication is the development of blood stasis and left ventricular thrombi with the risk of systemic embolization, the use of long-term oral anticoagulant therapy is controversal , Left ventricular aneurysm surgery , often with myocardial revascularization, is indicated in well-defined cases, with several surgical technique, depending on the type of aneurysm, the anatomical caractehristics and the team skill’s, we report in this article tow cases of the left ventricular aneurysm.
Py: package years
TTE: Transthoracic echocardiography
LV: left ventricul
LVA: left ventricular aneurysm
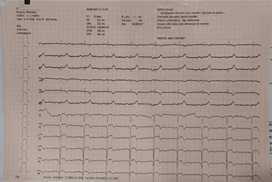
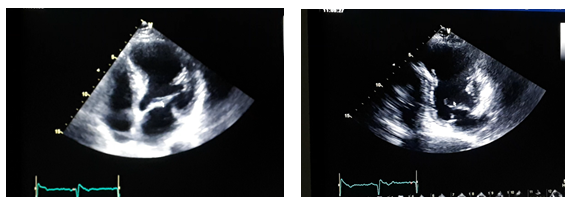
A 67 years old man smoker at 40 py, cessed since 20 years. He suffered an acute myocardial infarction.20 years earlier; he underwent percutaneous coronary intervention with stents in left anterior descending artery in 1999 and 2001. He presented a left sided weaknes with slured speech then aphasia related to a left superficial sylvien stroke, without pain or dyspnea, His 12-lead electrocardiogram (fig 1)showed a persistent ST segment elevation and QS waves in the precordial leads (it was similar to the anterior ECGs), Chest X-ray showed cardio-thoracic ration of 0.75,Transthoracic echocardiography (TTE) revealed the presence of aneurysm of the apico-septal left ventricular (LV) wall( fig 2), the coronarography showed a stenosis of 70 % of the proximal left anterior descending artery , intrastent subocclusive restenosis of the middle left anterior descending artery ( fig 3). The heart team decided to propose MR B.M to LVA surgery and to prefer the endoventricular circular plasty, myocardial revascularization will be discussed during the perioperator time

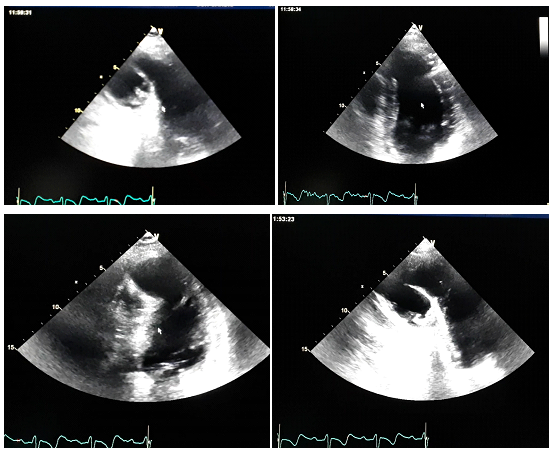
A 55 years old man smoker at 15 py, cessed since 40 years, having a high blood pressure, and diabetes. He suffered an acute myocardial infarction 10 years earlier; he underwent double coronary bypass grafting. He ran away during 4 years because of an psychological disorder and he stoped his medical treatement even after returning home. One week before his hospitalization he presented an acute chest pain without dyspnea, none syncope, His 12-lead electrocardiogram showed a QS waves in V1 and negative T wave in the anterior and inferior territory, Transthoracic echocardiography (TTE) revealed severe left ventricular dysfunction, the presence of an pseudoaneurysm of the apical left ventricular (LV) wall, with the presence of thrombus (fig 4), the coronarography showed a severe triple vessel coronary artery disease (fig 5). The heart team decided to propose BO.M to LVA surgery but the patient refused and preferred medical treatment.

Left ventricular aneurysm is a real consequence of coronary heart disease, both acute myocardial infarctus and chronic coronary disease [1]. In the other side 5% of left ventricular aneurysm are reported to trauma, Chagas disease, and sarcoidosis [2].
A true ventricular aneurysm differs from a pseudoaneurysm in terms of morphology and risk of rupture.A true ventricular aneurysm is defined as a thinning of the ventricular wall in an area void of muscle and is caused by fibrosis or scar formation; it is akinetic and bulges during the cardiac cycle. On the contrary the pseudoaneurysm has a narrow neck and is a rupture of the myocardial wall contained by pericardium, thrombus or adhesions, but none of the myocardium elements are present in the wall of the pseudoaneurysm. Differentiating these is clinically relevant as pseudoaneurysms have a greater risk of rupture and need surgical treatment [2, 3, 4].
The formation of a Left ventricular aneurysm involves in two phases: at first we have expansion of transmural necrosis in second phase wall stresses are increased at theborder zone so we have subsequent remodeling. The early expansion occurs in the area of the myocardial infarctus, whereas the remodeling phase affects the myocyt cells, leading to fibrosis and changes in the geometry of the ventricular cavity. [2, 5]A normal conic left ventricular apical configuration is essential for cardiac pump function. After ischemic injury, the helical apex of the myocardium loosens; resulting in a spherical myocardial geometry could be associated with decreased left ventricular systolic function [6].
Within the first month after ischemia there is a decrease in aneurysm size, followed by a progressive enlargement of the aneurysm. The adverse outcomes are directly linked to left ventricular aneurysm’s larger [6]. Moreover, larger of the left ventricular aneurysm were an independent predictor of an adverse outcome after adjusting for the LVEF, which is a well-validated prognostic factor [7]. Left ventricular aneurysm occurrence is a risk factor for the development of left ventricular thrombi, blood stasis, subendocardial injury and hypercoagulability play also a role in thrombus formation. [6, 8]
TTE represent the gold standard in the assessment of the LVA. The wall of the LV aneurysm is very thin and localized pericardial effusion is present at TTE. Computed tomographyand magnetic resonance imaging can also be used to identify aneurysms [2, 9]
In the early 1980s, Reeder et al reported that mural thrombus was present in 48% of the patients undergoing left ventricular surgery and correlated inversely with the duration of previous anticoagulant therapy [10]. In 1985, Lapeyre et al, concluded that the extremely low incidence of systemic emboli in patients with chronic LV aneurysm did not justify the use of long-term oral anticoagulant therapy. [11, 12]
Ga Yeon Lee et al compared outcomes of anticoagulation therapy using warfarin in patients with ischemic LVAs both acute and chronic LVAs after ischemic injury. Death, nonfatal MI, CVA, systemic embolization, and primary and secondary outcomes as composites of those cardiac and cerebrovascular events did not differ according to anticoagulation status. [13] Further studies are needed to confirm these finding.
Left ventricular aneurysm Surgery is indicated in refractory heart failure, persistent angina, thromboembolism, or life-threatening tachy arrhythmias occur. Myocardial revascularization is typically performed at the time of aneurysmectomy. After 5 years, the survival rate is approximately 69% for patients undergoing aneurysmectomy and either revascularization or mitral valve replacement, compared with 57% for those undergoing aneurysmectomy alone. [14]
There are several surgical techniques for Left ventricular aneurysm: plication, linear closure, circular patch, and endoventricular patch. The endoventricular circular plasty technique is principally the first line surgical technique. The improvement in left ventricular geometry and the decrease in the tension of the muscle fibers that this technique provides result in a decrease of oxygen consumption and an improvement in cardiac performance as indicated by increased left ventricular ejection fraction, reduced left ventricular end-diastolic pressure, and decreased left ventricular volume. The technique also provides revascularization, especially combined with endoventricular circular plasty, can improve cardiac function by increasing blood flow and oxygen supply to the ischemic areas of the myocardium.[2] The circular plasty technique may be the better choice for patients with extensive and defined fibrotic aneurysmal sacs, whereas Cooley technique or linear closure may also be preferable in patients whose aneurysms lack a well-defined border [15].
The best way to heal is to prevent the improvement and the accessibility of revascularization in acute MI or Chronic Coronary Syndromes and the optimization of the coronary heart disease’s medical treatment had and will have a positive impact to reduce the prevalence of LVA.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
