
Review Article | DOI: https://doi.org/10.31579/2643-6612/020
1Skeletal Biology Research Center, Department of Oral and Maxillofacial Surgery, Massachusetts General Hospital, Harvard School of Dental Medicine, Boston, MA, USA.
2Biomaterials Group, Department of Physical Chemistry, São Paulo State University (Unesp), Institute of Chemistry, Araraquara, SP, Brazil.
*Corresponding Author: Fernando P.S. Guastaldi, Department of Oral and Maxillofacial Surgery, Massachusetts General Hospital, Harvard School of Dental Medicine, Boston, MA, USA.
Citation: F.P.S. Guastaldi, J.L.G.C. Monteiro, T. Takusagawa, A.C. Guastaldi. A review of biomechanical studies for mandibular angle fracture internal fixation, J Dentistry and Oral Maxillofacial Surgery. 4(1) DOI: 10.31579/2643-6612/020
Copyright: © 2021 :Fernando P.S. Guastaldi, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 23 August 2021 | Accepted: 10 September 2021 | Published: 14 September 2021
Keywords: Mandibular angle fractures; internal fixation; biomechanics; mechanical testing.
Mandible fractures correspond to 19-40% of all facial fractures. Among all mandible fractures, 12-30% are fractures of the mandibular angle. These fractures are mainly caused by sports activities, interpersonal violence and car accidents. The presence of the third molar and the thin transverse bone area seem to be responsible for the frequent involvement of the mandibular angle in facial fractures. Before the advent of antibiotics, a high frequency of infection was always associated after an open reduction in mandibular angle fractures. Wired osteosynthesis and maxillomandibular fixation (MMF) were traditional methods for fixing mandibular angle fractures. The limitation of both methods has influenced the development of new approaches for the treatment of mandibular angle fractures. Currently, osteosynthesis of mandibular angle fractures with plates and screws has become an effective treatment option. Several forms are described in the literature as: fixation of bone segments with a miniplate on the upper edge of the mandible, fixation with two miniplates, lag screw or by a single rigid plate on the lower edge of the mandible. The purpose of this study was to summarize the main characteristics of biomechanical studies such as the type of mandible source used, the plating techniques employed, the plate material, and the loading protocols used to evaluate the stability of the fixation methods. The Medline (PubMed) database was searched combining relevant terms and pertinent articles in English were included. Articles had to meet the following inclusion criteria: be in vitro biomechanical studies evaluating fixation methods for mandibular angle fractures. A total of 27 articles fulfilled the inclusion criteria. Synthetic mandibles (n=12), animal mandibles (n=9), and human cadaveric mandibles (n=5) were used as the sample source to perform the biomechanical analysis. One article used both synthetic and human cadaveric mandibles. Also, a variety of fixation techniques was described such as mini-plates, lag-screws, reconstruction plates, and three-dimensional plates. The materials of the bone plates used were: stainless steel, commercially pure titanium, titanium alloy or bioresorbable. However, there was inconsistency in reporting the materials and not all studies clearly stated the material of the bone plates. For the biomechanical analysis, there was a high variation among all studies regarding the loading protocols used. The same side of fixation, the anterior part of the mandible (central incisors) or the contralateral side were reported as the dentate regions in which the force was applied. For more than 2 decades, in vitro biomechanical studies have been used to help researchers and clinicians in the field of Oral and Maxillofacial Surgery to properly evaluate and compare the different devices and techniques available for the treatment of mandibular angle fractures. Also, biomechanical studies are important to answer questions on fatigue performance and fracture strength on the gross level.
The mandible is the largest, strongest and the only movable stress bearing bone of the face (Wong et al., 2011). However, position, prominence, anatomic configuration, mobility, and less bone support make the mandibular bone fractures occurring twice as frequently as fractures of the midface (de Matos et al., 2010). The distribution of fracture sites seems to be influenced by the cause of the injury, which in turn is influenced by geographic locations, local behavior, and socioeconomic trends (Erdmann et al., 2008; Bormann et al., 2009). Mostly, these injuries are related to a traumatic incidence including traffic accident, interpersonal violence, falls, and sport injuries (Zachariades et al., 2006; Jain et al., 2009).Mandible fractures correspond to 19-40% of all facial fractures. Of these, 12-30
A computer database search was performed, using Medline (PubMed) without data restriction. The following search criteria was used: (("mandible"[MeSH Terms] OR "mandible"[All Fields]) OR ("mandible"[MeSH Terms] OR "mandible"[All Fields] OR "mandibular"[All Fields])) AND (("fractures, bone"[MeSH Terms] OR ("fractures"[All Fields] AND "bone"[All Fields]) OR "bone fractures"[All Fields] OR "fracture"[All Fields]) OR ("injuries"[Subheading] OR "injuries"[All Fields] OR "trauma"[All Fields] OR "wounds and injuries"[MeSH Terms] OR ("wounds"[All Fields] AND "injuries"[All Fields]) OR "wounds and injuries"[All Fields]) OR ("wounds and injuries"[MeSH Terms] OR ("wounds"[All Fields] AND "injuries"[All Fields]) OR "wounds and injuries"[All Fields] OR "injury"[All Fields])) AND (angle[All Fields] OR angulus[All Fields]) AND (biomechanical[All Fields] OR ("in vitro techniques"[MeSH Terms] OR ("vitro"[All Fields] AND "techniques"[All Fields]) OR "in vitro techniques"[All Fields] OR "vitro"[All Fields] OR "in vitro"[All Fields])).
Terms were limited to studies that were published in the English language. Studies were included if models were used for looking at the biomechanics of any method of mandibular angle fracture fixation either alone or in combination with clinical studies. Studies were excluded if the full text wasn’t available, if they reported on models used any other site of mandibular fracture fixation, bone graft for mandibular reconstruction, orthognathic surgery, distraction osteogenesis, dental implants and dental prosthesis. Any papers reporting only clinical outcomes were also excluded.
Articles that met the inclusion criteria based on their abstract information were selected. Articles were also obtained when there was not enough information in the abstracts or if a citation had no abstract.The following data was extracted from each article: author(s), year of publication, title, sample source (human, animal or synthetic), plating technique and plate material, and load-bearing area (for the biomechanical analysis). These data were summarized in figures and tables and descriptive statistic was provided when appropriate.
The search (performed on March 11th, 2020) yielded a total of 134 titles. After reading the titles and abstracts, a total of 27 articles were selected for reading the full text and for data extraction (Table 1).
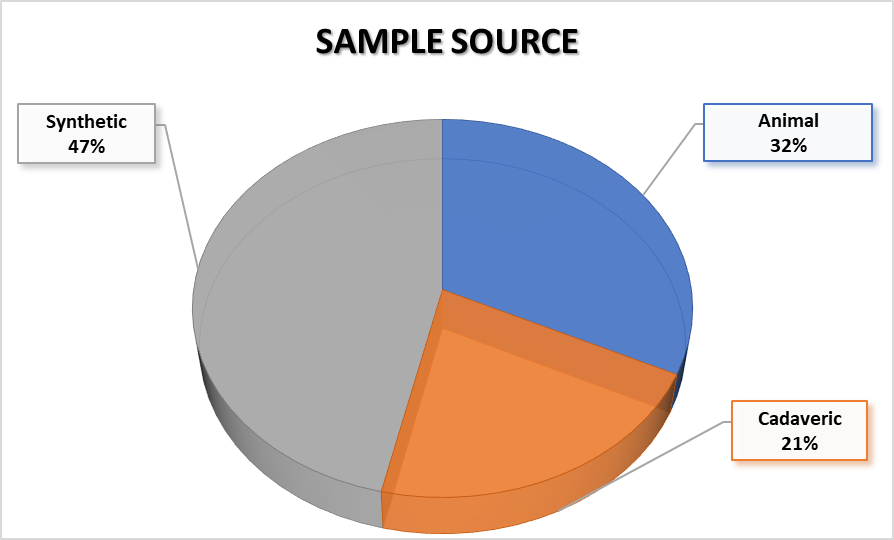
Nine studies were performed in mandibles derived from animals. In these studies, sheep mandibles were used. Four studies used mandibles derived from human donors, and 11 studies used synthetic mandibles, mostly composed of polyurethane. One study performed analysis in both human cadaveric and synthetic mandibles (Figure 2).
A variety of plates from different manufacturers was described as follows: titanium miniplates, resorbable miniplates (poly-DL-lactic acid; PDLLA), locking and non-locking systems, plates with tridimensional design, and reconstruction plates. The constitution of the plates was not adequately reported in most papers; however, some mentioned details regarding the materials.
A single-plating technique was the most performed technique in most articles, and the site for fixation was usually the external oblique ridge, according to principles of Champy et al. (1976), using a four-hole plate. However, a fixation on the intermediary portion of the fracture was also reported (middle of the buccal surface). The site of fixation if a second place was chosen was the inferior mandible border. However, if only the inferior border was plated, a reconstruction plate was used. Fixation only with screws was also reported (Shetty and Caputo 1992; Shetty et al., 1995). One article reported fixation with a Herbert bone screw (Wallner et al., 2017). Table 2 provides a summary of the included biomechanical studies of mandibular angle fractures.
After the mandible was plated, most studies performed biomechanical tests applying loadings on the same side of the fixation, generally on the molar region. Other variations include loading on the canines, bicuspids, between the canine and first bicuspids, and 20 mm anterior to the osteotomy site. Some studies also applied loading the contralateral side and vertical loading at the central incisors. One article (Suer et al., 2014) reported using a machine stated to simulate the masticatory muscles, which was designed to apply vertical, lateral and tensile forces (Figure 3).

The aim of this study was to summarize the methodological aspects of biomechanical in vitro studies evaluating different plating and fixation techniques for mandibular angle fractures. Also, synthetic jawbone models, animal mandibles, and cadaver mandibles have been described in the scientific literature as the sample source in in vitro studies. They are used to evaluate the mechanical strength and stability of the different available fixation systems for the treatment of mandibular angle fractures (Wong et al., 2011; Guastaldi et al., 2014; Guastaldi et al., 2020). Due to the significant complications (i.e. infection, malocclusion) that may arise from the treatment of these fractures (Zimmermann et al., 2017), different treatment modalities have been proposed in the last 30 years aimed at improving fracture stability. These include using plates with different thickness (Alkan et al., 2007; Turgut et al., 2008), plates with different composition [i.e., commercially pure titanium versus titanium alloys (Guastaldi et al., 2014)], plates with three-dimensional configuration (Kalfarentzos et al., 2009; Oliveira et al., 2018), resorbable materials (Cural et al., 2018), lag screws (Shetty & Caputo, 1992), and even bone adhesives (Cural et al., 2018).
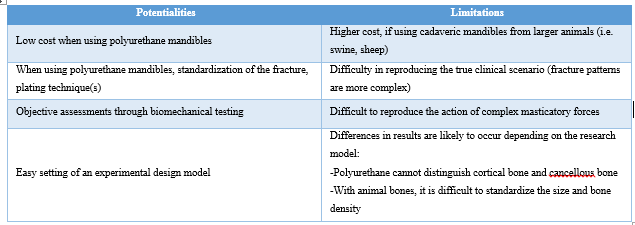
The thin cross-section of the mandibular angle in addition sometimes to the presence of impacted third molars makes this region prone to fractures (Dhara et al., 2019), which may occur in association with multiple facial fractures and other patient morbidities (Le et al., 2020). Moreover, high-energy trauma (i.e. road traffic accidents) is usually associated with these injuries (Jaber et al., 2020) causing a comminution that furthers complicates treatment (Chen et al., 2018; Sikora et al., 2019). These factors make the treatment of mandibular angle fractures challenging and hinders carrying controlled studies to evaluate different treatments. Therefore, in vitro studies try to replicate patterns of mandibular angle fracture to overcome the limitations of standardized patient recruitment. Table 3 presents some potentialities and limitations of biomechanical studies.
It has been shown that the screw dimeter influences the distribution of stress/strains in holes, which is directly related to screw loosening (Yoon et al., 2014). Also, the results from computational modeling studies [i.e. finite element analysis (FEA)] simulating the distribution of stress/strains along fracture lines show that screw position is an additional factor that influences microstrains on holes (Guastaldi et al., 2020; Ramos et al., 2020). However, there are some limitations of computational models, such as the lack of mechanical testing to evaluate fatigue performance and the fact that FEA modelling is applied to a static situation. Therefore, in vitro studies help to validate the accuracy and precision of these models (Wong et al., 2011). Additionally, there are some testing machines that can simulate the action of the masticatory muscles (Suer et al., 2014), which is an important factor in the real clinical scenario. Also, incisal edge loading, along with molar loading, inflicts a combination of torsional and vertically deforming forces that are encountered clinically (Haug et al., 2002). Table 4 describe some information of available standards that should be used when performing biomechanical studies for mandibular angle fixation.

Mandibular angle fractures still represent one of the most controversial issues in the relevant literature, especially regarding the recommended treatment. The evolution of internal fixation was aided by the discovery of biocompatible materials that resisted corrosion, such as vitallium and titanium. Currently, titanium is the metal of choice for fixation plates, mainly because of its high biocompatibility, ease of manipulation, and the potential for no second surgery. Additionally, efforts have been made to increase the use of resorbable plates. However, few studies have investigated the biomechanical behavior of the stability when using resorbable plates and screws (Cural et al., 2018). Although a spectrum of techniques for treatment of angle fractures with plates/screws has been proposed in the literature (Table 5), and what constitutes adequate stability at a fractured mandibular angle remains controversial (Levy et al., 1991; Schierle et al., 1997; Ellis, 1999).
Biomechanical studies of mandibular angle fracture fixation are challenging due to the complex forces acting on the mandible. They represent a valuable methodology to identify trends in behavior, however these trends need to be verified with clinical investigations. There isn’t a consensus regarding the “gold standard” treatment of mandibular angle fractures. However biomechanical studies contribute to the assessment of the biomechanical performance for the stable internal fixation of mandibular angle fractures. Also, they are important to develop new techniques and help to answer questions on fatigue performance and fracture strength on the gross level.
The authors declare that they have no competing interests.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
