
Review Article | DOI: https://doi.org/10.31579/2640-1053/225
College of Health Sciences, Hawler Medical University, Erbil, Iraq.
*Corresponding Author: Fattma A. Ali. College of Health Sciences, Hawler Medical University, Erbil, Iraq.
Citation: Yasmeen M. Khalil, Fattma A. Ali, Ahmed A. K. Al-Daoody, Muna M. Najeeb, (2025), Treatment of Breast Cancer by Monoclonal Antibodies, J Cancer Research and Cellular Therapeutics, 9(1); DOI:10.31579/2640-1053/225
Copyright: © 2025, Fattma A. Ali. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 December 2024 | Accepted: 24 December 2024 | Published: 02 January 2025
Keywords: monoclonal antibody; breast cancer; HER2-positive breast cancer
Breast cancer continues to be a significant global health concern, prompting ongoing research to create innovative treatment options. Monoclonal antibodies (mAb) are emerging as a promising and targeted method for treating breast cancer, offering greater specificity and fewer side effects than traditional treatments. This overview highlights the current landscape of monoclonal antibody therapy for breast cancer. These antibodies are engineered proteins designed to specifically identify and attach to antigens found on cancer cell surfaces. A key benefit of monoclonal antibody therapy is its ability to inhibit the growth and survival of cancer cells while protecting normal cells. This targeted method minimizes side effects and enhances the treatment's safety profile. Combination therapies, which may include monoclonal antibodies alongside standard chemotherapy or other targeted treatments, are being explored for their potential to create synergistic effects and improve patient outcomes. Despite the promise of this approach, challenges persist, such as the emergence of resistance mechanisms and the necessity for tailored treatment strategies. Ongoing clinical trials are examining combination therapies and investigating new targets to tackle these challenges. Additionally, managing side effects and addressing economic factors associated with monoclonal antibody treatments are active areas of research. While mAb therapies can lead to side effects like fever, chills, fatigue, headaches, muscle pain, nausea, vomiting, breathing difficulties, skin rashes, and bleeding, this study reviews the current and future prospects of monoclonal antibodies in diagnosing and treating breast cancer, taking into account the advantages and disadvantages of this technique.
Breast cancer is a growth of abnormal cells in the ducts or lobules and can be classified into invasive and non-invasive cancers that affect both male and female [1]. The use of monoclonal antibodies in breast cancer can restore or improve immune system function. A monoclonal antibody (mAb) is defined as a laboratory-created molecule designed to bind to antigens on the surface of cancer cells in order to attack cancer cells by restoring, strengthening, or mimicking the immune system [2]. monoclonal antibody was fully licensed in 1986, the development of monoclonal antibodies is a new way to target specific mutations and defects in protein structure and expression in many diseases and conditions [3]. Today, humanized monoclonal antibodies are the fastest growing class of biotechnology-derived molecules in clinical trials, as the translation of genetic sequencing and basic medical research into clinical practice has progressed rapidly. The global value of the antibody market is approximately $20 billion annually. The FDA currently has 30 monoclonal antibodies approved for use in humans for a variety of diseases and conditions, including cancer, chronic inflammatory diseases, organ transplants, infectious diseases, and hearts diseases [4]. Monoclonal antibodies are drugs that inhibit specific targets on the surface of cancer cells. The target may also be present in nearby areas of the cancer cells/tissues. Monoclonal antibodies possess the ability to generate toxicity towards cancer cells. Chemotherapy and radiation therapy can successfully and efficiently target cancer cells, as example (5). Monoclonal antibodies possess three key distinguishing features that set them apart from other treatment methods. Firstly, they exhibit tumor selectivity, meaning they specifically target tumors. Secondly, monoclonal antibodies can be modified, such as by attaching stable linkers that are cleaved upon entering a cell. Lastly, humanized monoclonal antibodies are not immunogenic and cause low systemic toxicity [6]. This review covers the types, mechanisms of action and targeted delivery to breast cancer cells of monoclonal antibodies used to treat breast cancer. Three major molecular markers categorize breast cancer patients into subtypes: estrogen receptor (ER), progesterone receptor (PR), and Human epidermal growth factor receptor-2 (2). Targeted antibodies act on tumor cells through several mechanisms. Tumor signaling can be inhibited by antibodies that interfere with growth signaling pathways through modulation of the active state of receptors located on the cell membrane or by inhibiting cytokines that play a crucial role in tumor growth and development. Various agents, including drugs, radioactive materials, and toxins, have the ability to effectively eradicate tumor cells. However, their toxicity towards healthy tissues restricts their therapeutic application. Conjugating anticancer drugs to antibodies can minimize adverse effects. Optimal antibodies are those that specifically bind to antigens exclusively present on malignant cells [5].
The traditional monoclonal antibody (mAb) production process typically begins with the generation of mAb-producing cells (i.e., hybridomas) by fusing myeloma cells with spleen cells (e.g., B cells) that produce the desired antibody. Typically, these B cells are derived from animals, particularly mice. Following cell fusion, a large number of clones undergoes screening and selection according to their antigen specificity and immunoglobulin class. After identifying prospective hybridoma cell lines, each one was subsequently confirmed, validated, and characterized by a series of upstream functional assays. Once the clones have matured, they are expanded with further downstream bioprocesses occurring [7]. A typical monoclonal antibody production process:
2.2 Half-life of antibodies
The half-life of a monoclonal antibody (mAb) can vary widely depending on the specific antibody, its structural characteristics, its interaction with the target antigen, and also its interaction with the immune system [5]. Monoclonal antibodies are molecules created in the laboratory that can mimic the immune system and its ability to fight harmful pathogens such as viruses and cancer cells. Several monoclonal antibodies have been developed and studied for therapeutic effects in the setting of breast cancer. It is important to note that the availability and approval of specific monoclonal antibodies varies by region and may vary over time [8]. Some monoclonal antibodies kill cancer cells by binding directly to them. These monoclonal antibodies are called targeted therapies because they target specific receptors on cells. An example is trastuzumab (Herceptin), which is used to treat HER2-positive breast cancer. HER2-positive breast cancer is a type of breast cancer that is characterized by the presence of a protein known as human epidermal growth factor receptor 2 (HER2). This protein stimulates the proliferation of cancer cells. In 20% of breast cancer cases, the tumor cells exhibit gene amplification, resulting in an additional copy of the HER2 protein gene. HER2-positive breast cancer exhibits a higher level of aggressiveness compared to other forms of breast cancer [9]. Trastuzumab binds to the HER2 receptor on cancer cells and prevents them from growing, stopping the growth and slowing the progression of the cancer. Additional monoclonal antibodies enhance the immune system's ability to combat cancer cells. These substances are referred to as immunotherapies. Nivolumab is an instance of a drug that specifically targets the PD-1 receptor. It is employed for the treatment of various types of cancers such as lung cancer, kidney cancer, melanoma, lymphoma, and some head and neck cancers [10].
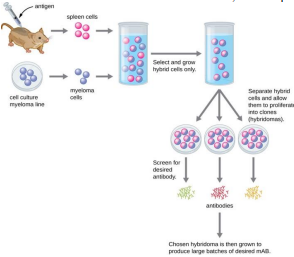
Figure 1: typical monoclonal antibody production process
2.3 Examples of Monoclonal antibodies.
Here are some examples of monoclonal antibodies. used or under investigation for breast cancer:
The addition of trastuzumab into chemotherapy resulted in several positive outcomes, including a delayed disease progression, an increased rate of objective response, a prolonged response duration, a decreased mortality rate, extended survival, and a reduced risk of death [11].
Figure 2: Monoclonal antibodies like Herceptin, block HER2 receptors, preventing growth factors binding to the cell. This stops the accelerated growth and division.
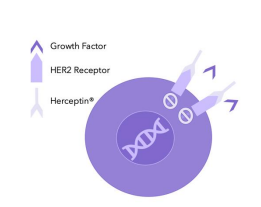
Figure 2: Monoclonal antibodies like Herceptin, block HER2 receptors, preventing growth factors binding to the cell. This stops the accelerated growth and division.
2.2 Pertuzumab (Perjeta):
While not a traditional monoclonal antibody, denosumab is a targeted therapy that inhibits the activity of a protein involved in bone destruction. It is used to prevent bone complications in certain cases of advanced breast cancer [15].
Palbociclib, Ribociclib, and Abemaciclib: While not traditional monoclonal antibodies, these drugs are cyclin-dependent kinase 4/6 (CDK4/6) inhibitors and are often used in combination with hormone therapy. They work to inhibit the activity of CDK4 and CDK6, which are proteins involved in cell cycle regulation.it is approved for the treatment of HR+, HER2- advanced breast cancer in combination with an aromatase inhibitor as initial endocrine-based therapy or in combination with fulvestrant in patients who have received prior endocrine therapy [16].
promising target for monoclonal antibody is the programmed cell death protein 1 (PD-1) and its ligand PD-L1, which are key components of the immune system and play a crucial role in regulating immune responses. PD-1 is a cell surface receptor expressed on activated T cells, which are a type of immune system cells. The primary function of PD-1 is to regulate the immune response and prevent excessive activation, which could lead to autoimmune reactions. When PD-1 binds to its ligands, PD-L1 or PD-L2, it inhibits the activity of T cells, dampening the immune response. which play a crucial role in immune checkpoint regulation. Antibodies that block the PD-1/PD-L1 interaction have been developed as cancer immunotherapies. These antibodies, such as pembrolizumab and nivolumab (targeting PD-1) Atezolizumab, which targets PD-L1, is part of a group of drugs called immune checkpoint inhibitors. checkpoint inhibitors work by releasing the "brakes" on the immune system, allowing T cells to recognize and attack cancer cells more effectively. These therapies have shown significant success in the treatment of various cancers, including melanoma, lung cancer, and certain types of breast cancer, especially triple-negative breast cancer (TNBC). targeting the PD-1/PD-L1 pathway with monoclonal antibodies has become a groundbreaking approach in cancer immunotherapy, providing a way to enhance the body's natural immune response against cancer cells. These antibodies unleash the immune system to recognize and attack cancer cells, providing a novel immunotherapeutic approach [17].
Monoclonal antibodies can be used with other treatment methods such as chemotherapy, radiation therapy, and surgery, depending on the stage and characteristics of the breast cancer.
2.3 Indications for Use and Administration
Indications for mAbs in oncology include both solid tumor and hematologic malignancies. mAbs may be administered intravenously as well as subcutaneously [9].
2.4 Benefits of Monoclonal Antibody Therapy for Breast Cancer:
Monoclonal antibody therapy has brought about significant benefits in the treatment of breast cancer, particularly in the context of targeted therapies. Here are some key advantages:
2.5 Future perspectives of monoclonal antibodies for breast cancer:
The future prospects for monoclonal antibodies against breast cancer are bright. This is because research and development are focused on improving the effectiveness of treatment, reducing side effects and expanding the range of treatments that are prescribed. Some key areas for future exploration include:
Monoclonal antibodies have emerged as a transformative force in breast cancer treatment, changing the landscape of treatment options and significantly improving patient outcomes. Engineered to selectively bind to particular chemicals present on the outer membrane of cancer cells, these laboratory-developed antibodies represent a paradigm shift in precision medicine, providing individualized and targeted approaches to breast cancer patients. This conclusion discusses major achievements, challenges, and ongoing developments in monoclonal antibody therapy for breast cancer. One of the most important success stories in monoclonal antibody therapy is the victory over HER2-positive breast cancer. Trastuzumab, a pioneering monoclonal antibody, has become the cornerstone of therapy for HER2-positive breast cancer. Trastuzumab, which specifically targets the HER2 receptor overexpressed in cancer cells, has led to unprecedented improvements in survival and disease. The addition of pertuzumab and ado-trastuzumab emtansine (T-DM1) to the treatment arsenal continues to demonstrate the success of combination strategies, providing more comprehensive and effective approaches to the treatment of HER2-positive breast cancer. Equally important is the study of monoclonal antibodies in the complex landscape of triple negative breast cancer (TNBC). The emergence of immune checkpoint inhibitors, such as pembrolizumab and atezolizumab, has opened new avenues for the treatment of TNBC, which lacks targeted receptors commonly found in other breast cancer subtypes. Designed to unleash the power of the immune system against cancer cells, these immunotherapies offer hope to a patient population that has historically had limited options for targeted therapies. The promise of monoclonal antibodies extends beyond their efficacy; it includes a vision of personalized medicine. These antibodies are adapted to recognize specific molecular signatures of tumors, enabling treatment strategies tailored to the unique characteristics of each patient and cancer. This customization not only increases therapeutic effectiveness, but also mitigates potential side effects, marking an important step forward in the pursuit of more patient care. However, the journey of monoclonal antibody therapy in breast cancer is not without its challenges. Mechanisms of resistance, variable patient responses, and the need for improved biomarkers are areas that require continued investigation and clarification. The dynamic and heterogeneous nature of breast cancer requires a nuanced understanding of the complex interactions between the immune system and cancer cells. Unraveling the complexity of the tumor microenvironment and identifying strong prognostic biomarkers are critical steps in optimizing the use of monoclonal antibodies in breast cancer therapy. Development of monoclonal antibody therapy for breast cancer has not stopped at all; it is a continuum characterized by relentless research and innovation. Clinical trials investigating new antibodies, targets and combinations are at the forefront of this development and aim to further improve outcomes and expand the applicability of these therapies. The emphasis on combination strategies that include monoclonal antibodies in combination with chemotherapy, targeted agents, and immunotherapies emphasizes a holistic approach to overcoming the challenges of breast cancer. In conclusion, monoclonal antibodies have steadily shaped the history of breast cancer treatment, offering hope, efficacy and personalization. The success stories of HER2-positive breast cancer and promising advances in TNBC are examples of the transformative power of precision medicine. As the field advances, the integration of biosimilars, ongoing research projects and dedication to unraveling the complexities of breast cancer biology point to a future where monoclonal antibody therapy is a sign of progress in the fight against breast cancer.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
