
Case Report | DOI: https://doi.org/10.31579/2641-0419/369
Riojan Health Service, Emergency Service 061, Piqueras 98, 26006, Logroño, La Rioja, Spain.
*Corresponding Author: Alejandro Jesús Bermejo Valdés, Riojan Health Service, Emergency Service 061, Piqueras 98, 26006, Logroño, La Rioja, Spain.
Citation: Bermejo Valdés AJ, Sara I. Gutiérrez, Basilio T. Ruiz, (2024), First description of a mixed Brugada pattern in inferior leads, J Clinical Cardiology and Cardiovascular Interventions, 7(4); DOI: 10.31579/2641-0419/369
Copyright: © 2024, Alejandro Jesús Bermejo Valdés. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 April 2024 | Accepted: 08 May 2024 | Published: 16 May 2024
Keywords: brugada syndrome; channelopathy; arrhythmias
Brugada Syndrome is a cardiac channelopathy closely related to lethal arrhythmias and sudden death in people without underlying structural pathology. The diagnosis is usually assumed with electrocardiographic patterns strictly limited to the right precordial leads, V1 or V2; but this is not so at all. In our article, we present the clinical case of a patient with a novel and different electrocardiographic presentation: the typical diagnostic pattern was presented in a lower lead of the electrocardiogram, and next to it, another pattern was presented in a contiguous lead. In addition, we propose the possible association of a structural pathology (non-compaction cardiomyopathy) with Brugada Syndrome, since both share a possible common genetic origin in the SCN5A gene.
Brugada Syndrome (BrS) is a channelopathy of myocardial cells, first described in 1992, with characteristic electrocardiographic patterns, which determines a predisposition to sudden death and lethal ventricular arrhythmias[1].
Today, the diagnosis of BrS is based on the electrocardiogram (ECG), for which, according to the latest advances, two basic morphological patterns have been described. The diagnosis is made if, excluding phenocopies, one of the following criteria is met[1].
1. ST segment elevation with type 1 pattern morphology: ≥ 2 mm in one or more of the right precordial leads (V1 or V2), positioned in the second, third, or fourth intercostal space.
2. Type 1 morphology appears either spontaneously or after intravenous pharmacological challenge tests using sodium channel blockers (for example: ajmaline).
The type 1 pattern is diagnostic[1,2].
The remaining pattern, called type 2, is characterized by ST segment elevation in right precordial leads ˃ 1 mm, followed by a positive or isobiphasic T wave, which gives the ST-T complex a “saddleback” appearance[1,2].
The Brugada patterns are due to the affectation of the transmural electrical potential gradient in phase 1 of the action potential, due to the imbalance between the input and output of ions to the cardiomyocyte[2]. On the other hand, the genetic origin of BrS implies the involvement of cardiomyocytes as a whole. However, it appears that there is specificity of Brugada patterns in the right precordial leads[1,2]. Although theoretically, repolarization should also be affected in other leads.
Below, we present the case of a patient in whom a type 1 pattern in lead III was found on the same electrocardiographic tracing together with a type 2 pattern in lead II, in the context of syncope with refractory vagal symptoms.
A 69-year-old male, with no known toxic habits, who consumes bisoprolol 2.5 mg every 12 hours, with a personal history of non-compaction cardiomyopathy, and mild-moderate aortic and mitral regurgitation. No family history. He suffers from syncope without prodromes at home with a refractory vagal picture. The ECG performed by the Advanced Life Support team (Figure 1) showed sinus bradycardia and a posterior three-lead bipolar rhythm strip (Figure 2) revealed a Brugada type 1 pattern morphology in III, along with a type 2 pattern in II.
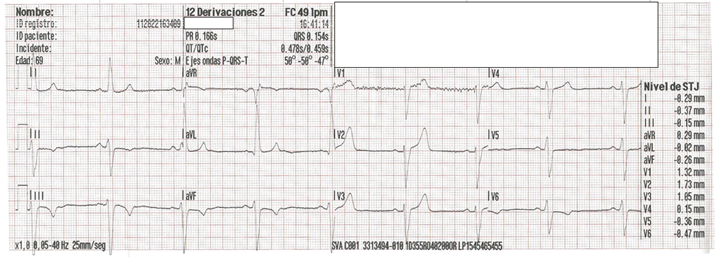
Sinus bradycardia at 49 bpm.

Appearance of type 1 (in III) and type 2 (in II) Brugada patterns.
Upon his arrival at the hospital, he had a blood pressure of 80/40 mmHg; remainder of the normal physical examination. The analysis was anodyne, with negative troponin seriation. Thus, after the initial assessment in the ER, it was decided to consult with Cardiology.
In the electrocardiographic analysis of Figure 2 we have: Lead I: We interpret it as a mirror image of III; Lead II: Brugada pattern type 2, and Lead III: Brugada pattern type 1.
The literature describes the variability of Brugada patterns in the same patient, even on the same day[1], and the existence of BrS patterns in lower limb leads[3] has also been described. However, we did not find reported cases that concomitantly present different patterns in the same tracing.
Regarding the presentation of Brugada patterns in lower leads, Sarkozy et al.[3] concluded that there are indeed Brugada patterns only in lower
leads. Even in one of the cases with a single presentation with a type 2 pattern, the challenge with ajmaline produced the transformation towards a type 1 pattern, also inferior[3].
In a molecular biology study, Potetet al.[4] detected that mutations of the SCN5A gene, which encodes structures of the sodium channel of myocardial cells, can produce a Brugada phenotype in inferior leads.
Based on the work of Chevallier et al.[5], we have been able to verify that the type 2 pattern morphology of the record in Figure 2 is equivalent to the type 2 pattern described for right precordial leads. We measuring the angle β (> 58º) and length of the base of the triangle of the r' wave 5 mm below the point of maximum ascent (4 mm)[1] (Figure 3), which are variables with high predictive values, sensitivity and specificity that allow discerning between type 2 patterns and other causes such as, for example, branch locks[1].

Lead II of Figure 2. Calculation of the angle β and the base of the triangle that involves the wave r'.
Based on this, we can anticipate that, in this case, a mixed electrocardiographic pattern was observed, at the same moment, in two lower leads.
To support the diagnosis of BrS, in the case presented, the presence of BrS phenocopies (ECG tracings with morphology that mimics BrS but with demonstrable environmental etiology) cited by Baranchuket al.[6] (metabolic causes, extracardiac mechanical compression, ischemia) was ruled out, coronary artery disease, pericardial disease, tricuspid valve defects, and electrocution).
It is also interesting to make a reference to the relationship between vagal symptoms and BrS. Mizumakiet al.[7] conclude that in BrS there is a spontaneous increase in ST elevation related to an increase in vagal tone that may occur at some point in daily life.
Lastly, regarding the previous diagnosis of non-compaction cardiomyopathy in the patient we present, there are precedents in the literature of its possible relationship with BrS. Park et al.[8] described a man with non-compaction cardiomyopathy whose baseline ECG showed a Brugada type 2 pattern in right precordial leads. Chevallier et al.[5] reported a case of non-compaction cardiomyopathy in a sample of patients with Brugada patterns. This generated the need for us to investigate if any data was reported that related these two pathologies from a more scientifically sustainable profile, for example, from a genetic profile. Shan et al.[9] described in 2007 a mutation of the SCN5A gene in patients with non-compaction cardiomyopathy who presented arrhythmias. Here we would have a molecular origin, a gene, common to two phenotypically different pathologies, BrS and non-compaction cardiomyopathy.
Brugada patterns should no longer be considered as circumscribed to right precordial leads; it is possible to distinguish them also on the underside. There is even the possibility of finding mixed patterns (type 1 together with type 2) in lower leads, on the same electrocardiographic tracing.
In patients with non-compaction cardiomyopathy, with or without vagal association, due to a possible common genetic origin in the SCN5A gene, the coexistence of a BrS is possible. Likewise, when faced with a refractory vagal clinical picture, an ECG is recommended.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
