AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2768-0487/155
Critical Care Unit, Kafr El-Bateekh Central Hospital, Damietta, Egyptian Ministry of Health (MOH), Egypt.
*Corresponding Author: Yasser Mohammed Hassanain Elsayed., Critical Care Unit, Kafr El-Bateekh Central Hospital, Damietta, Egyptian Ministry of Health (MOH), Egypt.
Citation: Yasser M H Elsayed., (2024). Yasser’s Sphygmomanometer Procedure; a Newly Therapeutic Procedure for the Psychogenic Hemiplegia in the Emergency Medicine and Neuropsychiatry-Case Series., Journal of Clinical and Laboratory Research 7(9); DOI:10.31579/2768-0487/155
Copyright: © 2024, Yasser Mohammed Hassanain Elsayed. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 November 2024 | Accepted: 15 November 2024 | Published: 02 December 2024
Keywords: psychogenic hemiplegia; regaining the movement; mimics; pseudostroke; psychogenic movement disorders; conversion disorder; motor functional neurological disorder
Introduction: Psychogenic hemiplegia is a suggestive symptom of stroke but in reality, is of psychogenic origin. Psychogenic hemiplegia is an identical subgroup of pseudostroke, and psychogenic movement disorders, and mimics for differential diagnosis of stroke. Treatment of psychogenic hemiplegia is still challenging.
The research objectives aimed to evaluate the hypothesis that Yasser’s sphygmomanometer procedure can regain movement and improvement of psychogenic hemiplegia.
Method of study and patients: The study was technical, prospective, observational, and interventional for 31 cases. This study was conducted in Kafr El-Bateekh Central Hospital, Fraskour Central Hospital, and a physician outpatient clinic. The author reported 31 cases of psychogenic hemiplegia over nearly 5 years and 3 months, starting on May 07, 2019, and, ending on August 12, 2024.
Results: A total of 31 patients are included in this study. There is a female sex predominance of 87.1%. The mean age of the cases was 35.29 years (range; 16-65). The most common occupation in the study was housewife; 54.84%. The most commonly associated hemiplegia was the left-side hemiplegia of cases; 90.32% vs. right-side; 6.45% and reversal; 3.23%. Latent tetany was the most predominant; 90.32% vs. the manifested; 9.68%. Wavy triple sign (WTS) was the most frequent ECG sign; 35.48%, then Wavy double sign (WDS); 22.58%, and combined WTS and WTS; 16.13%, WTS with Tee-Pee sign and Camel hump T-waves; 6.45%. Ionized hypocalcemia was detected in 32.26%. The response was complete but with a single recurrence.
Conclusions: The author concluded that Yasser’s sphygmomanometer procedure is easy, available, quick, non-costive, time-saving, and extremely safe for psychogenic hemiplegia. There is a strong association between hypocalcemia (clinical, ECG, and ionized hypocalcemia) and psychogenic hemiplegia. There were no reported complications for this procedure encouraging the generalizing use in psychogenic hemiplegia. Further widening the research to include the cases of organic stroke is essential.
Ca++: Calcium
CHTW: Camel hump T-waves
ED: Emergency department
ECG: Electrocardiography
EEG: Electroencephalography
FND; Functional neurological disorder
GCS: Glasgow Coma Scale
HR: Heart rate
ICU: Intensive care unit
IHD: Ischemic heart disease
NSR: Normal sinus rhythm
O2: Oxygen
PMD: Psychogenic Movement Disorders
POC: Physician outpatient clinic
PS: Pseudostroke
PVCs: Premature ventricular complexes
TPS: Tee-Pee sign
WDS; Wavy double sign
WTS: Wavy triple sign
Psychogenic hemiplegia
1.1 Introduction and Significance
Stroke is one of the most common diseases affecting 25% of people during their lifetime [1]. Most strokes are ischemic due to a reduction or interruption of blood flow (BF) to the brain. Approximately, 20–30% of strokes are hemorrhagic and result from damage to small or medium-size vessels [1]. Stroke is a medical emergency that presents with focal neurological deficits. Rapid assessment, confirmation of diagnosis, and treatment to re-establish BF leads to improvement in symptoms and prevention of brain damage [2].
1.2 Mimics of Stroke and Psychogenic Pseudostroke are Included
Mimics is about 25% of hospital admissions for suspected stroke [3]. The prevalence of stroke mimics is variable and depends on the focal diagnosis. It can be 20–50% of cases of acute suspected stroke depending on if the patients were assessed by the emergency or stroke physicians [4–6]. Psychogenic pseudostroke (PS) is a suggestive symptom of a stroke, but in reality, of psychogenic origin [7]. However, specific information regarding its management is deficient [7].
1.3 Psychogenic Movement Disorders and Conversion Disorders are implicated
Psychogenic Movement Disorders (PMD) are one of the most challenging neuropsychiatric disorders for both neurologists and psychiatrists. PMD has confounded the specialists of both these disciplines, time and again, over more than a century. These disorders cannot be fully accounted for by any known organic syndrome and have significant psychological and or psychiatric contributions [8]. The psychogenic neurological disorders include psychogenic hemiplegia, paraplegia, blindness, seizures, pain syndromes, a variety of movement disorders, and PMD. The latter include hyperkinetic syndromes of tremors, jerks, spasms (dystonias), gait disorders, and a hypokinetic extrapyramidal syndrome mimicking Parkinsonism [8]. Conversion disorder is an unconscious psychological response to a stressful situation [9,10].
1.4 Prevalence in Mimics of Stroke and Pseudostroke
Psychogenic symptoms reported in virtually all medicine specialties. Approximately 33% of outpatient's neurologic symptoms as being “nonorganic”. Most neurologists have encountered a case of such nature [7]. However, little information exists on psychogenic pseudostroke (PS). However, specific information regarding its prevalence, epidemiology, demographics, and psychopathology of PS is scarce [7]. The exact prevalence or incidence of PMD is idiopathic [8].
1.5 Somatoform Disorders, Factitious Disorders, and Malingering in Differentiation
According to the (DSM-IV-TR), physical symptoms due to psychological causes fall under three classes: somatoform disorders, factitious disorders, and malingering. Somatoform disorders, factitious disorders, and malingering fall among the most difficult differentiating issues for neuropsychologists [11]. It is essential to entertain stroke mimics in the differential diagnosis when treating an acute suspected stroke to avoid the inappropriate use of expensive and potentially harmful medications. This becomes particularly important with telestroke and hospitals with limited acute stroke experience [4]. The differential diagnosis of conversion disorder includes strokes, multiple sclerosis, and epilepsy [9,10]. Younger, females are commoner than males, altered level of consciousness, gradual in onset, fluctuations in severity, no vascular distribution, blood pressure usually not increased, sensory, vertigo (or dizziness) and visual, may have involuntary movements, unilateral facial twitching, lip-smacking, giveaway weakness, and arm drift/abrupt fall without pronation are considered in mimics of stroke and pseudostroke [3].
1.6 Diagnosis with Clinical Manifestations and Fallacies
Presentation is very varied and requires a high degree of suspicion. Stroke mimics may present as a functional (conversion) disorder or may be part of the symptomatology of a neurological or medical disorder. The diagnosis of acute ischemic stroke is however not always straightforward. Similar symptoms may develop in number of medical conditions commonly referred to as “stroke mimics” [3]. Diagnosis and management of PS are difficult. Factors that influence diagnosis (or misdiagnosis) and management of PS may be legal, ethical, moral, or financial. PS is when the acute symptoms are suggestive of a stroke but are of psychogenic origin. There are several challenges in the diagnosis and management of these patients. PS is unlike other psychogenic neurologic symptoms. Its presentation is acute and may be an isolated event. PS is and always should be a diagnosis of exclusion that requires concurrence of physical exam and diagnostic testing. Red flags suggest PS may be present, but caution is warranted to avoid a hasty diagnosis. Here are some of the potential indicators: previous history of psychogenic symptoms, history of other unexplained conditions that have undergone extensive work up to no avail, and coexisting, poorly-defined symptoms. PS is not only and simply a stroke mimicker, it is an entity in its own right [7]. Recent rates of stroke under-diagnosis (false-negative cases, "stroke chameleons") range from 2-26% and 30-43% for stroke over-diagnosis (false-positive cases, "stroke mimics") [6]. Functional mimics or conversion disorders are less frequent [12–15]. Some patients admitted to acute stroke units are diagnosed as stroke mimics. A minority have a functional neurological disorder ('functional mimics') [13]. A common type of stroke mimic is a functional neurological disorder presenting with limb weakness, numbness, or speech disturbances (previously known as psychogenic or conversion disorder) [16]. The essential feature of conversion disorder is the presence of symptoms or deficits affecting voluntary sensory or motor activity. These symptoms are not intentionally produced. Motor deficits include impaired balance, paralysis, limb weakness, and urinary retention. According to the DMS-5 criteria, the following features are identified for psychogenic paralysis etiology: [1] Contradictory clinical findings such as normal muscle tone, normal deep reflex, or pyramidal signs; [2] Paradoxical behavior; [3] Normal electrophysiological features; and [4] Normal radiographic findings [10,17]. Conversion symptoms are often inconsistent. A "paralyzed" extremity will be moved inadvertently while dressing, or when attention is as conversion disorder. Individuals with this disorder may show label indifference or lack of concern about the nature or implications of their symptoms [18]. Clinical features of PMD include: 1] increase or become elaborate when examination is focused on the affected part, 2] decrease or resolve when not the clear focus of attention or inquiry and during tests requiring concentration or other tasks, 3] triggered or relieved with unusual non-physiological interventions (such as trigger points on the body, tuning fork), 4) deliberate slowness of movements, 5] rhythmical and often violent shaking, 6] changing characteristics of movements -severity, frequency, type, and distribution, 7] entrainment (see below), 8] selective disability, 9] demonstration of fatigue, 10] presence of multiple movement disorders, 11] presence of bizarre movements which are difficult to classify, 12] excessive startle response, 13] paroxysmal movement disorders, and 14) bizarre gait [8]. The absence of expected findings of disk herniation, epidural hematoma, or contusion of the spinal cord will suggests and supports the diagnosis of Conversion Disorder [18]. Failure to diagnose stroke can preclude time-sensitive treatments and has been associated with poor outcomes [6]. Functional stroke mimics are an important subgroup admitted to acute stroke services and have a distinct demographic and clinical profile [13]. Hoover's sign, hip abductor sign, drift without pronation, and give-way weakness (collapsing) are helping signs in functional stroke mimics [16].
1.7 Risk Factors
Stroke mimics may have systemic illness, psychological stress, younger, often had a previous history of migraines or seizures, and fewer vascular risk factors [3]. Psychogenic hemiplegia is prominent among multiple sclerosis, myasthenia gravis, and idiopathic or substance-induced dystonia [18].
1.8 Prognosis and Burden
Generally, the prognosis of motor functional neurological disorder (FND) seems unfavorable [14] and considered poor [15]. Psychogenic paralysis after minor trauma presents a difficult medico-legal issue [18]. The prognosis for full recovery is unfortunately not very good with more than one-third of patients reporting the same or worse deficits during follow-up [20]. While many underlying conditions can be recognized rapidly by careful assessment, a significant proportion of patients unfortunately still receive thrombolysis and admission to a high-intensity stroke unit with inherent risks and unnecessary costs [3]. Additional strategies to improve the accuracy of stroke diagnosis should focus on rapid clinical reasoning in the time-sensitive setting of acute ischemic stroke and identifying imperfections in the healthcare system that may contribute to diagnostic error [6]. These rates of stroke mimic diagnosis pose a high burden on healthcare resources [3].
1.9 Workup
Workup is aimed at reducing underdiagnoses in atypical stroke presentations [6]. Multi-modal CT or magnetic resonance imaging (MRI) may be helpful to confirm an acute ischemic stroke and is necessary if stroke mimics are suspected [3]. A diagnosis of Conversion Disorder should be made only after a thorough medical investigation has been performed to rule out a neurological or general medical condition [10,17]. There are no specific laboratory abnormalities are associated with this condition [18]. Neurodiagnostic techniques measure brain and spinal cord dysfunction that might otherwise be missed with CT or MRI. They complement imaging techniques by providing a noninvasive measure of the existing physiology [21-23]. At times, physicians are faced with situations in which a patient's symptoms are not completely compatible with the description of the original accident or the physical examination [24-29]. In such cases, electrophysiological examination including modalities such as somatosensory evoked potentials (SSEPs) or transcranial motor evoked potentials (TcMEPs) confirms the psychogenic nature of the neurologic deficit [22,23,30].
1.10 Management
Management of PS patients should begin with a prudent, respectful, yet truthful disclosure [7]. In contrast to the unconscious nature of symptoms in somatoform disorders, factitious disorder, and malingering suggest that the patient is purposely being deceptive [7]. Treatment of functional disorders can be challenging, is often incomplete, and requires early psychiatric intervention [3].
My study was technical, prospective, and interventional for 31 cases. The study was conducted in the physician outpatient clinic (POC), Kafr El-Bateekh Central Hospital, and Fraskour Central Hospital. The author reported 31 cases of psychogenic hemiplegia over 5 years and 3 months, starting on May 07, 2019, and, ending on August 12, 2024 (Table 1). Complete clinical and specifically neurological examination was done for all cases. CBC, liver enzymes, RBS, renal function tests, and sometimes ABG were done as routine investigations in most cases. ECG tracings were only provided. Ionized calcium was used in most cases. Clinical and laboratory data of all cases were collected (Tables 2 and 3).
• Suggesting hypothesis and research objectives
| Issue | Definition |
Title
| Yasser’s Sphygmomanometer Procedure and Dramatic Recovery for the Psychogenic Hemiplegia; a New Maneuver in Emergency Medicine and Neuropsychiatry |
| Estimated enrollment | 31 participants |
| Study type | Technical, observational, and interventional |
| Observational model | Case series |
| Time | Prospective |
| Study date | Started on May 07, 2019, and ended on August 12, 2024 |
Table 1: Showing remarks on the study method and data.
• Eligibility criteria:
Case presentations
• Case No. 1: A 42-year-old married female Teacher, Egyptian patient was presented to the physician outpatient clinic (POC) after psychological stress due to a home burn with left side weakness, ipsilateral body aches, and ipsilateral facial weakness and numbness. She was tested for latent tetany which was positive.

Figure 1A : ECG tracing shows a wavy triple sign of hypocalcemia.
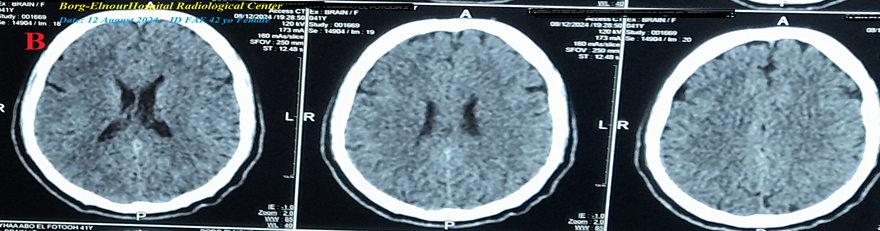
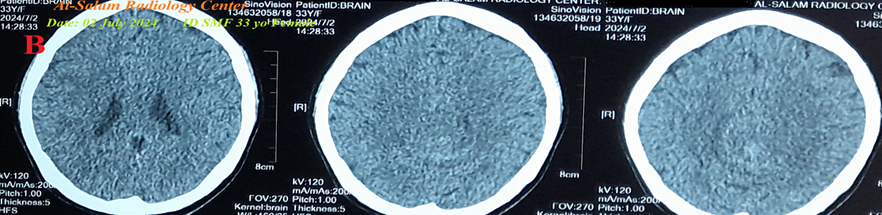
Figure 1B : There are laboratory hypocalcemia and vitamin D deficiency. Brain CT was normal.
Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
Figure 1 A-ECG tracing on the day of the presentation shows a Wavy triple sign” in V1 (dark blue, red, and lime arrows) and superficial T-wave inversion in III, V2, and V3 leads. B-Brain CT sections were done on the day of the presentation showing no abnormalities. Red arrows =elevated beats, green arrows = isoelectric beats, and blue arrows =depressed beats.
• Case No. 2: A 29-year-old married female housewife Egyptian patient was presented to the POC after sadness with left side weakness, ipsilateral body aches, ipsilateral facial weakness, and hyperventilation syndrome. She was tested for latent tetany which was positive. There is laboratory hypocalcemia.
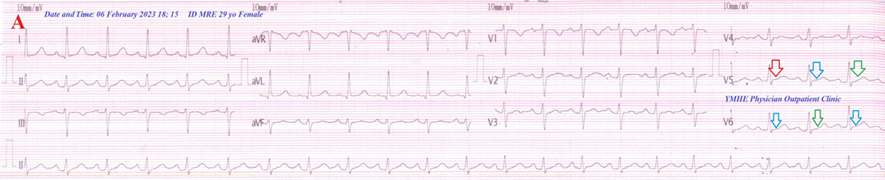
Figure 2A: ECG tracing shows wavy triple and wavy double signs of hypocalcemia.
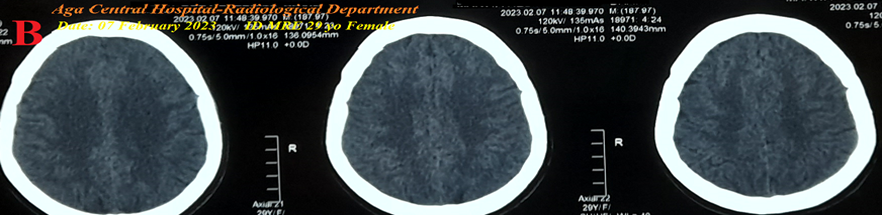
Figure 2B: Brain CT was normal.
Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
Figure 2 A-ECG tracing on the day of the presentation shows a Wavy triple sign” in V5 (light blue, red, and green arrows) and a Wavy double sign” in V6 (light blue and green arrows). B-Brain CT sections were done on the second day of the presentation showing no abnormalities. Red arrows =elevated beats, green arrows = isoelectric beats, and blue arrows =depressed beats.
• Case No. 3: A 37-year-old Employee married female Egyptian patient was presented to the ICU after stress with left side weakness, ipsilateral body aches, and paresthesia. She was tested for latent tetany which was positive.
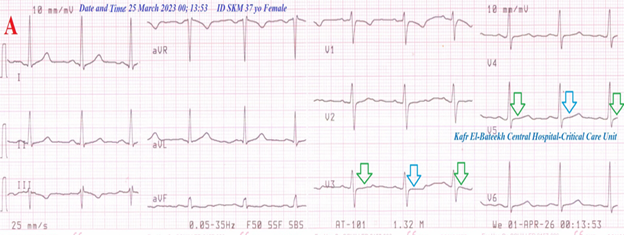
Figure 3A: ECG tracing shows a wavy double sign of hypocalcemia.
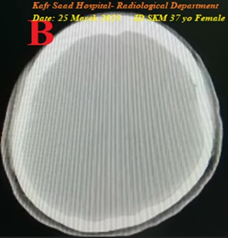
Figure 3B: Brain CT was normal .
Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
Figure 3 A-ECG tracing on the day of the presentation shows a Wavy double sign” in V3 and V5 (light blue and green arrows). B-Brain CT video section was done on the day of the presentation showing no abnormalities. Green arrows = isoelectric beats, and blue arrows =depressed beats.
• Case No. 4: A 42-year-old married Housewife female Egyptian patient was presented to the emergency department (ED) after stress with left side weakness, ipsilateral body aches, and numbness. She was tested for latent tetany which was positive.
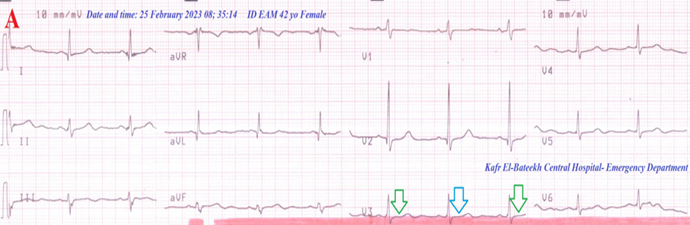
Figure 4A: ECG tracing shows a wavy double sign of hypocalcemia .
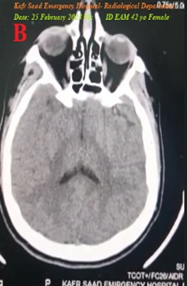
Figure 4B: Brain CT was normal .
Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
Figure 4 A-ECG tracing on the day of the presentation shows a Wavy double sign” in V3 (light blue and green arrows). B-Brain CT video section was done on the day of the presentation showing no abnormalities. Green arrows = isoelectric beats, and blue arrows =depressed beats.
• Case No. 5: A 23-year-old divorced housewife female Egyptian patient was presented to the ICU after psycho-familial troubles with left-side weakness, ipsilateral body aches, tachypnea, and numbness. She was tested for latent tetany which was positive.
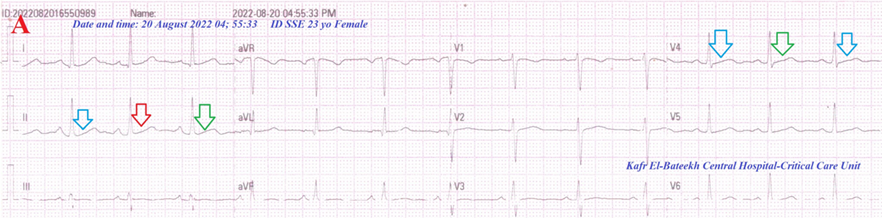
Figure 5A: ECG tracing shows wavy triple and wavy double signs of hypocalcemia .
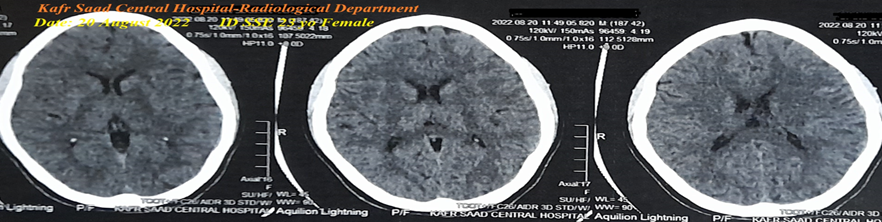
Figure 5B: There is laboratory hypocalcemia. Brain CT was normal .
Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
Figure 5 A-ECG tracing on the day of the presentation shows a Wavy triple sign” in lead II (light blue, red, and green arrows) and a Wavy double sign” in V4 (light blue and green arrows). B-Brain CT sections were done on the second day of the presentation showing no abnormalities. Red arrows =elevated beats, green arrows = isoelectric beats, and blue arrows =depressed beats.
• Case No. 6: A 42-year-old married female housewife Egyptian patient was presented to the POC after psycho-familial troubles with right side weakness, ipsilateral body aches, ipsilateral facial weakness, and paresthesia. She was tested for latent tetany which was positive.
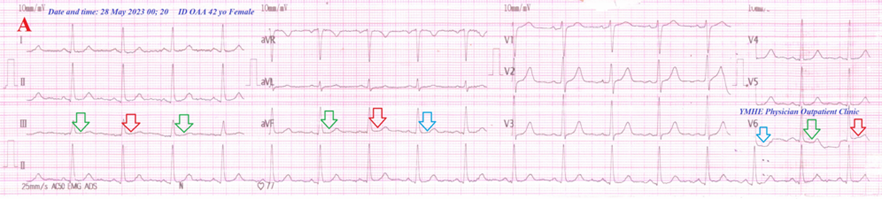
Figure 6A: ECG tracing shows Wavy triple and Wavy double signs of hypocalcemia .
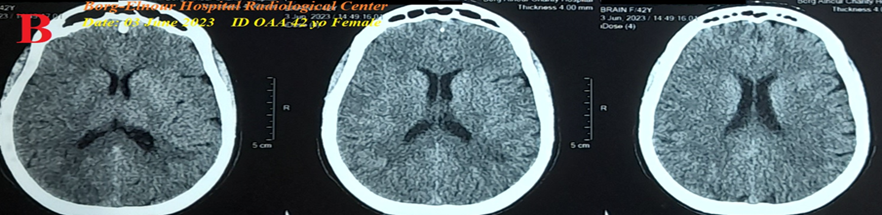
Figure 6B: There is laboratory hypocalcemia. Brain CT was normal .
Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with dramatic improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
Figure 6 A-ECG tracing on the day of the presentation shows the Wavy triple sign” in aVF and V6 leads (light blue, red, and green arrows) and the Wavy double sign” in lead II (red and green arrows). B-Brain CT sections were done on the second day of the presentation showing no abnormalities. Red arrows =elevated beats, green arrows = isoelectric beats, and blue arrows =depressed beats.
• Case No. 7: A 41-year-old married female housewife Egyptian patient was presented to the ICU after psychogenic stress with the left side weakness, ipsilateral body aches, ipsilateral facial weakness, hyperventilation, chest pain, and numbness. She was tested for latent tetany which was positive.
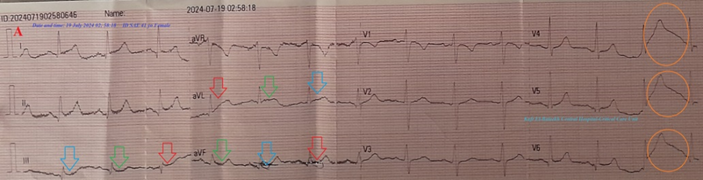
Figure 7A: ECG tracing showing Wavy triple sign, Tee-Pee sign, and Camel hump T-waves .

Figure 7B:There is no laboratory hypocalcemia. Brain CT was normal .
Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
Figure 7 A-ECG tracing on the day of the presentation shows Wavy triple sign” in III, aVL, and aVF leads (light blue, red, and green arrows), and Tee-Pee sign with Camel hump T-waves” in V4-6 leads (orange circles). B-Brain CT video section was done on the third day of the presentation showing no abnormalities. Green arrows = isoelectric beats, and blue arrows =depressed beats.
• Case No. 8: A 33-year-old married female housewife Egyptian patient was presented to the POC after psycho-familial troubles with left side weakness, ipsilateral body aches, and paresthesia. She was tested for latent tetany which was positive.
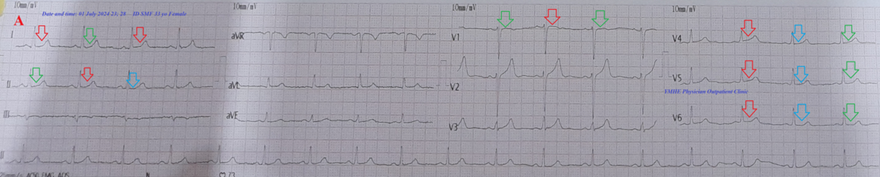
Figure 8A: ECG tracing shows Wavy triple and wavy double signs of hypocalcemia .
There is laboratory hypocalcemia. Brain CT was normal (Figure 8B).
Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
Figure 8 A-ECG tracing on the day of the presentation shows Wavy triple sign” in II and V4-6 leads (light blue, red, and green arrows) and Wavy double sign” in lead I and V1 (red and green arrows). B-Brain CT sections were done on the second day of the presentation showing no abnormalities. Red arrows =elevated beats, green arrows = isoelectric beats, and blue arrows =depressed beats.
• Case No. 9: A 34-year-old married worker female Egyptian patient was presented to the ED after psychogenic stress with left-side weakness, ipsilateral body aches, and numbness. She was tested for latent tetany which was positive.
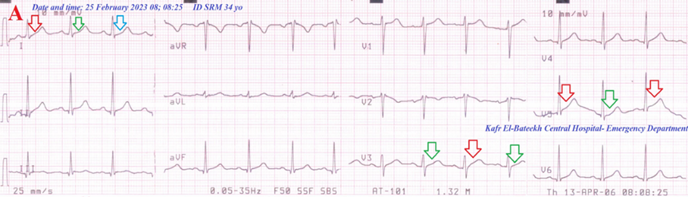
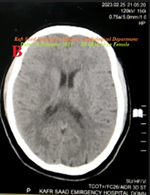
Figure 9B: ECG tracing shows Wavy triple and Wavy double signs of hypocalcemia.
Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
Figure 9 A-ECG tracing on the day of the presentation shows a Wavy triple sign” in lead I (light blue, red, and green arrows), and Wavy double sign” in lead I and V3, and V5 (red and green arrows). B-Brain CT video section was done on the second day of the presentation showing no abnormalities. Green arrows = isoelectric beats, and blue arrows =depressed beats.
• Case No. 10: A 27-year-old married female farmer Egyptian patient was presented to the POC after sadness with left side weakness, ipsilateral body aches, and paresthesia. She was tested for latent tetany which was positive.
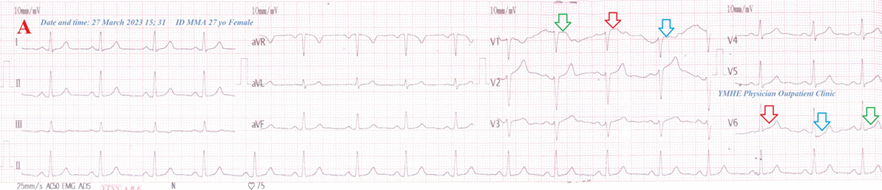
Figure 10B: ECG tracing shows a wavy triple sign of hypocalcemia .
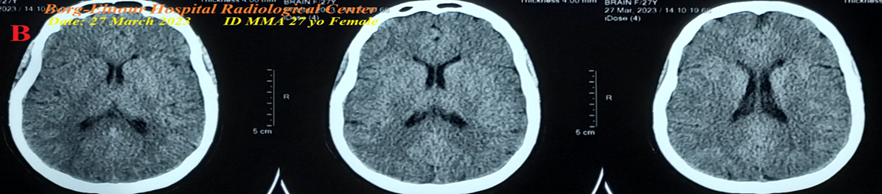
Figure 10B: There is laboratory hypocalcemia. Brain CT was normal .
Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
Figure 10 A-ECG tracing on the day of the presentation shows a Wavy triple sign” in V1 and V6 leads (light blue, red, and green arrows). B-Brain CT sections were done on the second day of the presentation show no abnormalities. Red arrows =elevated beats, green arrows = isoelectric beats, and blue arrows =depressed beats.
• Case No. 11: A 21-year-old married female housewife Egyptian patient was presented to the POC after psycho-familial troubles with left side weakness, ipsilateral body aches, ipsilateral facial weakness, tachypnea, and paresthesia. She was pregnant. She was tested for latent tetany which was positive. ECG tracing shows a double sign of hypocalcemia. There is laboratory hypocalcemia. Brain CT was not done due to pregnancy. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 12: A 25-year-old divorced female housewife Egyptian patient was presented to the ICU after psycho-familial troubles with left side weakness, ipsilateral body aches, and numbness. The same attack happened 17 months ago. She was tested for latent tetany which was positive. ECG tracing showed a Wavy triple sign of hypocalcemia. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 13: A 43-year-old married female housewife Egyptian patient was presented to the ICU after psycho-familial troubles with left side weakness, ipsilateral body aches, ipsilateral facial weakness, tachypnea, and paresthesia. She was tested for latent tetany which was positive ECG tracing showing a Wavy triple sign of hypocalcemia. There is laboratory hypocalcemia. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 14: A 35-year-old married male worker Egyptian patient presented to the ED after work troubles with left-side weakness, ipsilateral body aches, chest pain, and paresthesia. He was tested for latent tetany which was positive. ECG tracing showed a Wavy triple sign of hypocalcemia. Brain CT and brain MRI were normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 15: A 28-year-old married female housewife Egyptian patient presented to the POC after psycho-familial troubles with left-side weakness, ipsilateral body aches, and numbness. She was tested for latent tetany which was positive. ECG tracing showing Wavy triple sign, Tee-Pee sign, and Camel hump T-waves. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with dramatic improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 16: A 43-year-old married female housewife Egyptian patient was presented to the POC after psycho-familial troubles with left-side weakness, ipsilateral body aches, ipsilateral facial weakness, tachypnea, and tetany. ECG tracing showed a Wavy triple sign of hypocalcemia. There is laboratory hypocalcemia. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. Two IV calcium was initially given, and then an oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 17: A 65-year-old married housewife female Egyptian patient was presented to the POC after psycho-familial troubles with right-side weakness, ipsilateral body aches, ipsilateral facial weakness, and tetany. There is laboratory hypocalcemia. ECG tracing shows frequent PVCs. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. Two IV calcium was initially given then, an oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 18: A 40-year-old married female housewife Egyptian patient was presented to the POC after psycho-familial troubles with left-side weakness, ipsilateral body aches, ipsilateral facial weakness, tachypnea, and paresthesia. She was tested for latent tetany which was positive. ECG tracing showed a Wavy triple sign of hypocalcemia. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 19: A 40-year-old married female housewife Egyptian patient was presented to the ICU after sadness with left-side weakness, ipsilateral body aches, and numbness. She was tested for latent tetany which was positive. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 20: A 25-year-old married female housewife Egyptian patient was presented to the POC after psycho-familial troubles with left upper limb weakness, ipsilateral body aches, ipsilateral facial weakness, tachypnea, chest pain, and numbness. She was tested for latent tetany which was positive. ECG tracing showed a Wavy triple sign of hypocalcemia. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 21: A 36-year-old married male sweet worker Egyptian patient was presented to the ICU after sadness with left side weakness, ipsilateral body aches, ipsilateral facial weakness, and paresthesia. He was tested for latent tetany which was positive. ECG tracing and brain CT were normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 22: A 37-year-old married female housewife Egyptian patient was presented to the POC after stress with left side weakness, ipsilateral body aches, ipsilateral facial weakness, and paresthesia. She was tested for latent tetany which was positive. ECG tracing and brain CT were normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with dramatic improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 23: A 19-year-old single male student Egyptian patient was presented to the POC after psychological stress with left side weakness, ipsilateral body aches, ipsilateral facial weakness, and numbness. He was tested for latent tetany which was positive. ECG tracing showed a Wavy triple sign of hypocalcemia. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 24: A 29-year-old married female farmer Egyptian patient was presented to the POC after psycho-familial troubles with left side weakness, ipsilateral body aches, ipsilateral facial weakness, tachypnea, and tetany. ECG tracing shows a Wavy double sign of hypocalcemia. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. Two IV calcium were initially, given then an oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 25: A 34-year-old married female teacher Egyptian patient was presented to the POC after sadness with left side weakness, ipsilateral body aches, ipsilateral facial weakness, tachypnea, and paresthesia. She was tested for latent tetany which was positive. ECG tracing showed a wavy triple sign of hypocalcemia. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 26: A 42-year-old married female farmer Egyptian patient was presented to the POC after psychological stress with left side weakness, ipsilateral body aches, ipsilateral facial weakness, tachypnea, and paresthesia. She was tested for latent tetany which was positive. ECG tracing shows a wavy triple sign of hypocalcemia. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 27: A 35-year-old married male farmer Egyptian patient was presented to the POC after sadness with left upper limb weakness, ipsilateral body aches, and paresthesia. The weakness suddenly reversed to the right lower limb. He was tested for latent tetany which was positive. ECG tracing shows a wavy triple sign of hypocalcemia with a repolarization pattern. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 28: A 16-year-old single female student Egyptian patient was presented to the POC after psychological stress with left-side weakness, ipsilateral facial weakness, tachypnea, palpitations, and paresthesia. She was tested for latent tetany which was positive. ECG tracing shows a Wavy triple sign of hypocalcemia and sinus tachycardia. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with dramatic improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 29: A 50-year-old married female housewife Egyptian patient was presented to the POC after sadness with left side weakness, ipsilateral body aches, ipsilateral facial weakness, dysarthria, and paresthesia. She was tested for latent tetany which was positive. ECG tracing and brain CT were normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with dramatic improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 30: A 47-year-old married female housewife Egyptian patient was presented to the POC after stress with left side weakness, ipsilateral body aches, ipsilateral facial weakness, tachypnea, and paresthesia. She was tested for latent tetany which was positive. ECG tracing shows a Wavy triple sign of hypocalcemia. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with dramatic improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
• Case No. 31: A 34-year-old married female teacher Egyptian patient was presented to the POC after psychological stress with left side weakness, ipsilateral body aches, ipsilateral facial weakness, tachypnea, and paresthesia. She was tested for latent tetany which was positive. ECG tracing showed a Wavy triple sign of hypocalcemia. Brain CT was normal. Yasser’s sphygmomanometer procedure was applied in both the left upper and lower extremities with a dramatically improving response. Complete clinical recovery had happened. An oral calcium-vitamin D tab was prescribed for two weeks.
A total of 31 patients are included in this study. There is female sex predominance; 87.1% (n: 27) vs. 12.9% (n = 4) of the male patients. The mean age of the cases was 35.29 years (range; 16-65). The most commonly associated hemiplegia in the study was the left-side hemiplegia of the cases; 90.32% (n: 28) vs. right-side hemiplegia; 6.45% (n = 2) and reversal hemiplegia; 3.23% (n: 1). Latent tetany was the most predominant tetany; 90.32% (n: 28) vs. the manifested; 9.68% (n = 3). Wavy triple sign represents the most frequent sign in the ECG; 35.48% (n: 11) vs. Wavy double sign; 22.58% (n: 7), combined Wavy triple sign and Wavy double sign; 16.13% (n: 5), Wavy triple sign with Tee-Pee sign and Camel hump T-waves; 6.45% (n: 2), sinus tachycardia with Wavy triple sign; 3.23% (n: 1), Premature ventricular complexes; 3.23% (n: 1), normal; 9.68% (n: 3), and unavailable ECG; 3.23% (n: 1). Laboratory hypocalcemia for ionized calcium were detected in 32.26% (n: 10). The response to the Yasser’s Sphygmomanometer Maneuver was 100%, but there was recurrence for one case (Case No. 5) after about 17 months. The most common occupations in the study were a housewife; 54.84% (17), farmer; 16.13% (n: 5), worker; 9.68% (n: 3), teacher; 9.68% (n: 3), student; 6.45% (n: 2), and employee; 3.23% (n: 1) (Figure 2 and 3).
| Case No. | Age/y | Sex | Occupation | Pulse/ bpm | BP /mmHg | Temp/C | RR/ bpm | O2 Sat/% | Tetany | ECG
| Ionized Ca++ | Hemiplegia | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SBP | DBP | ||||||||||||
| 1 | 42 | F | Teacher | 70 | 130 | 70 | 36 | 16 | 97 | Latent | WTS | 4.24 mg/dl | Left |
| 2 | 29 | F | Housewife | 95 | 100 | 80 | 37 | 19 | 99 | Latent | WTS+WDS | 3.79mg/dl | Left |
| 3 | 37 | F | Employee | 70 | 100 | 70 | 36.5 | 15 | 97 | Latent | WDS | UA | Left |
| 4 | 42 | F | Housewife | 66 | 110 | 60 | 36 | 14 | 95 | Latent | WDS | UA | Left |
| 5 | 23 | F | Housewife | 86 | 140 | 90 | 37 | 20 | 99 | Latent | WTS+WDS | 0.66 mmol/l | Left |
| 6 | 42 | F | Housewife | 82 | 110 | 70 | 37 | 21 | 96 | Latent | WTS+WDS | 4.3 mg/dl | Right |
| 7 | 41 | F | Housewife | 83 | 120 | 80 | 36.6 | 22 | 95 | Latent | WTS+TPS+CHTS | 1.32mmol/l | Left |
| 8 | 33 | F | Housewife | 80 | 110 | 70 | 36 | 17 | 97 | Latent | WTS+WDS | 1.1 mmol/l | Left |
| 9 | 34 | F | Worker | 93 | 130 | 80 | 80 | 19 | 99 | Latent | WTS+WDS | UA | Left |
| 10 | 27 | F | Farmer | 74 | 140 | 80 | 37 | 16 | 99 | Latent | WTS | 1mmol/l | Left |
| 11* | 21 | F | Housewife | 65 | 140 | 70 | 36 | 24 | 97 | Latent | WDS | 3.76mg/dl | Left |
| 12 | 25 | F | Housewife | 71 | 110 | 70 | 36 | 18 | 96 | Latent | WTS | 4.29 mg/dl | Left |
| 13 | 43 | F | Housewife | 80 | 100 | 80 | 36 | 18 | 95 | Latent | WTS | 0.57 mmol/l | Left |
| 14 | 35 | M | Worker | 80 | 100 | 60 | 37 | 18 | 98 | Latent | WTS | UA | Left |
| 15 | 28 | F | Housewife | 74 | 110 | 70 | 36.7 | 21 | 99 | Latent | WTS+TPS+CHTS | UA | Left |
| 16 | 43 | F | Housewife | 65 | 140 | 70 | 36 | 24 | 97 | Manifested | WDS | UA | Left |
| 17 | 65 | F | Housewife | 86 | 130 | 80 | 37.5 | 22 | 95 | Manifested |
| UA | Right |
| 18 | 40 | F | Housewife | 76 | 130 | 90 | 36.5 | 16 | 99 | Latent | WDS | UA | Left |
| 19 | 40 | F | Housewife | 88 | 120 | 70 | 37 | 18 | 98 | Latent | UA | UA | Left |
| 20 | 25 | F | Housewife | 76 | 130 | 80 | 36 | 20 | 95 | Latent | WDS | UA | Left |
| 21 | 36 | M | Worker | 70 | 120 | 80 | 37.5 | 14 | 98 | Latent | Normal | UA | Left |
| 22 | 37 | F | Housewife | 98 | 100 | 70 | 36 | 16 | 95 | Latent | Normal | UA | Left |
| 23 | 19 | M | Student | 70 | 130 | 70 | 36 | 17 | 99 | Latent | WTS | UA | Left |
| 24 | 29 | F | Farmer | 68 | 90 | 70 | 36.5 | 22 | 97 | Manifested | WDS | UA | Left |
| 25 | 34 | F | Teacher | 72 | 100 | 60 | 37 | 23 | 99 | Latent | WTS | UA | Left |
| 26 | 42 | F | Farmer | 84 | 130 | 80 | 36 | 25 | 95 | Latent | WTS | UA | Left |
| 27 | 35 | M | Farmer | 80 | 140 | 80 | 36 | 18 | 96 | Latent | WTS | UA | Reversed |
| 28 | 16 | F | Student | 125 | 140 | 70 | 37 | 20 | 97 | Latent | WTS+ST | UA | Left |
| 29 | 50 | F | Farmer | 67 | 120 | 80 | 36.5 | 24 | 97 | Latent | Normal | UA | Left |
| 30 | 47 | F | Housewife | 97 | 130 | 80 | 37 | 21 | 95 | Latent | WTS | UA | Left |
| 31 | 34 | F | Teacher | 94 | 120 | 90 | 37 | 17 | 99 | Latent | WTS | UA | Left |
Table 2: Summary of the history, clinical, and management data; (n: 31)
Abbreviations: BP; Blood pressure, Ca++: Calcium, CHTW: Camel hump T-waves, DBP; Diastolic blood pressure, F; Female, Male; Male, PVCs: Premature ventricular complexes, SBP; Systolic blood pressure, RR: Respiratory rate, ST: Sinus tachycardia, TPS: Tee-Pee sign, UA: Unavailable, WDS; Wavy double sign, WTS; Wavy triple sign
*: Pregnant
| Variable | Numbers | % | Range | Means |
| Age | - | - | 16-65 | 35.29 |
Sex Female Male | 27 4 | 87.1 12.9 | - | - |
Type of hemiplegia Left Right Reversed |
28 2 1 |
90.32 6.45 3.23 | -
| -
|
Tetany Latent Manifested |
28 3 |
90.32 9.68 | - | - |
ECG WTS WDS WTS+WDS WTS+TPS+CHTS WTS+ST PVCs Normal UA |
11 7 5 2 1 1 3 1 |
35.48 22.58 16.13 6.45 3.23 3.23 9.68 3.23 | - | - |
| Laboratory hypocalcemia | 10 | 32.26 | - | - |
Table 3: Statistical summary of age, sex, type of hemiplegia, tetany, ECG, and laboratory hypocalcemia; (n: 31)
Abbreviations: Camel hump T-waves, PVCs: Premature ventricular complexes, ST: Sinus tachycardia, TPS: Tee-Pee sign, UA: Unavailable, WDS; Wavy double sign, WTS; Wavy triple sign
• Age;
• Range; 16-65, Minimal; 16, Maximal; 65, Mean; 35.29, Median: 35, and Mode: 42 (Tables 2 and 3).
• Sex;
• Female sex; 87.1% (27 cases).
• Male sex; 12.9% (4 cases) (Figure 11A)
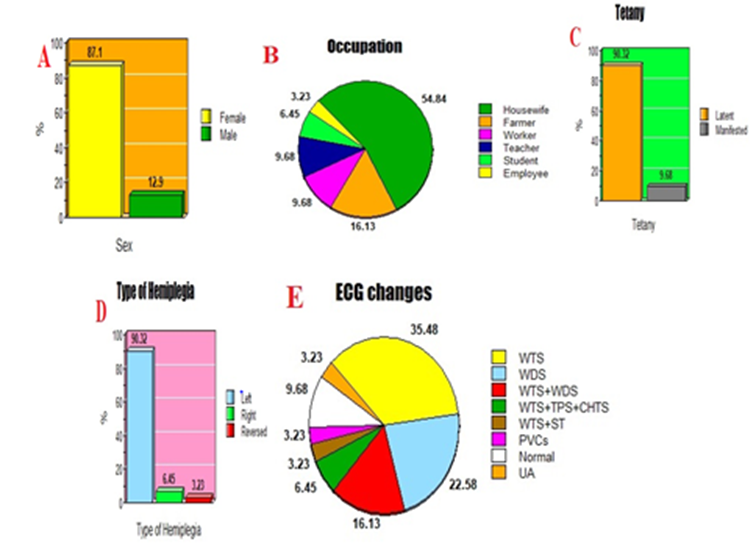
Figure 11: A. Bar presentation of sex in the study. B. Pie presentation of occupation in the study. C. Bar presentation of tetany in the study. D. Bar presentation of the type of hemiplegia in the study. E. Pie presentation of ECG changes in the study.
• Occupation
• Housewife; 54.84% (17 cases)
• Farmer; 16.13% (5 cases)
• Worker; 9.68% (3 cases)
• Teacher; 9.68% (3 cases)
• Student; 6.45% (2 cases)
• Employee; 3.23% (1 case) (Table 3) (Figure 11B).
• Tetany
• Latent; 90.32% (28 cases)
• Manifested; 9.68% (3 cases) (Table 3) (Figure 11C).
• Type of hemiplegia
• Left; 90.32% (28 cases)
• Right; 6.45% (2 cases)
• Reversed; 3.23% (1 case) (Table 3) (Figure 11D).
• ECG changes
• WTS; 35.48% (11 cases)
• WDS; 22.58% (7 cases)
• WTS+WDS; 16.13% (5 cases)
• WTS+TPS+CHTS; 6.45% (2 cases)
• WTS+ST; 3.23% (1 case)
• PVCs; 3.23% (1 case)
• Normal; 9.68% (3 cases)
• UA; 3.23% (1 case) (Table 3) (Figure 11E).
• Response
• Application; 100% (31 cases) (Table 2).
4.1 Past studies
Depending on the past literature publications, there were interesting case report series and a single study for psychogenic hemiplegia (1994-2020). Haghighi SS (2019) [18] reported one case that has been presented with psychogenic hemiplegia secondary to cervical spine discectomies and fusion reversed by rehabilitation. Haghighi SS and Meyer S (2001) [22] reported a case of psychogenic paraplegia following a motor vehicle accident reversed by treatment of depression and conversion disorder. Morota N et al. (1994) [23] reported a case of a 12-year-old girl presented with psychogenic quadriparesis after undergoing surgical repair of a recurrent syringomyelia that was fully recovered within 1 month by rehabilitation. N Chastan and D Parain (2010) [31] studied 70 patients of psychogenic paralysis and recovery after motor cortex transcranial magnetic stimulation. Berhane L et al. (1998) [25] reported a case of recurrent psychogenic paraplegia following gynecologic laparoscopy reversed with treatment of conversion disorder. Ito A. et al. (2020) [32] reported an unusual case of postoperatively psychogenic tetraplegia the patient spontaneously fully recovered within 12 hours. Shell MG et al. (1997) [24] reported a case of paraplegia presented in a patient with an implantable morphine pump and an epidural abscess with treatment of conversion disorder primarily supportive, focused on consistency and behavioral management. Laraki M et al. (1996) [27] reported a case of hysterical paraplegia in a 15-yr-old, 45-kg girl, transiently after epidural anesthesia and the patient spontaneously fully recovered within 6 days. (Table 4)
| Study | Year | Sex | Primary disorder | Secondary trigger | Reversal | Reference |
1. Haghighi SS
| 2019
| F
| Psychogenic hemiplegia
| Cervical spine discectomies and fusion | Rehabilitation
| 18 |
2. Haghighi SS and Meyer S
| 2001
| F
| Psychogenic paraplegia
| Motor vehicle accident
| Treatment of depression and conversion disorder | 22
|
3. Morota N et al.
| 1994
| F
| Psychogenic quadriparesis
| Surgical repair of a recurrent syringomyelia
| Rehabilitation
| 23
|
4. N Chastan and D Parain
| 2010
| 44 F/26 M
| Paraparesis
| Psychosocial event or a physical injury
| Motor cortex transcranial magnetic stimulation
| 31
|
5. Berhane L et al.
| 1998
| F
| Paraplegia
| Gynecologic laparoscopy
| Treatment of conversion
| 25
|
6. Ito A et al.
| 2020
| F
| Tetraplegia
| Postoperative
| Spontaneous recovery
| 32
|
7. Shell MG et al.
| 1994
| F
| Paraplegia
| Implantable morphine pump and an epidural abscess | Supportive
| 24
|
8. Laraki M et al.
| 1996
| F | Paraplegia | Epidural anesthesia | Spontaneous recovery
| 27 |
Table 4: Past studies for psychogenic coma from 1994 to 2020.F;
Female; M; Male
4.2 The procedure description
• Preparation:
• Indications:
• Psychogenic hemiplegia. The author depended in a diagnosis of psychogenic hemiplegia on the presence of limb weakness, painful paralyzed extremity, ipsilateral facial numbness or paresthesia with or without facial weakness, normal Glasgow Coma Scale (GCS), and normal brain CT scan. Follow up for at least for 48 hours post recovery with Yasser’s Sphygmomanometer Procedure.
• Principal and Interpretations:
• Pressuring of the cuff of the sphygmomanometer on inflation may produce an obstructive power at the distal to the compressive site and another transmission power at the proximal to the compressive site. Distal power may be due to compression of local blood arteries resulting in decreasing blood flow to the paralyzed limb inducing some increasing pain over the present pain stimulating the local nerves to produce trial to the movement of this limb. Local hypocalcemia for the paralyzed limb due to this local obstruction may also be a suggestive theory for this pain. On contradictory, the proximal power to the compressive site may be due to transient increasing the diameter of the proximal local blood arteries to the compressive cuff while increasing the blood flow to the proximal area in the paralyzed limb also may be stimulant for the local nerves to produce trial to the movement of this limb. The author thinks that distal power is stronger than the proximal power (red and lime arrows)

Figure 12: The author caricaturing a diagram for Yasser’s sphygmomanometer procedure in the management of psychogenic hemiplegia.
• Target:
• The maneuver and response:
• Advantages:
• Disadvantages:
• Contraindication:
4.3 Limitations of the study:
There are no conflicts of interest.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.



























































