
Research Article | DOI: https://doi.org/10.31579/2688-7517/072
1Department of spine surgery, Ningxia Medical University General Hospital, 804 Shengli Street, Xingqing District, Ningxia 75004, China.
2The First Clinical Medical College of Ningxia Medical University, Ningxia, 750004, China.
3Hainan District People's Hospital, WuHai City, Inner Mongolia,016030,China.
4WuHai People's Hospital, Inner Mongolia,016030,China.
5The Efficacy of Arthroscopic Tie-Knot Technique Versus Suture Bridge Technique in The Treatment of Anterior Cruciate Ligament Tibial Insertion Avulsion Fractures.
*Corresponding Author: Haifeng Yuan, The Efficacy of Arthroscopic Tie-Knot Technique Versus Suture Bridge Technique in The Treatment of Anterior Cruciate Ligament Tibial Insertion Avulsion Fractures.
Citation: Zhe Liu, Jing Guo, Donghui Cao, Xiao Zhang Haoxin Li, et al, (2025), The Efficacy of Arthroscopic Tie-Knot Technique Versus Suture Bridge Technique in The Treatment of Anterior Cruciate Ligament Tibial Insertion Avulsion Fractures, J. Addiction Research and Adolescent Behaviour, 8(3) DOI:10.31579/2688-7517/072.
Copyright: © 2025, Haifeng Yuan. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 November 2025 | Accepted: 19 November 2025 | Published: 28 November 2025
Keywords: anterior cruciate ligament; tibial fracture; knee injury; arthroscopy; fracture fixation surgery
This study compared the surgical outcomes and postoperative recovery of the Tie - knot and Suture Bridge techniques for ACL tibial insertion avulsion fractures over a 5 - year follow - up. Ninety patients were divided into two groups based on the fixation method. Pre - operative general data showed good comparability. The Suture Bridge group had a longer surgical duration. One month post - surgery, it had better VAS, IKDC, Lysholm scores, ROM, and KT - 1000 results. However, from 6 months to 5 years post - operation, no significant differences were found. No postoperative complications were observed in either group. Both techniques are safe and effective. The Suture Bridge technique offers better early pain relief and functional recovery, but long - term effects are comparable. Future research could focus on optimizing these techniques.
Avulsion fracture of the anterior cruciate ligament (ACL) tibial insertion refers to a fracture at the site where the ACL attaches to the tibia and is one of the common knee joint injuries. Reports suggest that the annual incidence is approximately 0.0003%[1], accounting for 3%-5% of knee joint injuries, and there has been an upward trend in its occurrence over the years[2]. This kind of injury usually occurs in high-energy traumas such as traffic accidents or sports-related injuries[3], which can cause the loss of ACL tension and disrupt the dynamic stability of the knee joint. If left untreated, it may lead to malunion of the fracture, intercondylar impaction, cartilage damage, knee joint fibrosis, accelerated degenerative changes in the joint, and ultimately result in knee osteoarthritis, severely affecting the patient's daily life. In 1959, Meyers and McKeever[5] classified ACL tibial insertion avulsion fractures. Due to the limitations of the equipment at that time, the classification was solely based on the degree of displacement of the fracture fragment shown on X-rays. Later, Green6 and others established a new classification system based on MRI findings, providing specific quantitative criteria. However, the Meyers-McKeever classification is still used as a clinical guide. For Meyers-McKeever Type I fractures, conservative treatments like limb immobilization and plaster fixation are generally employed. Type IV fractures, because of the severe comminution of the fracture fragments, along with postoperative bone loss and joint fluid infiltration leading to nonunion and fixation failure, require ACL reconstruction surgery, which not only impacts the patient's physical and mental well-being but also increases the economic burden. Therefore, in clinical practice, fracture fixation surgeries are mostly carried out on Type II and Type III fractures. Traditional surgical methods involve open exposure, reduction, and fixation, which cause greater tissue trauma, increase the risk of infection, and are also restricted by the size of the fracture fragments7. If the fragments are too small, screw fixation cannot be used, and drilling holes for screw insertion leads to bone loss. Additionally, the process of screw compression poses a risk of fragment comminution. As a result, some surgeons have used steel wires and staple fixation, but all internal fixation devices need to be surgically removed, further increasing the physical, psychological, and economic burden on the patient8. Due to these limitations, traditional open reduction techniques have largely been abandoned. In recent years, with the widespread adoption of the minimally invasive concept, arthroscopic technology has become the gold standard for treating Type II and III ACL tibial insertion avulsion fractures, thanks to its advantages of minimal trauma, fewer complications, and faster recovery. Arthroscopic technology mainly utilizes internal fixation materials such as sutures, anchors, and looped titanium plates8–11. Sutures are flexible and compatible with the joint cavity, making them a core internal fixation material in arthroscopic surgery. Anchors combine the advantages of both screws and sutures and have been widely used as new fixation materials for ligament and avulsion fractures. Loop plates offer good resistance to reverse tensile forces and are primarily used in ligament reconstruction surgeries. The suture bridge technique involves arthroscopically creating bone tunnels, using sutures to loop the avulsion fracture fragment and tying a knot at the exit of the tunnel, similar to a "tie-knot" structure. This technique is easy to perform, shortens the surgical time, and is widely accepted by sports medicine surgeons. The suture bridge technique creates a "bridge" structure using internal and external screws along with sutures to cover and stabilize the bone fragment, making it especially suitable for smaller, comminuted fracture fragments that cannot be fixed with screws. Although prior studies have verified the clinical effectiveness of both techniques, there is currently a dearth of long-term research that directly compares the efficacy of these two techniques. Thus, this study retrospectively examined the clinical data of 90 patients with ACL tibial insertion avulsion fractures, contrasting the clinical outcomes of the arthroscopic suture bridge technique and the tie-knot technique, and offering a reference for the selection of surgical approaches in clinical practice.
This study was approved by the institutional ethics committee (1503022015005). Informed consent was obtained from all participants before they were included in the study. A retrospective analysis was carried out on 90 patients who had undergone arthroscopic treatment for ACL tibial insertion avulsion fractures using the tie-knot technique and the suture bridge technique at our hospital between April 2015 and August 2020. The inclusion and exclusion criteria were as follows:
Inclusion criteria:
Diagnosis of ACL tibial insertion avulsion fracture was confirmed by X-ray, CT, and MRI. Meyers-McKeever classification Type II or Type III. Age of 16 years or older. Time from injury to surgery less than 2 weeks Complete follow-up data.
Exclusion criteria:
Associated injuries such as damage to other ligaments or tibial plateau fractures.
Open fractures or associated skin or joint infections.
Pathological fractures.
Previous knee surgery or a history of knee osteoarthritis.
Follow-up duration less than 5 years or patients who did not follow the required follow-up schedule.
Surgical Protocol
All surgical procedures were carried out by the same senior attending surgeon. Epidural anaesthesia was administered to all patients, who were positioned in a supine posture. A standard arthroscopic method was employed, utilizing anterior medial and anterolateral portals. The intra-articular hematoma was removed, and the joint was thoroughly flushed with saline. The ligaments, meniscus, and cartilage within the joint were inspected, and requisite repairs were carried out. The avulsed fracture fragment and the tibial bone bed were exposed, and blood clots and fibrous tissue were cleared using a rasp and a small curette. The fracture site was freshened up, and the surrounding soft tissues and meniscus were mobilized with a probe to aid in achieving an anatomical reduction of the fracture fragment.
TK Group (Figure 1):
The surgical technique involved using Ultrabraid sutures to encircle and secure the avulsed fracture fragment at the ACL base, creating a "tie-knot" configuration. Depending on the fragment size, an Arthrex ACL tibial locator guided the placement of two 2mm Kirschner wires slightly posterior to the fracture bed, typically at the 3 o'clock and 9 o'clock positions inside the joint. This ensured the proximal tibial entry points were spaced at least 1 cm apart, forming a double bone tunnel. After removing the Kirschner wires, an epidural puncture needle facilitated the passage of a PDS II suture through the tunnel, followed by the Ultrabraid suture tail. A small curette or probe aided in reducing and compressing the fracture fragment, while the suture tail was tightened and tied externally to complete the reduction and fixation.
SB Group (Figure 2):
The fractured fragment was elevated using anteromedial and anterolateral approaches. Through the plate method, one 4.5mm absorbable double-strand suture anchor was placed at the 10 o'clock and 2 o'clock positions of the tibial fracture bed. A suture hook was then used to pass the suture through the anterior cruciate ligament (ACL) tissue at the proximal bone fragment. After reducing the fracture fragment with assistance from a small curette or probe, a 4.75mm absorbable suture anchor was positioned on the anterolateral side of the fracture bed, and its suture tail was tightened and secured. A similar process was performed to tighten and fix the suture tails from the lateral suture anchor. Ultimately, an X-shaped suture bridge was created between the internal and external suture anchors. The external suture anchors were generally positioned at the 4 o'clock and 8 o'clock positions, with adjustments made based on the extent of fragment displacement.
Postoperative Management and Rehabilitation Protocol
After completing the fixation of the fractured fragment, the surgeon assessed the tension restoration of the anterior cruciate ligament (ACL) using a probe. The knee joint was then flexed and extended to verify the stability of the fracture fixation and rule out any intercondylar impingement. Anatomical reduction of the fracture was confirmed via X-ray fluoroscopy, after which the incision was sutured and covered with sterile dressings followed by compressive bandaging. An adjustable knee immobilizer was applied to maintain the affected limb in extension. Post-anesthesia recovery included early initiation of ankle pump exercises and quadriceps training. During the initial two postoperative weeks, the knee was kept extended, followed by a gradual weekly increase in flexion by 30 degrees. For the first four weeks, patients used a brace and crutches for non-weight-bearing ambulation. Partial weight-bearing walking with assistive devices began by the eighth week, progressively increasing over the next two weeks until full weight-bearing was achieved by the tenth postoperative week, at which point assistive devices were discontinued12.
Observation Indicators
We compared various parameters between the two groups to identify any statistical differences. These included basic demographic information such as gender, age, injured side, and fracture type (classified according to the Meyers-McKeever system). We also analyzed surgical duration, length of hospital-stay, and fracture healing time. Patient outcomes were assessed using multiple measures: pain levels via the Visual Analog Scale (VAS)13, knee function through the International Knee Documentation Committee (IKDC) 14and Lysholm scales15, range of motion (ROM), and knee stability measured by KT-100016. These evaluations were conducted at several time points: before surgery and during follow-up visits at 1 month, 6 months, 1 year, 2 years, 3 years, and 5 years after the operation.
Statistical Processing
This study conducted all statistical analyses using IBM SPSS 27.0 software. Initially, we assessed data normality through the Shapiro-Wilk test, followed by evaluating variance homogeneity with Levene's test. For normally distributed data with equal variances, results are expressed as mean ± standard deviation. Within-group comparisons across different time points (pre-operative, 1 month, 6 months, 1 year, 2 years, 3 years, and 5 years post-operative) were performed using paired T-tests, while between-group comparisons employed independent sample t-tests. Statistical significance was defined as P less than 0.05.
The study found no significant differences between the two groups regarding gender, age, injured side, Meyers-McKeever classification, hospital stay duration, fracture healing time, or follow-up period (P>0.05), indicating strong baseline comparability (Table 1). Both groups were monitored for at least 5 years (60 months), with the tie-knot group averaging 77.88 ± 15.174 months (range: 60–113 months) and the suture bridge group averaging 73.35 ± 14.213 months (range: 60–113 months). Notably, the suture bridge group required significantly longer surgical times than the tie-knot group (P<0>0.05, Tables 2–4).

Figure 1: Tie-knot Group Surgical Procedure: a. Clear the hematoma around the fracture fragment. b. Use a curette to deepen the bone bed. c. Position the tibial locator and prepare the lateral bone tunnel. d. Prepare the medial bone tunnel. e. Suture the proximal fragment's substantial part. f. Reduce the fracture fragment and tie the knot at the bone tunnel exit. g. Illustration of the tie-knot technique.

Figure 2: Suture-Bridge Group Surgical Procedure: a. Freshen the fracture fragment and deepen the bone bed. b. Position, prepare the 4.5mm reamer and tap for the screw hole. c. Screw in the posterior medial anchor. d. Screw in the posterior lateral anchor. e. Suture the substantial part of the proximal fragment. f. Reduce the fracture fragment and perform pressure fixation with a 4.75mm cancellous anchor. g. Postoperative imaging. h. Illustration of the suture-bridge technique.
| TK group(n=42) | SB group(n=48) | t/χ2 | P | |
| Age (y) | 34.40±7.768 | 34.04±9.107 | 0.202 | 0.840 |
| Gender (n(%)) | 1.087 | 0.956 | ||
| Male | 23(25.56%) | 26(28.89%) | ||
| Female | 19(31.67%) | 22(24.44%) | ||
| Injured side(n(%)) | 1.087 | 0.302 | ||
| Left | 23(25.56%) | 21(23.33%) | ||
| Right | 19(31.67%) | 27(30.00%) | ||
| Cause of injury (n(%)) | 1.531 | 0.459 | ||
| Traffic Accident | 18(20.00%) | 15(16.67%) | ||
| Sport injury | 13(14.44%) | 20(22.22%) | ||
| Injury to other parts | 11(12.22%) | 13(14.44%) | ||
| Meyers-Mckeever classification (n (%)) | 0.001 | 0.977 | ||
| Type II | 27(30.00%) | 31(34.44%) | ||
| Type III | 15(16.67%) | 17(18.89%) | ||
| Meniscus injury (n (%)) | 0.009 | 0.925 | ||
| YES | 11(12.22%) | 13(14.44%) | ||
| NO | 31(34.44%) | 35(38.89%) | ||
| Operation Time(min) | 55.57±10.371 | 68.04±8.168 | -6.373 | < 0> |
| Hospital Stay(d) | 8.14±1.336 | 7.73±1.364 | 1.449 | 0.151 |
| Fracture healing Time(w) | 8.57±1.451 | 7.81±1.511 | 2.422 | 0.018 |
| Follow-up Time(mon) | 77.88±15.174 | 73.35±14.213 | 1.461 | 0.456 |
Table 1: Comparison of general date between the two groups(n=90, t/χ2)
TK group: Patients were treated with the joint arthroscopic tie knot technique; SB group: Patients were treated with the joint arthroscopic suture bridge technique. y: years; min: minutes. d: days. w: weeks; mon: months
| TK group | SB group | t | P | Cohen d | ||||
| VAS | ||||||||
| Pre-op | 7.76±0.850 | 7.75±0.812 | 0.068 | 0.946 | ||||
| Post-op 1m | 2.76±0.617 | 2.42±0.539 | 2.832 | 0.006 | 0.577 | |||
| Post-op 6m | 0.36±0.485 | 0.48±0.505 | -1.165 | 0.247 | 0.496 | |||
| Post-op 1y | 0.10±0.297 | 0.10±0.309 | -0.139 | 0.890 | 0.303 | |||
| Post-op 2y | 0.07±0.261 | 0.17±0.337 | -1.375 | 0.173 | 0.328 | |||
| Post-op 3y | 0.21±0.415 | 0.21±0.410 | 0.068 | 0.946 | 0.413 | |||
| Post-op 5y | 0.19±0.455 | 0.19±0.357 | 0.521 | 0.603 | 0.405 | |||
| IKDC | ||||||||
| Pre-op | 41.36±1.872 | 41.15±1.856 | 0.537 | 0.593 | ||||
| Post-op 1m | 66.81±2.308 | 68.21±1.529 | 0.010 | 0.001 | 1.932 | |||
| Post-op 6m | 92.95±0.882 | 82.82±0.895 | 0.911 | 0.850 | 0.889 | |||
| Post-op 1y | 94.60±1.308 | 94.90±1.547 | -0.988 | 0.326 | 1.440 | |||
| Post-op 2y | 98.00±0.937 | 98.29±1.010 | -1.414 | 0.161 | 0.977 | |||
| Post-op 3y | 98.57±0.703 | 98.85±0.743 | -1.846 | 0.068 | 0.725 | |||
| Post-op 5y | 99.02±0.749 | 99.10±0.751 | -0.507 | 0.613 | 0.750 | |||
Table 2: Comparison of VAS scores and IKDC scores of the two groups
VAS: Visual Analogue Scale scores; IKDC: International Knee Documentation Committee scores; m: months; y: years.
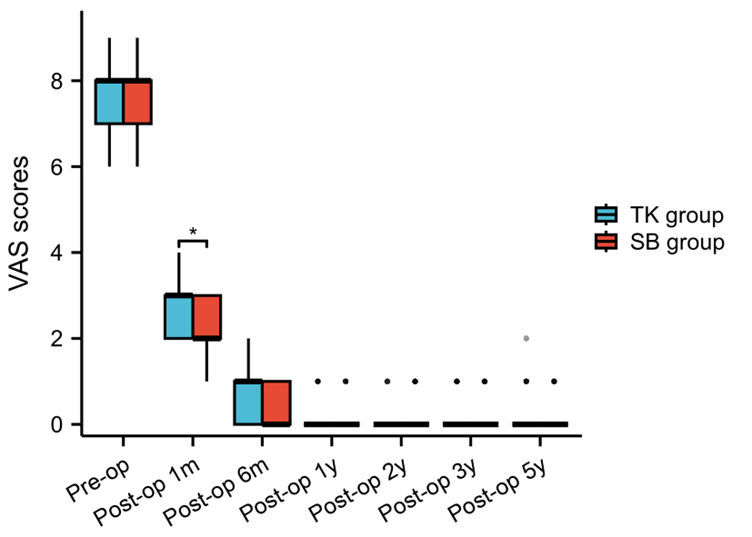
Figure 3: Comparison of VAS scores between TK group and SB group

Figure 4: Comparison of IKDC scores between TK group and SB group
| TK group | SB group | t | P | Cohen d | |
| Lysholm | |||||
| Pre-op | 43.40±1.939 | 43.15±1.856 | 0.537 | 0.593 | |
| Post-op 1m | 73.71±1.812 | 74.88±1.953 | 0.010 | 0.001 | 1.888 |
| Post-op 6m | 94.88±0.832 | 94.83±0.930 | 0.911 | 0.850 | 0.886 |
| Post-op 1y | 94.60±1.308 | 94.90±1.547 | -0.988 | 0.326 | 0.808 |
| Post-op 2y | 98.00±0.937 | 98.29±1.010 | -1.414 | 0.161 | 0.885 |
| Post-op 3y | 98.57±0.703 | 98.85±0.743 | -1.846 | 0.068 | 0.881 |
| Post-op 5y | 99.02±0.749 | 99.10±0.751 | -0.507 | 0.613 | 0.782 |
| ROM ( °) | |||||
| Pre-op | 58.74±2.025 | 58.15±2.010 | 1.390 | 0.168 | |
| Post-op 1m | 86.12±2.481 | 87.63±2.826 | -2.669 | 0.009 | 2.671 |
| Post-op 6m | 125.05±0.909 | 125.08±0.846 | -0.193 | 0.847 | 0.876 |
| Post-op 1y | 128.90±0.850 | 129.10±0.692 | -1.227 | 0.223 | 0.769 |
| Post-op 2y | 133.86±0.843 | 133.65±0.911 | 1.137 | 0.259 | 0.880 |
| Post-op 3y | 134.38±0.492 | 134.42±0.498 | -0.341 | 0.734 | 0.495 |
| Post-op 5y | 134.43±0.501 | 134.40±0.494 | 0.312 | 0.756 | 0.497 |
Table 3: Comparison of Lysholm scores and ROM of the two groups
Lysholm: Lysholm Knee Scoring Scale scores; ROM: Range of motion of the affected knee joint; m: months; y: years.

Figure 5: Comparison of Lysholm scores between TK group and SB group
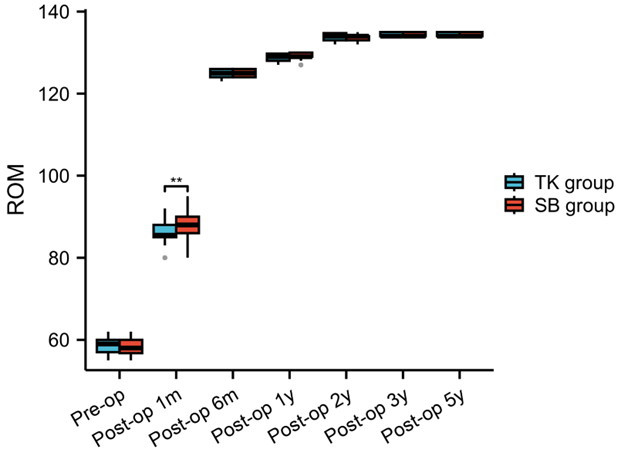
Figure 6: Comparison of the affected knee joint ROM between TK group and SB group
| TK group | SB group | t | P | Cohen d | |
| Pre-op | 5.190±0.308 | 5.177±0.328 | 0.797 | 0.428 | |
| Post-op 1m | 1.355±0.137 | 1.283±0.115 | 1.157 | 0.029 | 0.148 |
| Post-op 6m | 1.550±0.137 | 1.552±0.135 | -0.073 | 0.942 | 0.136 |
| Post-op 1y | 1.619±0.153 | 1.619±0.130 | 0.010 | 0.992 | 0.141 |
| Post-op 2y | 1.779±0.163 | 1.765±0.130 | 0.453 | 0.652 | 0.146 |
| Post-op 3y | 1.919±0.123 | 1.875±0.135 | 1.610 | 0.111 | 0.130 |
| Post-op 5y | 2.000±0.170 | 1.929±0.115 | 2.345 | 0.054 | 0.143 |
Table 4: Comparison of the measurement results by KT - 1000 in two groups (mm) TK group: Patients were treated with the joint arthroscopic tie knot technique; SB group: Patients were treated with the joint arthroscopic suture bridge technique. m: monthes; y: years.
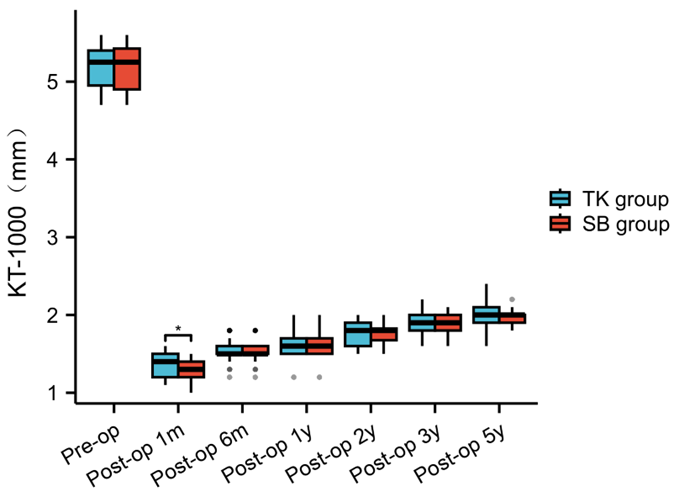
Figure 7: Comparison of the KT-1000 measurements between TK group and SB group
Biomechanical Characteristics of the Two Techniques
The treatment goals for ACL tibial insertion avulsion fractures focus on achieving anatomical realignment, ensuring strong fixation, and promoting early functional recovery. Two commonly used fixation methods—the tie-knot technique and the suture bridge technique—offer different biomechanical advantages in addressing these fractures. The tie-knot technique uses non-absorbable sutures wrapped around the fracture fragment in a bow-tie configuration to provide continuous fixation. This two-point, single-plane method depends heavily on the positioning of the two-bone tunnel exit sites within the joint, as improper placement—too far forward or backward—can cause the fragment to tilt, complicating anatomical reduction. Surgeons typically rely on clinical experience to position the tunnels correctly. While some improved approaches using three or four tunnels have shown positive results, the two-tunnel method remains preferred for its simplicity and shorter surgery time. However, the technique carries risks such as the "windshield wiper effect" and "bungee effect," which are inherent limitations. Additionally, knots tied outside the tunnel may not maintain tension long-term, leading to suture loosening. To counter this, anchors have been used for fixation with satisfactory outcomes.The suture bridge technique, inspired by rotator cuff repair, is a bridging fixation method where multiple intersecting sutures form a net-like structure to distribute uniform compressive stress, ensuring close contact between the fracture fragment and the bone bed for optimal healing. Biomechanical studies confirm its fixation strength can withstand normal ACL tension, allowing early postoperative rehabilitation. By directly implanting anchors around the bone bed, it avoids iatrogenic comminution of the fragment. Short-distance compression within the joint minimizes the "windshield wiper effect" and "bungee effect," while the mesh-like suture coverage reduces relative sliding between the fragment and bone bed, accelerating healing. In this study, the 5-year follow-up revealed a 13% reduction in tibial anterior translation (measured by KT-1000) in the suture bridge group [(2.0 ± 0.17) mm vs. (1.9 ± 0.11) mm in the tie-knot group], indicating more stable fixation. However, the technique's complex threading process initially prolonged surgical time. As surgeons gain proficiency and procedures are simplified, operative duration is expected to decrease significantly.
Comparison of Clinical Outcomes
The findings of this study demonstrate that while the suture bridge technique required longer surgical time, it offered distinct advantages in early functional recovery. 1-month post-surgery, patients in the suture bridge group showed significantly better outcomes across multiple metrics—including lower VAS scores, higher IKDC and Lysholm functional scores, improved range of motion (ROM), and more stable KT-1000 measurements—compared to the tie-knot group, highlighting the technique's effectiveness in promoting faster rehabilitation. These results align with previous work by Zj Huang et al., who observed similar functional improvements in pediatric patients with ACL tibial insertion avulsion fractures treated using high-strength suture tie-knot fixation, where normal knee flexion-extension range and significant score enhancements were achieved by six months. However, it's worth noting that by the six-month follow-up and beyond, the differences between the two techniques diminished, with no significant variations in VAS, IKDC, or Lysholm scores, ROM, or KT-1000 stability. This suggests that both methods ultimately lead to comparable and satisfactory restoration of knee function, reinforcing existing research that emphasizes the importance of anatomical reduction and secure fixation in achieving positive mid- to long-term outcomes, regardless of the specific fixation approach used.
In this study, both groups showed no instances of fever, joint infection, nerve injury, or other severe complications, with no significant difference in complication rates between them. The types and frequency of complications observed align with previous research findings. Specifically, the suture bridge group experienced one case of superficial infection and one of joint stiffness, while the tie-knot group had one case of suture reaction; all these issues resolved with conservative management. It is important to note that non-absorbable sutures in the tie-knot method can provoke suture reactions, and high-strength sutures might cut into soft tissues during rehabilitation, potentially increasing the long-term risk of anterior cruciate ligament rupture. Conversely, the suture bridge technique, involving multiple sutures, adds procedural complexity and extends surgical duration, which could elevate the chance of superficial infections. Therefore, surgeons should choose the most suitable technique based on the patient's fracture characteristics, individual needs, and their own surgical expertise.
Innovation and Limitations of the Study
This study's key innovation is directly comparing the clinical outcomes of arthroscopic tie-knot versus suture bridge techniques for ACL tibial insertion avulsion fractures, providing valuable guidance for surgical decision-making. While offering practical insights, the research has several limitations worth noting: its retrospective nature introduces potential selection bias, the modest sample size may limit statistical reliability, and the short follow-up period precludes assessment of long-term issues like joint degeneration. Additionally, the absence of biomechanical testing means we can't directly compare the fixation strength between these methods. To build on these findings, future investigations should employ larger-scale, multi-center prospective randomized controlled trials to more thoroughly evaluate the techniques' comparative effectiveness. Such studies should also include biomechanical assessments to examine fixation stability and strength, ultimately yielding more robust clinical evidence. These improvements would help surgeons make better-informed choices between these two surgical approaches.
Both the arthroscopic tie-knot technique and suture bridge technique are effective in treating ACL tibial insertion avulsion fractures, successfully restoring knee joint stability and function with minimal complications. While the tie-knot technique stands out for its simplicity and shorter surgical duration, the suture bridge technique, despite requiring more operative time, offers superior advantages in early functional rehabilitation of the knee. Clinicians should select the appropriate method based on fracture type, patient needs, and their own surgical expertise. For younger patients seeking a quick return to functional activity, the suture bridge technique is preferable, whereas the tie-knot technique may be more suitable for those prioritizing reduced operative time.
Conflicts of Interest: The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Author Contributions: Z.L.: study concept and design, literature screening, and desk review. J.G.: initial writing. D.C.: literature screening. X.Z.: data extraction. H.L.: statistical analysis. H.Y.: primary writing, revision of the manuscript, study concept and design, statistical support, and critical revision of the manuscript. All authors have made substantive contributions to this study and manuscript, and all have reviewed the final paper before its submission.
Funding: The Ningxia Natural Science Foundation (2023AAC03543), Central Government Guides Local Science and Technology Development Fund Projects(2022FRD05038).
Informed Consent Statement: All patients included in the study signed informed consent for the conduct of the study.
Institutional Review Board Statement: The study was approved by the Ethics Committee of WuHai People's Hospital (1503022015005).
Author disclosures: No generative artificial intelligence or artificial intelligence-assisted technologies were used during the writing process.
Conflicts of Interest: The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Data Availability: Summary data can be obtained from the corresponding or first author upon reasonable request
Acknowledgements:The authors have no acknowledgements
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
