
Research Article | DOI: https://doi.org/10.31579/jcitr.2018/005
*Corresponding Author: Hajira Mojdeh, Department of Radiology, Jamal mina, Kabul, Afghanistan.
Citation: Hajira Mojdeh, The developments of innovative technologies of focal radiotherapy a viable, safe, and effective option of treatment, J. Radiology and Therapeutic Interventions. Doi: 10.31579/jcitr.2018/005
Copyright: © 2018 Hajira Mojdeh. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 October 2018 | Accepted: 23 October 2018 | Published: 29 October 2018
Keywords: brain metastases; stereotactic radiosurgery; image-guided intervention; local control
Objectives: To determine if the postoperative delivery of fractionated stereotactic radiotherapy (FSRT) for resection cavity for patients with single and resectable brain metastases is safe and effective.
Methods: A prospective feasibility protocol was set up to include patients with single and resectable brain metastases who underwent surgery and had low risk profile according to RPA classification. Fractionated stereotactic radiotherapy was applied. Single dose: 3.8 Gy, total dose: 41.8 or 49.6 Gy.
Results: There was no case of break due to clinical problems. There was no case of delay of FSRT. The onset acute toxicity was observed in 40 cases (76.9%), no grade 3 and more was seen. Local recurrence free survival was 32.6 months, local control rate at 6, 12, 18 and 24 months were 85%, 77.9%, 65.9% and 65.9%. Overall local failure occurred in 34.1% of patients. Overall survival rates at 6, 12, 18 and 24 months were 90.3%, 63.9%, 47.7% and 31.6%. Median survival was 18.3 months (13.8-22.8) and overall 17.3% were living at the time of last analysis. Distant control rates at 6, 12, 18 and 24 months were 49.4%, 38.2%, 25.5% and 22.3%. Median distant recurrence free survival was 6 months (0-12.0) with overall distant failure in 77.7% of patients.
Conclusion: FSRT for surgical cavity might be one possible option in treatment of single and resectable brain metastases.
Brain metastases occur in approximately 30% of patients with metastasized cancer, greatly shortening their life expectancies as well as detrimentally effecting personal and societal quality of life [1]. Prognostic assessments using validated scoring systems can help clinicians select approaches and management strategies for brain metastases that are tailored to the individual characteristics of the patient and his or her disease. Relevant scoring systems have been developed based on recursive partitioning analysis (RPA) and graded prognostic assessments (GPA) [2].
The exact management of patients with favorable or intermediate prognoses (RPA I and II, respectively; GPA scores ≥3 and 1.5–2.5) can vary depending on the number of metastases [3]. However, whole-brain radiotherapy (WBRT) or, in the case of resectable tumors, surgery has traditionally been performed for patients with these favorable and intermediate prognoses. Level I evidence indicates that the combination of WBRT and surgery for resectable single metastases is better than surgery alone in terms of local control (LC; 46% versus 10%), but does not confer any survival benefits [4]. Because the addition of WBRT has not been observed to improve survival, physicians and patients may be hesitant to combine WBRT with surgery.
Indeed, there are some disadvantages to WBRT besides its lack survival benefit. First, WBRT has several acute side effects, including hair loss, skin irritation, nausea, vomiting, and fatigue. Second, WBRT can have a clinically and statistically significant impact on neurocognitive function, thereby reducing patients' quality of life after treatment [5,6]. Third, WBRT standard doses of 30 Gy (in 10 fractions) and 20 Gy (in 4 or 5 fractions) appear to be suboptimal for cancers that are relatively resistant to radiotherapy, such as melanoma and renal cell carcinoma [7]. Because of these disadvantages, there is a recognized need for alternative treatment strategies. At present, WBRT is vastly used in cases that have especially favorable characteristics: a single resectable cerebral lesion with a good KPS, patient age <65 years, and a controlled or potentially controllable primary tumor. It may be considered in these cases as overtreatment. A variety of alternative therapeutic options is available in these favorable clinical scenarios, including focal high-precision radiotherapy, which we decided to investigate. However, because of the experimental nature of focal high-precision radiotherapy, we decided to begin our investigation more cautiously, using fractionated stereotactic radiotherapy (FSRT), which is a somewhat less aggressive technique.
Little data are available on hypo fractionated stereotactic radiation therapy with a single daily dose >2.2 Gy up to a total dose of 40-50 Gy that is delivered to the resection cavity after removal of a single and resectable brain metastasis. We specifically designed our study to examine the feasibility and safety of image-guided FSRT, sought to determine whether FSRT was an effective option for single and resectable brain metastases. In the present study, we describe our clinical experiences focusing on issues of reproducibility, patient safety and clinical outcome.
Patient selection and study endpoints
Demographic data for all patients were obtained from a prospectively maintained database. Informed consent was obtained from all patients before treatment. The local review committee approved the protocol. We identified 61 patients who had single brain metastases (which had resulted from a variety of different cancers), all of whom underwent resection followed by FSRT between January 2010 and December 2012. Of the 61 identified cases, 52 met our protocol's inclusion criteria: a single resectable cerebral lesion with KPS >60 and a controlled or potentially controllable primary tumor. We did not exclude patients older than 65 years, so long as they were physically fit, active, younger than 75 years, but explicitly wished to receive FSRT.
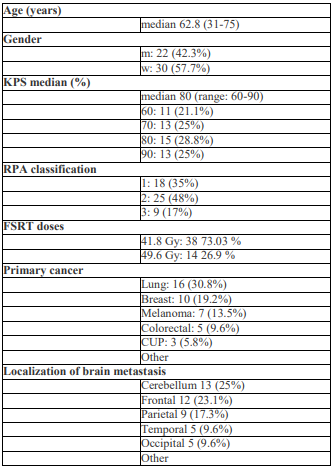
The median age of included patients was 62.8 years (31–74 years). The study cohort comprised 30 female and 22 male patients. One experienced team performed the surgical procedures, and a second experienced team performed the radio therapeutic procedures. A multidisciplinary team made clinical decisions. The primary endpoints of the study were technical and medical feasibility, including workflows and FSRT-related toxicity greater than grade 2, according to the Common Terminology Criteria for Adverse Events (CTC AE, version 4.0). The secondary endpoint was local tumor control within the irradiated region.
Treatment
All patients were treated with image-guided frameless (linac)-based FSRT. The majority of patients (n=38, 73%) received 41.8 Gy at 11 fractions of 3.8 Gy. The remaining patients (n=14, 26.9%) received two additional fractions, increasing the total to 49.4 Gy (13 fractions of 3.8 Gy).
Patient immobilization was achieved using a commercially available head mask fixation system (Brainlab AG, Feldkirchen, Germany). The specific characteristics of the system and principles of the technique have been described previously [8]. The clinical target volume (CTV) was identified on the basis of 1 mm gadolinium-enhanced axial MRI (Siemens Medical Systems, Erlangen, Germany) images fused with computed tomography (Siemens Medical Systems, Erlangen, Germany) image data sets. Scanning was conducted in the spiral mode using a pitch of 0.75, and slices of 1.2 mm thickness and spacing were acquired for the entire cranium. Surrounding edema or the operative corridor was not included. The dose prescription was made to the planning target volume (PTV), which consisted of the CTV with an added 2 mm margin around it as the planning target volume (PTV). To ensure that at least 95% of the PTV received the prescribed dose, doses were prescribed constantly to the 80% isodose line, as normalized to the maximum dose. Treatment volumes were achieved with 3–5 dynamic arcs using a dedicated Novalis accelerator (Brainlab AG, Feldkirchen, Germany). Dexamethasone therapy was started by the first day of treatment, orally administered at doses of 4–6 mg per day, and maintained for 10 days following the end of treatment.
Follow-up
Patients were clinically observed before and during FSRT. The first follow-up appointment was scheduled three months later, with additional appointments occurring at least once every six months. We planned to document treatment-related toxicity in first three months following FSRT. Local progression was defined as new contrast enhancement in the PTV. Distant intracranial progression was defined by the presence of new brain metastases or leptomeningeal enhancement outside the PTV. For each patient who died, we attempted to determine the cause of death.
Statistics
LC, distant control (DC), and OS were defined as beginning at the time of FSRT and were estimated using the Kaplan-Meier method. In univariate analyses, we used the log-rank test to assess survival differences for categorical variables and the Cox proportional hazards model to assess survival differences for continuous variables. Significant prognostic factors (p<0.05) were included in a multivariate analysis, using a Cox proportional hazards regression model. Statistical evaluations were performed using a commercial statistical software package (SPSS version 20.0, IBM Germany GmBH).
Patient and tumor characteristics are summarized in Table 1. The most common primary tumors were non-small cell lung cancer (16/52, 30.8%), breast cancer (10/52, 21.1%), melanoma (7/52, 9.2%), and colorectal cancer (5/52, 6.6%). Median follow-up time with imaging was 9.6 months (1–45 months).
The median interval between surgery and FSRT was 1.9 months (0.53–4.01 months). Median KPS at the time of FSRT was 80 (60–90). Ten patients were excluded from the analyses of LC, DC, and salvage therapy because sufficient imaging data were unavailable.
Primary endpoints: feasibility, acute toxicity
With respect to feasibility, we observed that all patients completed FSRT. No cases involved breaks or pauses in FSRT because of adverse responses. In three cases, there was a short break (1–2 days) because of technical problems with the machines. All delays in the time of FSRT were scheduled in advance; there were no unscheduled delays.
With respect to FSRT-related toxicity, new-onset acute toxicity was observed in 40 cases (76.9%). However, none of these cases involved acute toxicity of grade 3 or higher. Patients reported manageable fatigue (grade 2, n=32, 61.5%), lethargy (grade 2, n=32, 61.5%), headache (grade 2, n=18, 34.6%), dizziness, (grade 2, n=12, 23%), and ataxia (grade 2, n=6, 11.5%).
Secondary endpoint: local control
In 10 cases a recurrence occurred. Median local recurrence-free survival was 32.6 months. LC rates at 6, 12, 18, and 24 months were 85%, 77.9%, 65.9%, and 65.9%, respectively (Figure 1). Overall, local failure occurred in 34.1% of patients. Univariate analysis identified residual tumor mass after resection as a highly significant factor associated with local failure (p<0.001).
Tertiary endpoint: overall survival and distant control
Median survival was 18.3 months (range: 13.8–22.8 months), with 17.3% of patients alive at the time of last follow-up. OS rates at 6, 12, 18, and 24 months were 90.3%, 63.9%, 47.7%, and 31.6% (Figure 2). RPA and KPS were identified prognostic factors for OS. Univariate analysis also indicated that RPA class 2 was predictive of OS (p<0.02), and that RPA class 1 was associated with better survival than RPA class 3 (p<0.061). An analysis of patients stratified according to KPS (Group 1 KPS: 80–90, Group 2 KPS: 60–70) confirmed KPS of Group 1 was predictive of better survival (p<0.048).
DC rates at 6, 12, 18, and 24 months were 49.4%, 38.2%, 25.5%, and 22.3%, respectively. Median distant recurrence-free survival was 6 months (range: 0–12.0 months) with distant failure ultimately occurring in 77.7% of patients.
Salvage therapy
Twenty-six of 42 patients (61.9%) received salvage therapy: 42.3% received WBRT (n=11), 42.3% received FSRT (n=11), and 9.5% underwent resection (n=4). Among the 26 patients, the median time to salvage therapy was 5.3 months (range: 1.87–19.91 months). The median subsequent survival time was 8.4 months (range: 5.2–11.6 months). In 69.23% of cases (18/26), the patient received initial salvage therapy because of distant failure alone.
Our results demonstrate the technical and medical feasibility of focal high-precision radiotherapy (FSRT) of the resection cavity after removal of single brain metastases. Our decision to defer investigation of whole-brain radiotherapy was motivated by the only prior study that provided level 1 evidence [4] and the few other relevant studies that provided lower-level evidence and were available when we planned our study [9-12]. We were additionally motivated by outcome data showing that, for a variety of cancers, improvements in systemic therapy lead to longer survival times.
Currently, the delayed effects of WBRT are becoming a more serious issue. During study planning, we generated a specific hypothesis for investigation: WBRT is deferrable, and it is better to postpone WBRT for patients who have resectable single brain metastases and favorable risk profiles, and therefore longer life expectancies. However, WBRT undoubtedly reduces local and regional recurrence when assessed in a prospective setting [4,13]. For patients with multiple, unresectable or medium–high risk brain metastases, WBRT should remain the standard treatment.
Technical and medical feasibility
our preliminary results indicate that FSRT is feasible from a technical perspective, at least for departments that have sufficient technical infrastructure and experienced teams. FSRT is also safe, causing no severe side effects. However, the duration of FSRT may be a critical limitation; FSRT is delivered over the course of two weeks. To date, few studies have considered hypo fractionation. To our knowledge, this study's dose regimen (a single dose of 3.8 Gy delivered in 11–13 fractions) is the only regimen of this type.
Few previous studies of FSRT have reported toxicity. In a recent study of 33 cases, Steinmann et al., reported no toxicities of grade 2 or higher [14]. Their study examined a dose prescription that nominally differed from our own, but was actually similar in terms of biologic equivalence. The authors reported side effects including mild alopecia, dermatitis, and fatigue. Only eight patients received corticosteroids at the end of radiotherapy. In an excellent study of 33 patients with solitary brain metastases, Connolly et al., reported side effects experienced during and after a hypo fractionated radiotherapy regimen (2.67 Gy, 15 times) that was similar to our own. It was observed that none of the patients experienced additional neurological symptoms related to the therapy [15].
Local control
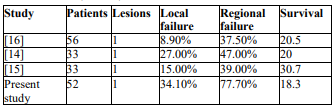
A 65.9% LC rate was observed in the present study. This is the lowest LC rate of among the studies compared, possibly because 9.5% of patients included in the estimation of intracranial control had residual tumor mass, which was strongly associated with local failure. We observed no significant difference in LC rates between the two dose regimens. The median prescription dose of 41.8 Gy was comparable to studies with a wide range of LC rates. For example, in a study with a prescription dose of 40 Gy, Steinmann et al., observed a 73% LC rate [14], while in a study with a prescription dose of 40.5 Gy, Connolly et al., observed an 85% LC rate [15]. Considering the small sizes of study cohorts, the LC rate that was observed in the present study may be not be unusual at all (Table 2).
Overall survival
Median OS times have ranged from 18.3 to 30.7 months in studies of patients with single brain metastasis who received focal radiotherapy after resection [14-16], including the OS in the present study. In comparison, median OS times have ranged from 11 to 17 months for cohorts that include multiple brain metastases [10-12,17-22].
Among patients with brain metastases, single brain metastasis is predictive of longer survival [11]. Accordingly, the present study's median survival time of 18.3 months reasonably consistent with previous reports, particularly in comparison to the approximately 20 month median OS that was observed in a prior study of a similar number of patients [16]. Three retrospective studies of single brain metastases that incorporated the present study's treatment mode reported a median survival time of 20–30.7 months [14-16], whereas studies with initial postoperative WBRT reported median survival times of 10.7–12 months [4,13]. Therefore, research on the difference in survival times for patients with single brain metastasis could provide a major argument for proper treatment.
Our analysis of RPA indicated that classes 1 and 2 were associated with better OS than class 3. However, we did not observe any significant difference in OS between RPA classes 1 and 2, perhaps because the factors contributing to RPA classification (age, extra-cranial metastases) were not significantly associated with OS in our univariate analyses. Therefore, KPS could be the major factor that contributes to the survival differences that were observed. Additionally, the number of patients and the case censoring varied across RPA classes.
Distant intracranial control
The 6-month median DC time fell short of the18.3-month median OS time. The rather low 22.3% DC rate suggests the underlying reason for the majority of first salvage interventions (69.2% of salvage therapies followed loss of DC). Therefore, patients were burdened by complications of distant metastases and the associated therapeutic aftermath. Higher DC rates have previously been reported for WBRT as standard treatment after surgery (range: 76–86%) [4,13].
These findings lead us to question the value of enhanced DC conferred by WBRT, drawing attention to the specifics of the application of WBRT in the present study. First, STs of the relevant cases were conducted after a median of 5.37 months. In the present study, 26.19% of first salvage therapies after recurrence were WBRT. Compared with traditional upfront WBRT, use of WBRT as salvage therapy delays possible side effects. Second, 16.7% (7/42) of people in the present study lived longer than 18 months without recurrence, and 11.9% (5/42) lived longer than two years without recurrence. These patients are proof that WBRT is not necessary for long-term survival. Indeed, these patients entirely avoided the risks of upfront WBRT. Apart from these two arguments in favor of image-guided stereotactic radiotherapy, there is little evidence concerning the balance of benefits and harms of upfront WBRT and WBRT as a salvage therapy after DF.
However, despite the side effects of WBRT [5,23], which include loss of health-related quality of life [24], there is some contradictory evidence concerning its effects. Indeed, overall neurocognitive benefit has been claimed [25], as well as the possibility of reducing harm by sparing portions of the brain [26,27].
In the last decade, the developments of innovative technologies have made focal radiotherapy a viable, safe, and effective option of treatment. Accordingly, the predominance of WBRT treatment strategies should be critically revised. The use of WBRT as a one-size-fits-all treatment should be reconsidered. In the present study, we examined FSRT of the surgical cavity and demonstrated that it could be a treatment option for single and resectable brain metastases.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
