
Case Series | DOI: https://doi.org/10.31579/2692-9422/010
1 Physiotherapy studio of Villanuova sul Clisi, Brescia, Italy.
2 Multidisciplinary Medical Center, Brescia, Italy.
3 Physiotherapy studio Fisiotek Castiglione delle Stiviere.
4 Center for Genetic Engineering and Biotechnology, Havana, Cuba.
5 Latin American School of Medicine, Havana, Cuba.
*Corresponding Author: Giselle Pentón-Rol, Avenida 31 No.15802 e/ 158 y 190, Reparto Cubanacan, Havana, Cuba.
Citation: Matteo Bonori, Giovanni Galli, MD, Nicola Gennari, Sara Sudati, Giselle Pentón-Rol, MD, PhD, (2025), The Bonori Method: Whole-Body Shock Wave Stimulation of the Myofascial System and Traditional Chinese Medicine Meridians in Neurodegenerative Diseases – A Case Series, J Neurodegeneration and Neurorehabilitation, 4(1); DOI:10.31579/2692-9422/010
Copyright: © 2025, Giselle Pentón-Rol. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 August 2025 | Accepted: 21 August 2025 | Published: 02 September 2025
Keywords: Bonori method; neurodegenerative diseases; multiple sclerosis; Parkinson's disease
Neurodegenerative diseases such as multiple sclerosis (MS) and Parkinson’s disease (PD) have limited pharmacological treatment options, highlighting the need for novel rehabilitative strategies. The Bonori Method is an innovative physiotherapeutic intervention that combines radial extracorporeal shock wave therapy with stimulation of the myofascial system and acupuncture meridians based on Traditional Chinese Medicine (TCM). In this observational study, four patients with MS and six with PD received weekly 40-minute sessions of the Bonori Method over one year (MS) or six months (PD). Clinical evaluations conducted before and after the intervention revealed significant improvements in physical and emotional parameters. These included the SF-36 quality of life questionnaire, Tinetti balance and gait scale, Beck Depression Inventory-II, and visual analogue pain scale in MS patients, and the Unified Parkinson’s Disease Rating Scale (UPDRS)and Hoehn and Yahr staging in PD patients. These findings suggest that the Bonori Method may enhance quality of life in individuals with neurodegenerative conditions.
Neurodegenerative diseases such as Multiple Sclerosis (MS) and Parkinson’s disease (PD) are progressive and disabling conditions for which few pharmacological treatments can significantly alter disease progression or improve long-term quality of life [1,2]. As a result, there is growing interest in physiotherapeutic and integrative approaches that may support physical function and neurological stability in these patients.
Extracorporeal shock wave therapy (ESWT) has demonstrated potential in reducing spasticity and improving motor function in patients with neurological disorders [3]. In MS, ESWT combined with botulinum toxin A reduced muscle spasticity and improved mobility [4]. In PD, focused ESWT applied to cortical and subcortical regions reduced motor symptoms, as reflected by UPDRS scores [5].
In parallel, Traditional Chinese Medicine (TCM) therapies, including acupuncture and meridian stimulation, have shown potential neuromodulatory effects in MS [6] and PD [7]. These approaches aim to regulate neurovascular, neurolymphatic, and muscular systems through activation of specific anatomical points.
Building on these therapeutic foundations, the Bonori Method (BM) was developed in 2017 by physiotherapist Matteo Bonori. BM integrates radial ESWT with systematic stimulation of myofascial structures and TCM meridians throughout the body. Although the method has been applied in athletic and clinical practice, no peer-reviewed studies have been published to date. The present case series therefore represents the first formal scientific report evaluating BM in neurodegenerative conditions.
This study presents a case series describing the clinical outcomes of ten patients (four with MS and six with PD) treated with the BM. We evaluated changes in motor, emotional, and quality-of-life parameters using validated clinical scales, with the aim of exploring the potential utility of this integrative approach in neurorehabilitation.
Study Design and Ethics
This prospective case series was conducted in a real-world clinical setting to evaluate the effects of the Bonori Method in patients with neurodegenerative diseases. The study included ten patients, which falls within the accepted range of case series design in clinical research, typically involving between two and ten participants. The study was carried out with clearly defined inclusion and exclusion criteria, standardized intervention procedures, validated clinical scales, and ethical oversight. All procedures complied with the institutional and national research committee standards and with the 1964 Declaration of Helsinki and its later amendments [8]. Written informed consent was obtained from all participants prior to inclusion. As the intervention was non-pharmacological and exploratory in nature, and no control group was included, trial registration was not required.
Patient Selection and Characteristics
Inclusion Criteria
For patients with multiple sclerosis:
• Diagnosis of MS according to the 2017 McDonald Criteria [9]
• Age between 18 and 80 years [10]
• Expanded Disability Status Scale (EDSS) score between 1.5 and 4.5 [11]
• Relapsing-remitting MS (RR-MS) subtype [12]
For patients with Parkinson’s disease:
• Diagnosis based on the Movement Disorder Society Clinical Diagnostic Criteria for PD [13]
• Age between 18 and 80 years [14]
Exclusion Criteria (MS [15] and PD [16]):
• Clinically active disease
• Pregnancy
A total of 10 patients were included in the study:
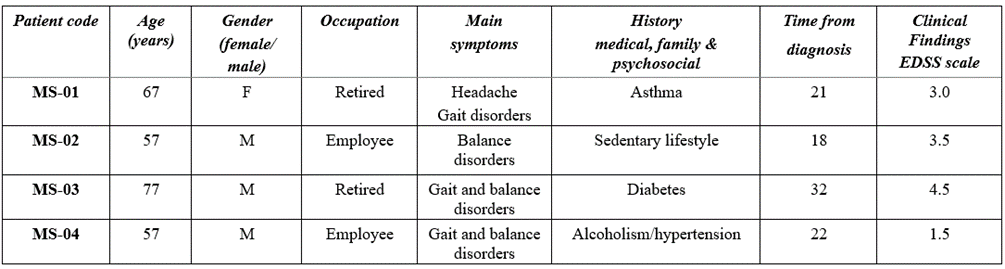
• MS group: 4 patients (3 males, 1 female), aged 57–67, EDSS 1.5–4.5
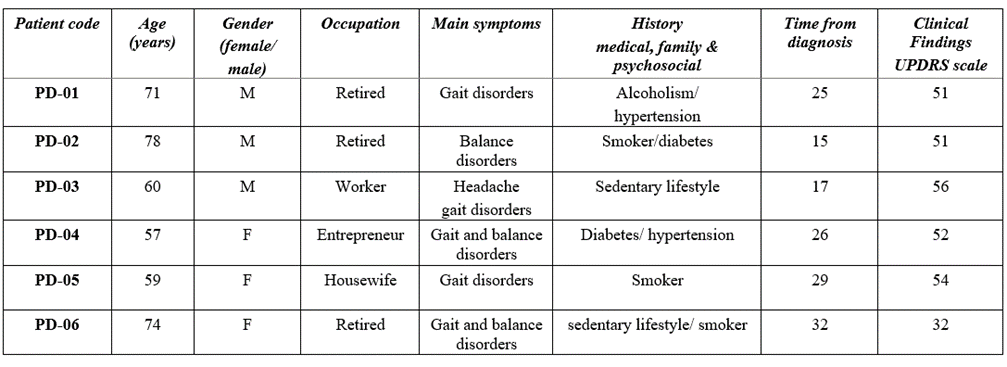
• PD group: 6 patients (3 males, 3 females), aged 57–78, UPDRS scores 32–56
Detailed patient characteristics are presented in Table 1.
Table 1: Patient information. Description of patient information. Demographic characteristics, main symptoms, medical-family and psychosocial history, time from diagnosis, clinical forms and clinical findings.
Intervention: The Bonori Method
Treatment Protocol
The intervention involved whole-body treatment using rESWT therapy with the EMS device. Each session delivered approximately 25,000 shock wave pulses at 10–12 Hz and ~2.2 bar pressure.Treatment targeted areas of increased myofascial tension, with a focus on muscle chains and meridians fromTCM. Specific acupuncture points—such as ST36 (Zusanli), LI4 (Hegu), and KI1 (Yongquan)—were stimulated, along with neurolymphatic and neurovascular zones.
Treatment Duration
• MS patients: 48 weekly sessions over one year (40 minutes each)
• PD patients: 24 weekly sessions over six months (40 minutes each)
Each session followed a fixed anatomical sequence, progressing from the anterior abdominal region to limbs and posterior chain, including the diaphragm, paravertebral regions, neck, and extremities.
Evaluation and Outcome Measures
Assessment Tools
For MS patients:
1. Short Form-36 Health Survey (SF-36) – Italian version 1.6 (IQOLA translation) [17].
2. Tinetti Performance-Oriented Mobility Assessment [18] – balance and gait subscales (max 28 points)
3. Beck Depression Inventory-II (BDI-II) [19].
4. Visual Analogue Scale (VAS) [20] for subjective pain intensity
For PD patients:
1. Unified Parkinson’s Disease Rating Scale (UPDRS) [21] – total and subscale scores.
Data Analysis
Given the exploratory nature of this case series and the small sample size, data analysis was primarily descriptive. Quantitative variables were summarized using means, standard deviations, and ranges. Within-patient comparisons (pre- vs. post-treatment) were assessed using paired non-parametric tests (Wilcoxon signed-rank test) for ordinal or non-normally distributed variables.
Graphical representations were created using GraphPad Prism 10.0 (GraphPad Software, San Diego, CA). A p-value of less than 0.05 was considered statistically significant. No adjustments for multiple comparisons were applied due to the observational design and hypothesis-generating purpose of the study.
Effects of the Bonori Method in Patients with Multiple Sclerosis
Figure 1 illustrates the evolution of the eight health domains of the SF-36 scale in the four RR-MS patients treated with the BM over one year. Patients 1, 2, and 3 showed significant improvements between baseline and final assessments (p less than 0.05 for patients 1 and 2; p less than 0.05 for patients 1 and 2; p < 0>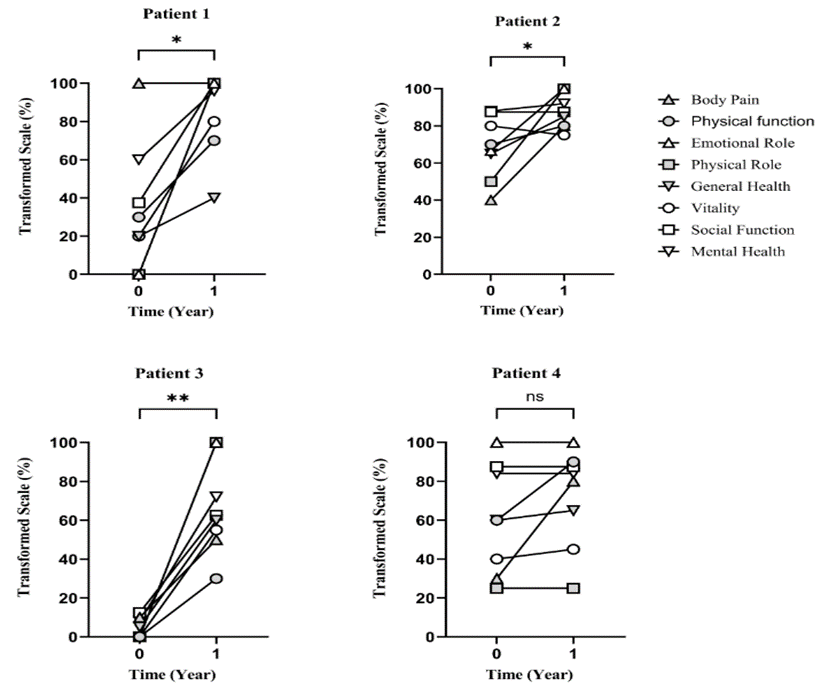
Figure 1: Effect of the application of the Bonori method in Multiple Sclerosis. RR-MS patients were treated with the Bonori method, once a week for 1 year. The graphs show the value in % of the Transformed Scale (TS) according to the equation described in the text; on the score of the eight multi-item scales (Physical Function, Physical Role, Body Pain, General Health, Vitality, Social Function, Emotional Role and Mental Health) of the SF-36 Health Questionnaire; at the beginning (baseline) and one year after the Bonori method. Wilcoxon matched-pairs signed rank test, p less than 0.05 (*), p<0>
Table 2 (column A) presents the Tinetti Balance and Gait Scale scores. Improvements were evident in all patients: Patients 1 and 4 improved by 13 points, Patient 3 by 7 points, and Patient 2 by 2 points. Notably, Patient 2 had an initially high baseline score (25/28), suggesting a ceiling effect that limited further gains.
Table 2 (column B) shows the results of theBDI-II. All four patients exhibited reduced depression scores post-treatment. Patient 3, who initially presented moderate depression (23 points), improved to a score of 5, indicating a marked emotional recovery. The other patients started within the "minimal depression" range and also showed reductions in their scores.
Pain intensity, measured using the VAS (Table 2, column C), decreased in all four patients following treatment. Patient 4, who initially reported the highest pain level (7 points), experienced a marked reduction to 2.5 points. Patients 1 and 2, who started with mild pain (2 points), reported either complete resolution or minimal residual pain after treatment. Patient 3 also showed substantial improvement, with pain decreasing from 5 to 0.5 points.
Table 2. Physical, emotional and pain scales in the 4 Multiple Sclerosis patients, at baseline and after 1 year of treatment with the Bonori method. The table shows the evaluations of the different scales: A) Tinetti: Measures balance (on a scale of 16) and gait (on a scale of 12); for a total of 28. B) BDI-II Measures the emotional degree; from 0-13- normal, from 14 -19- mild depression, from 20-28- moderate depression, from 29-63- severe depression. C) VAS- Measures the intensity of pain on a scale of 0 to 10.
Patient code | Times | SCALES | |||
| A | B | C | |||
| Tinetti evaluation | Beck's Depression Inventory (BDI-II) (From 0 to 63) | Visual analogue pain (VAS) (From 0 to 10) | |||
| Balance | Walk | ||||
| MS-01 | Time 0 (baseline) | 9/16 | 2/12 | 13 | 2 |
| 11/28 | |||||
| Time 1 (after 1 year of Bonori method) | 14/ 16 | 10/12 | 0 | 0 | |
| 24/28 | |||||
| MS-02 | Time 0 (baseline) | 16/16 | 9/12 | 2 | 2 |
| 25/28 | |||||
| Time 1 (after 1 year of Bonori method) | 16/16 | 11/12 | 0 | 0.5 | |
| 27/28 | |||||
MS-03
| Time 0 (baseline) | 4/16 | 2/12 | 23 | 5 |
| 6/28 | |||||
| Time 1 (after 1 year of Bonori method) | 8/16 | 5/12 | 5 | 0.5 | |
| 13/28 | |||||
MS-04
| Time 0 (baseline) | 6/16 | 2/12 | 13 | 7 |
| 8/28 | |||||
| Time 1 (after 1 year of Bonori method) | 12/16 | 9/12 | 11 | 2.5 | |
| 21/28 | |||||
Effects of the Bonori Method in Patients with Parkinson’s disease
Figure 2 shows the UPDRS and Hoehn and Yahr scores for the six PD patients before and after six months of BM treatment. The UPDRS total scores showed a statistically significant reduction (p less than 0.05), while changes in the Hoehn and Yahr stage were less consistent.
Patients 1 and 6 demonstrated moderate UPDRS improvements (4–5 points) without change in Hoehn and Yahr scores. The remaining patients exhibited more pronounced improvements (8–12 points in UPDRS), often associated with a one-stage reduction in the Hoehn and Yahr scale (Table 3).
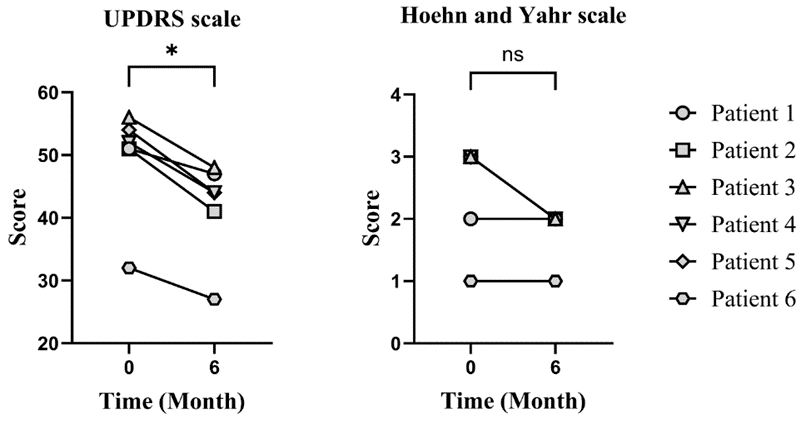
Figure 2: Effect of the Bonori method on the UPDRS and Hoehn and Yahr neurological scales in patients with Parkinson's disease. The graphs show the values of both scales at the beginning and after 6 months of treatment with the Bonori method in the 6 patients with Parkinson's disease. Wilcoxon matched-pairs signed rank test, p less than 0.05 (*), non-significant (ns) using GraphPad Prism Software.
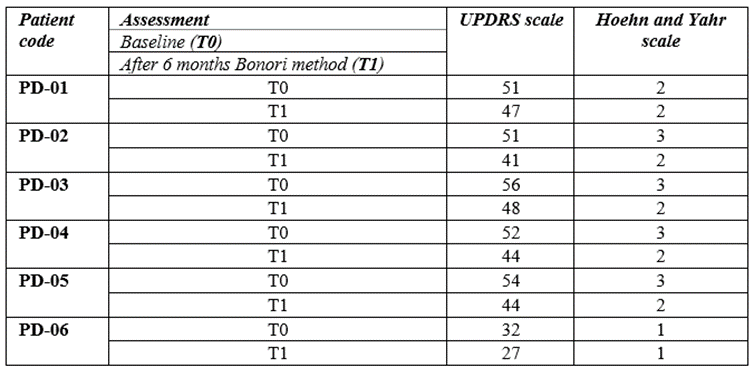
Table 3: Individual variation of the UPDRS and Hoehn and Yahr scales in patients with Parkinson's disease. The table shows the scores on both scales in the 6 patients with Parkinson's disease, at the beginning and after 6 months of treatment with the Bonori method.
Neurodegenerative diseases often cause disabling motor symptoms such as spasticity and balance disorders, which are frequently accompanied by emotional disturbances like depression and anxiety. These factors can significantly impair quality of life [22]. In this context, the BM offers an integrative approach aimed at improving both physical and emotional health through ESWT therapy aligned with TCM meridians.
To our knowledge, no other clinical studies have reported the use of ESWT applied systematically to the whole body based on TCM meridians in patients with MS or PD. One previous study applied shock waves to selected acupuncture points in low back pain [23], but the BM protocol is broader and more structured, incorporating both somatic and emotional dimensions.
Among MS patients, patient 3 showed the most significant overall improvement across SF-36 domains, starting from the lowest baseline scores. This highlights the potential of BM to benefit patients with more severe baseline impairments. Improvement in balance, assessed by the Tinetti scale, supports the role of BM in enhancing postural control, a critical issue in MS [24]. The significant reduction in depressive symptoms observed in patient 3, as evidenced by the BDI-II, may be linked to the improvements in physical functioning, suggesting a mind–body synergy.
Pain perception, evaluated via both VAS and the SF-36 pain domain, also improved in a correlated manner, particularly in patients 3 and 4. This aligns with literature suggesting that subjective pain intensity is strongly influenced by emotional and functional status [25].
In PD patients, the UPDRS scale reflected consistent clinical improvement after 6 months of BM. Although the Hoehn and Yahr stage did not always change, patients with UPDRS improvements greater than 8 points also showed one-stage reductions in Hoehn and Yahr, suggesting that functional recovery may precede detectable staging improvements [26].
These results are consistent with prior evidence supporting the benefits of physiotherapy in the early stages of PD [27]. However, the BM differs by incorporating shock wave stimulation across muscle chains and acupoints, which may explain the broad range of clinical effects.
This study provides the first clinical evidence on the potential of the BM, which uniquely integrates whole-body ESWT with TCM meridian stimulation. The findings suggest synergistic benefits on physical and emotional domains in ND patients. The duration of the intervention—one year for MS and six months for PD—allowed for the assessment of long-term effects, in contrast to many physiotherapeutic studies of shorter duration. The main limitations of this study are the small sample size and the absence of a control group, which restrict generalizability. Additionally, as this is an exploratory case series, molecular and physiological biomarkers (such as Sirtuin 1) were not measured. Future controlled clinical trials will incorporate biomarker assessments, including Sirtuin 1, to better understand the physiological mechanisms involved.
The BM may offer a novel, non-invasive therapeutic strategy for managing symptoms in patients with MS and PD. Its application could be extended to athletes and individuals at risk of chronic degenerative conditions. Wider dissemination across Italy and internationally would benefit from formal practitioner training programs.
Future research should investigate the molecular and physiological mechanisms underpinning the BM effects, including studies involving neuroimaging, biomarkers, and mechanistic models of neuroplasticity.
To our knowledge, this is the first peer-reviewed clinical report describing the Bonori Method (BM) applied to neurodegenerative diseases. Although BM has been used in athletic and clinical practice since its development in 2017, no formal scientific publications have been available until now. This novelty represents both strength and a limitation: on one hand, it highlights the originality of the approach; on the other, it restricts the possibility of direct comparison with previous studies. The present case series therefore provides an essential foundation for future controlled trials and mechanistic investigations that may validate and expand upon these preliminary findings. Importantly, our observations offer the first clinical data supporting BM as a promising physiotherapeutic intervention for multiple sclerosis and Parkinson’s disease. The improvements observed in mobility, mood, and pain suggest its potential to enhance quality of life in patients with neurodegenerative conditions. These results warrant further investigation in larger, controlled studies and support the mission of the Bonori Physiotherapy Network to advance innovative and holistic treatment approaches for neurological disorders.
The authors declare no conflict of interest.
The authors of this manuscript would like to thank the staff, especially the physiotherapists, who are applying the Bonori method in their studios, academies and hospitals.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
