AUCTORES
Globalize your Research

Case Report | DOI: https://doi.org/10.31579/2768-2757/165
Neurosurgical department, Medical and pharmaceutical school, laboratory of neurological, neurosensorial disease and disability, Hassan II university, Ibn Rushd Hospital, Casablanca, Morocco.
*Corresponding Author: Said Hilmani MD, PhD, Neurosurgical department, Medical and pharmaceutical school, Hassan II university, Ibn Rushd Hospital, Casablanca, Morocco.
Citation: Said Hilmani, Khadija Idahoan, Abdehakim Lakhdar, (2025), Successful Clipping of a Newborn Ruptured Geant Middle Cerebral Artery Aneurysm, Journal of Clinical Surgery and Research, 6(3); DOI:10.31579/2768-2757/165
Copyright: © 2025, Said Hilmani. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 March 2025 | Accepted: 20 March 2025 | Published: 18 March 2025
Keywords: anatomy; ankle; minimally surgery; surgical options
Objective: Ruptured Neonatal intracranial aneurysms are exceptional. Their etiology is not clear and are traditionally managed by endovascular embolization. We report a successful surgical clipping of neonatal geant aneurysm to encourage surgical treatment of this disease.
Case report: We describe the case of a 23-day-old girl with a ruptured geant intracranial aneurysm. She presented with seizure without fever or neurological deficit. CT-scan showed a large hematoma in the left frontotemporal region without hydrocephalus or ischemia. Cerebral angioscan demonstrated a large and partially thrombosed aneurysm arising from parietat branche of middle cerebral artery. She underwent successful surgical clipping with a good recovery without sequella under anticonvulsivant therapy.
Conclusion
Neonatal intracranial aneurysms are uncommon and can be treated safely by surgical clipping. Endovascular treatment is a good option in dificult cases despite the risque of radiation at this age.
Cerebral aneurysms are rare in infants representing less than 4% (3) and exceptional in neonatal period [11]. But the developement and increasing use of cerebral angiographical explorations, intracranial aneurysms are being reportered more often. Management of ruptured intracranial aneurysm is classically treated by embolisation. Few cases are opereted with succssus. We report the first case of succssful clipped neonatal aneurysm.
The patient was a 23-day-old girl born by normal vaginal delivery after an uncomplicated pregnancy. Her birth weight was 2900 gm. There was no history of infectious disease or head injury. she was admitted to pediatric department for apyretic seizure. The girl's general and neurological examination was normal with no fever. Her head circumference was normal. The blood account and chemistries were normal as hemostasis tests. Cerebral CT -scan showed a large hematoma with perifocal edema in the left frontotemporal region asssociated to suspected middle cerebral artery aneurysm without hydrocephalus or ischemia (Figure. 1),
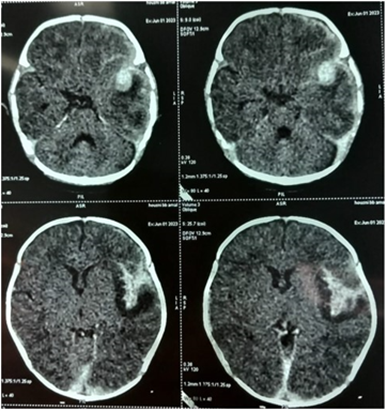
Figure 1: CT-scan shows large subcortical hemorrhage in the left cerebral hemisphere, associated to a round enhancing lesion suspected of the cerebral aneurysm.
Cerebral angio-MRI and angioscan demonstrated a large and partially thrombosed aneurysm (11 x 11 x 9 mm) arising from M2 of the left middle cerebral artery with a large neck (Figure. 2),
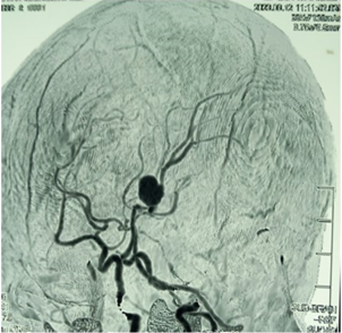
Figure 2: CT angiograms: saccular aneurysm with 11 x 11 x 9 mm size, arising from M2 of the left middle cerebral artery with a large neck.
Because of young age, endovascular treatment was not possible in our condition. After sylvian fisure discection and hematoma evacuation a large aneurysm sac was discovered originating 2 cm after middle cerebral artery bifurcation. We successfully clipped a ruptured aneurysm after temporary clip on upstream of aneurysm (Figure. 3),
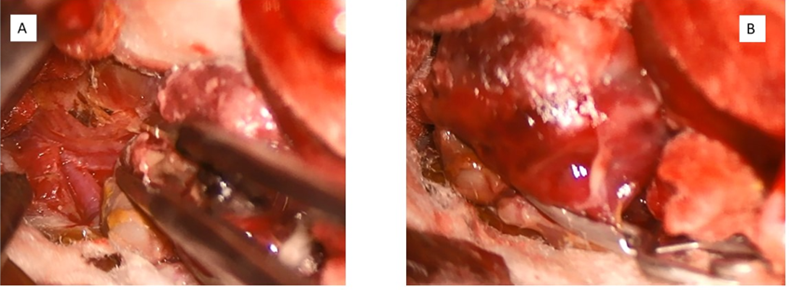
Figure 3: Intraoperative photograph shows (A) the large saccular aneurysm arising from M 2 and (B) neck clipping.
The dome was resected and histological examination showed an organized thrombus in the anevrysmal wall. Patient had episodic seizue in the postoperative course well controled by anticonvulsant therapy. She was discharged without neurological deficits 10 day later.
Intracranial aneurysms are uncommon in young children and exceptional in newborns [11] and their rupture represents 10-23% mortality [3]. The more frequente vascular malformations in this age are Galen vein aneurysms [7]. The youngest patient reported had 3-day-old [6]. Our patient had 23 days and representing the youngest reported case in Morocco. They have some characteristics, sixty seven percent of the aneurysms arose from the anterior circulation and 42% arose from the middle cerebral artery and its branches [12], followed by anterior communicating artery and they tend to be large as reported in our patient [1, 5, 8]. Vasospasm is more tolerated than in adult [3,13]. and the etiology is not clear. They can be related to brain injury and infection [10], but it is thought that at this age, a congenital anomaly of the vascular system during fetal development is the strongest cause. Seizures are the most common initial signs of anevrysmal rupture reported in literature, followed by Loss of consciousness [1,11]. Mortality rate after ruptur is about 50% [2]. They have been associated to other diseases and congenital anomalies included obstructive hydrocephalus caused by stenosis of the sylvian aqueduct hydromyelia of the spinal cord, a malformed fourth ventricle, hypoplasia of the cerebellum, and agenesis of the corpus callosum [3,12]. To our knowledge, there is no recommendation on managment as on the timing of surgery in this age as clearly established in adults. Surgical treatment with clipping of the aneurysm is the save and optimal treatment as reported by many authors [4,13], with a relative easy vascular dissection and a good tolerance of the surgical procedure. Clipping is recommended, allowing drainage of intraparenchymal hematoma, excluding the aneurysm better than embolisation and removing the mass [8, 9]. Advances in techniques mean that endovascular intervention is possible in newborn patients and can an alternative treatment in dificult or non surgical cases. It is the first-line treatment choosed by other teams producing less bleeding than clipping [8, 11]. But the decrease in the use of radiation in endovascular procedures is an advantage for clipping. Clipping and neurological endovascular therapy have shown similar results [3]. The prognosis is better attributed to the for mation of intracerebral hematomas at peripheral sites, the rarity of vasospasm, and the good functional compensation of the young brain.
Aneurysms in infancy are very rare and differ from adult in frequence, etiology, management and evolution. Clipping is a safe and effective treatment, but embolisation represents an alternative treatment in selective cases. The prognosis appears to be much more favorable. A good prognosis also depends on a prompt diagnosis.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.



























































