
Research Article | DOI: https://doi.org/10.31579/2643-1912/004
1 Deportment of Medicinal chemistry, Unity college of Pharmacy, Bongiri, India
2 Deportment of Pharmacology, Unity college of Pharmacy, Bongiri, India
3 Deportment of Pharmaceutics, Unity college of Pharmacy, Bongiri, India
*Corresponding Author: Ampati Srinivas, Deportment of Medicinal chemistry, Unity college of Pharmacy, Bongir, India.
Citation: Ampati Srinivas Kokkula pavan Kumar and Prasad Garrepally, Subcutaneous DL Technique Has Proven To Be an Adequate Host for Human Embryonic Stem Cells, DOI: 10.31579/2643-1912/004
Copyright: © 2019 Ampati Srinivas, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 March 2019 | Accepted: 09 April 2019 | Published: 12 April 2019
Keywords: islet Transplantation; embryonic stem cells; cell engraftment; cell maturation
Islet transplantation has become an important treatment modality for Type 1 Diabetes Mellitus (T1DM); nonetheless, the procedure may be limited by donor availability. An alternative has been the increasing use of cellular therapies derived from human Embryonic Stem Cells (hESC), showing very promising results in maturation, yield and ultimately, in insulin secretion in response to adequate stimuli. We recently developed a new technique for cellular transplantation under the skin. This manuscript evaluates the capabilities of the pre-vascularized Device-Less (DL) site to allow transplantation of Pancreatic Endoderm (PE) cells differentiated from hESC to treat diabetes mellitus. Fifty immunodeficient mice, n = 25 diabetic and n = 25 non-diabetic, were transplanted with PE cells. Animals were followed for 22 weeks and grafts were retrieved to evaluate engraftment and subsequent maturation. Diabetic mice showed slightly better engraftment (48% vs. 36%, p = 0.19) and secreted higher concentration of human C-peptide upon glucose stimulation (0.32 ± 0.15 ng/mL vs. 0.13 ± 0.09 ng/mL, p = 0.30), although differences were not significant. This maturation was not sufficient to successfully reverse diabetes. Monomorphic cystic changes were detected in 12% and 8%, respectively (diabetics vs. non-diabetics, p = 0.32) and all grafts seemed to be adequately contained by the surrounding collagen wall within the DL space. Our findings support the capabilities of the DL site to host PE cells and allow safe maturation as a new strategy to treat diabetes.
The recent advances in immunotherapy have allowed Islet Transplantation (IT) to become a mainstay treatment for Type 1 Diabetes Mellitus (T1DM). Today, the procedure is safer and long-term graft survival is comparable to that of pancreas transplant alone, with a reduced risk for complications [1,2]. Nonetheless, the IT procedure is limited by donor availability and usage. Significant variability is associated with this treatment modality and many factors may affect the successful utilization of a donated pancreas. In fact, the entire donation-transplant process depends upon many variables related to the donor clinical characteristics, the type of donation (living, brain death, cardiac death, etc.), the outcomes of islet isolation, and recipient characteristics. As a consequence, the process is not always efficient and like other transplant types, the demand may surpass the available donation pool.
An alternative to IT may be to use renewable sources for insulin secretion from proliferative stem cell populations. In particular, research using insulin-producing cells derived from human embryonic stem cells (hESC) has shown very promising results in maturation yield and ultimately, in insulin secretion in response to adequate stimuli [3-6]. The focus is now on optimizing the existing differentiation protocols to allow for a successful and stable diabetes reversal. However, finding the most efficient transplant site remains a dilemma given the infusion volume needed at the time of transplant and the potential need for graft retrieval in the event of tumor formation [7,8]. These reasons are a deterrent to use the conventional intra portal route for this transplantation modality.
Our group recently described a novel pre-vascularized Device-Less (DL) technique for cell transplantation in the subcutaneous space [9]. This approach was successful in reversing diabetes with mouse and human islets and is currently being used for other cell therapies. We herein describe the use of the DL technique to safely allow engraftment and maturation of Pancreatic Endoderm (PE) cells derived from a hESC line in an experimental xeno-transplant model of diabetes.
Human Embryonic Stem Cells-derived Pancreatic Endoderm
Pancreatic Endoderm (PE) cells derived from a human embryonic cell line were kindly provided by Drs. M.C. Nostro and G. Keller at the McEwen Centre for Regenerative Medicine in Toronto. Their differentiation protocol uses a combination of cytokines and small molecules to simulate pancreatic development and produces multipotent pancreatic progenitor cells with the potential to differentiate into all pancreatic lineages [10,11]. At the time of transplant, cells were harvested and shipped overnight to Edmonton for immediate implantation.
Transplantation of PE cells
Immunodeficient 8-12 week B6.129S7-Rag1tm1Mom mice (Jackson Laboratory, Bar Harbor, ME, USA) were used for all experiments. Animals (n = 50) were housed under conventional conditions with access to food and water ad libitum and their care was in accordance with guidelines approved by the Canadian Council on Animal Care.
The DL space was created as previously reported by inserting a nylon catheter subcutaneously in the left lower abdomen and left for five weeks before transplant [9].Diabetes was chemically induced by intraperitoneally injecting 180 mg/kg of streptozotocin (STZ; Sigma-Aldrich, ON, Canada) in half of the recipients, one week prior to transplantation. Mice were considered diabetic after two consecutive blood glucose measurements ≥ 11.3 mmol/L (350 mg/dL).
Two groups of mice (diabetics and non-diabetics, n = 25/group) were transplanted with approximately 7×106 PE cells using the DL technique. Animals in the diabetic group also received two consecutive insulin-releasing pellets (LinBit®; LinShin Canada Inc. Toronto, ON, Canada - ~0.1 U insulin/24 hours/30 days) to maintain health for the duration of the study (160 days). A separate group of four mice (two diabetics and two non-diabetics) were transplanted with same amount of PE cells and sacrificed four week post-transplant for early assessment of the graft. All mice were continuously monitored for general health, weight gain and non-fasting blood glucose, as well as the occurrence of tumor formation.
C-peptide Measurements
Blood samples were also obtained at post-transplant week 4, 8, 12, 16, 20 and 22 to quantify stimulated human C-peptide concentration in plasma. Mice from both groups were fasted overnight and whole blood was collected after intraperitoneal injection of glucose (2 g/kg). Quantification of C-peptide was performed using human-specific ultrasensitive ELISA (Mercodia, Uppsala, Sweden. Detection range: 5 - 280 pmol/L (0.015 - 0.85 ng/mL).
Histology
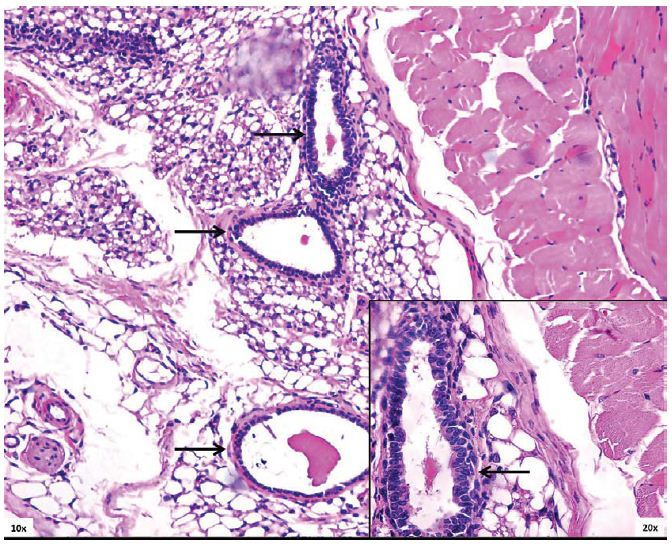
Engrafted cells were analyzed at early (four weeks post-transplant) and at the end of the study. Hematoxylin and eosin (H&E) and Masson’s trichrome stains were used to visualize the grafts on abdominal wall sections and to assess tumor boundaries. Immunofluorescence was used to evaluate endocrine secretory function of long-term engrafted cells using anti-insulin (Dako A0082 – Alexa 568) and anti-glucagon (Abcam – Vector Fl-1000) antibodies. The procedure followed previously established methodology [9] and it included deparaffinization, primary and secondary antibody treatment and counter stain with DAPI (Invitrogen Molecular Probes. Eugene, Oregon). Slides were visualized using a fluorescent microscope with appropriate filters and AxioVision imaging software (Carl Zeiss Microscopy GmbH. Jena, Germany).
Transplantation of Human Islets
In parallel, human islets were transplanted into 8-12 week B6.129S7-Rag1tm1Mom diabetic mice and monitored for 22 weeks to compare human C-peptide secretion levels to those achieved by the study PE cells. The Clinical Islet Transplantation laboratory at the University of Alberta kindly provided human islets after the process of donation, isolation and culture, as reported in previous publications [12]. Permission for these studies was granted by the Health Research Ethics Board of the University of Alberta, Edmonton, Alberta, Canada, and after written permission was obtained from donor families.
Mice were rendered diabetic by intraperitoneal injection of 180 mg/kg streptozotocin (STZ, Sigma-Aldrich, ON, Canada). Animals were considered diabetic after two consecutive blood glucose measurements ≥ 11.3 mmol/L (350 mg/dL). Recipients (n = 6 per group) received 0 IEQ (Sham and STZ), 1,000 IEQ and 3,000 IEQ human islets from three different isolations. Islets from each isolation were randomly allocated to each group and transplanted under the kidney capsule as previously described [13]. Mice in the Sham group were not diabetic and underwent the transplant procedure, but only received a saline solution under the kidney capsule. Animals in the STZ group were chemically-induced diabetics and did not receive transplant, remaining diabetic throughout the entire study.
Animals were periodically monitored for general health, weight and blood glucose until endpoint (22 weeks) when blood samples were taken to determine basal and stimulated human C-peptide levels.
A total of 54 mice received 7×106 PE cells/mouse subcutaneously, using the DL technique. Four weeks after transplantation, a viable graft was found in all four sacrificed animals, showing clear features of ductal formations (Figure 1). However, all animals remained diabetic and no detectable human C-peptide was found at this early time point (data not shown).
Twenty weeks after transplantation stimulated C-peptide was detected in both groups and continued to increase until the end of the study. Positive stimulated C-peptide was found in 12 of 25 (48%) mice in the diabetic group vs. 9 of 25 (36%), in non-diabetic (p = 0.19). Mean stimulated C-peptide concentrations at 22 weeks were higher in the diabetic group although differences were not statistically significant (0.32 ± 0.15 ng/mL vs. 0.13 ± 0.09 ng/mL, p = 0.30) (Figure 2A).
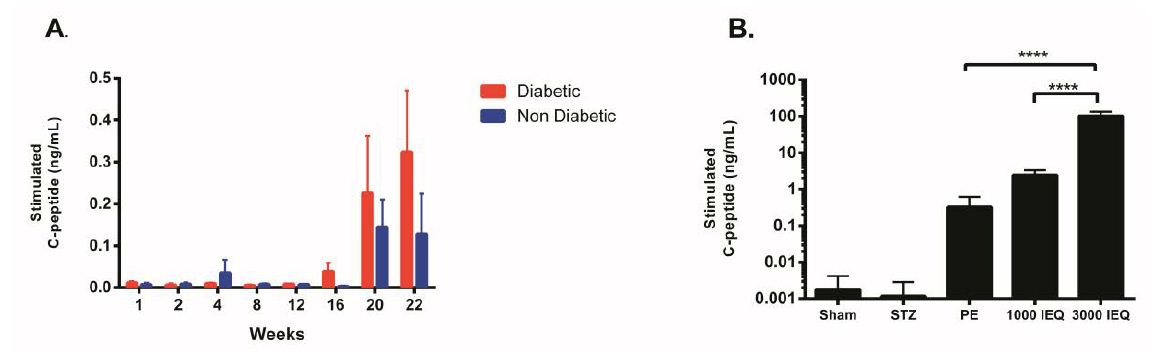
Figure 2: Stimulated C-peptide secretion from transplanted pancreatic endoderm (PE) cells; A. Secretory profile over time for diabetic and nondiabetic mice, showing detectable C-peptide beyond 20 weeks post-transplant; B. Comparison of C-peptide secretory capabilities of transplanted PE cells vs. human islets at minimal and full dose transplanted in immunodeficient mice. A Sham and STZ (diabetic, non-transplanted) groups are included for comparison and specificity of the assay.
Our findings corroborate the utility of the DL technique to facilitate cell therapies. In this case, the aim was to engraft and mature PE cells derived from hESC, and measure indicators towards diabetes reversal.
In our study design we evaluated the potential effect of underlying hyperglycemia for engraftment and maturation of PE cells based on published evidence for accelerated maturation under a chronic hyperglycemic environment [14]. Results confirmed an increased trend in both, maturation and mean concentration of stimulated human C-peptide levels measured at 22 weeks in diabetic mice. Differences however, did not reach statistical significance. C-peptide positive measurements were specific to engrafted cells from human origin, proving to be a valuable tool for assessment of maturation of transplanted PEs.
The process of effective differentiation of hESC is very complex and yet to be fully elucidated. Many authors agree on the multiple hurdles these cells encounter in the process of maturation and only recently, successful in vivo maturation have been reported with adequate glucose-response and occasionally, diabetes reversal [15-19].
Consistent with previous studies, the PE cells we tested in our experiments require a long (more than five months) in vivo maturation period [10,17,20,21].
Despite observing adequate engraftment in almost half of the animals, glucagon staining was predominant in most of the histology samples and positive insulin cells were only occasionally found, which is consistent with the low levels of stimulated c-peptide detected at week 22, as well as failure to correct hyperglycemia. We speculate that longer in vivo maturation or a higher number of hESC-derived PE cells at the time of transplantation may be required to normalize glucose control in diabetic mice, although a more prominent insulin staining has been previously reported when transplanting these cells in the kidney subcapsular space and mammary fat pad [10]. Further experimentation will definitely be required to fully understand the maturation process in this new transplant site.
One of the main limitations for the use of hESC is the inherit risk for teratoma transformation [7]. This is one of the rationales for using alternative transplant sites like the DL technique where a dysfunctional/transforming graft may be easily retrieved. Current differentiation protocols are now focused on producing hESC preparations with a high grade of purity to avoid residual undifferentiated cells, which could potentially lead to tumor formation [22]. In our series of transplants benign monomorphic cystic formations were present in 8 - 12% of cases and no teratoma was detected.
An interesting finding was that resulting cysts were successfully contained by the peripheral collagen wall present in the DL space during the 22-week observation period. This resulted in a restrictive effect similar to that present in other physical devices [14,18]. However, the real restraining capabilities in the settings of a true teratoma formation are still to be proven.
In conclusion, our subcutaneous DL technique has proven to be an adequate host for these human embryonic stem cells - derived pancreatic endoderm, allowing effective engraftment, maturation and added protection against tumor formations. This is certainly an important field of application for this technique and a starting point for further experimentation with improved cell preparation and transplant protocols.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
