
Research Article | DOI: https://doi.org/10.31579/JHV-2021/021
*Corresponding Author: K. C. Bhuyan, Department of Statistics, Jahangirnagar University, Dhaka Bangladesh
Citation: K. C. Bhuyan. (2021) Socioeconomic variables responsible for hypertensive heart disease among Bangladeshi adults. J, Heart and Vasculature 1(5); DOI: 10.31579/JHV-2021/021
Copyright: © 2021, K. C. Bhuyan, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 May 2021 | Accepted: 17 July 2021 | Published: 20 August 2021
Keywords: socioeconomic variables, hypertension, heart disease, risk ratio, discriminant analysis, correlation coefficient of discriminant function score and socioeconomic variable
The information presented here were the analytical results of data collected from a sample of 995 adults of age 18 years and above residing in both urban and rural areas of Bangladesh. The respondents were investigated to identify some responsible variables for prevalence of hypertensive heart disease in them. In the sample 50.1% were males and for them the risk of hypertensive heart disease was 57% more as it was in females. The percentages of urban residents, non-Muslims, married persons, eldest group of adults, higher educated people, retired persons, and persons from richest families in respect of income and expenditure were 46.4, 14.8, 93.1, 8.0, 57.5, 12.3, 12.6 and 13.5, respectively. All these groups of adults had more chance to be affected by the disease. The risk of prevalence of hypertensive heart disease in obese adults (31.4%), diabetic adults (67%), smokers (33.1%), process food consumers (36.5%), physically inactive persons (48.3%) and adults involved in sedentary activity (44.4%) were too high. However, the most responsible variable for prevalence was body mass index followed by duration of diabetes, smoking habit, family income, age, sedentary activity and family expenditure. These were identified by discriminant analysis.
Hypertension also called elevated blood pressure when blood pressure ≥ 140 / 90 and hypertensive heart disease refers to heart conditions caused by elevated blood pressure [1, 2, 3, 4 ]. Longstanding hypertension leads to heart failure and most of the patients with heart failure have a history of hypertension [5]. It is the most common modifiable risk factor for premature cardiovascular disease (CVD) and it coexists with other major risk factors such as heart failure, and stroke [1, 5, 6, 7, 8]. It is also responsible for 13% global death [9]. Three-quarters of the world’s hypertensive people reside in low-and – middle-income countries and the problem prevails more in Southeast Asia, particularly in Bangladesh [7, 9]. In Bangladesh, approximately 20% of adults and 40 – 65% of elderly people suffer from hypertension [10, 11]. Current prevalence rate of hypertension is 20-25% among adults in Bangladesh [12]. Again, obesity is the risk factor not only for hypertension but also for diabetes [13]. People with both diabetes and hypertension have approximately twice the risk of cardiovascular diseases compared to the people with non-diabetic hypertension [14]. The prevalence of hypertension among diabetic patients is around three times compared to the people of non-diabetic hypertension [15]. Hypertension prevailed in around 30 % patients of type 1 diabetes and 50 – 60% patients of type 2 diabetes [16]. In separate studies, it was reported that diabetes had a role in the development of hypertension, especially type 2 diabetes around 2.5 times likely to develop in patients with hypertension compared to subjects having normal blood pressure [17, 18]. Simultaneous occurrence of obesity and hypertension in the same individual doubles the risk of cardiovascular deaths [19].
Obesity is one of the most risk factors for the development of hypertension and both these health hazard are recognized as public health challenges [20, 21]. This problem is in increasing trend worldwide. The number of adults with hypertension will be increasing by approximately 60% to a total of 1.56 billion in 2025 in comparison with 2000 [20].
Obesity and its associated cardiovascular and renal disorders are major threat to global health [20, 21]. The problem is nearly doubled since 1980 and tripled in 2025. In 2016, WHO reported that the overweight adults were 1.9 billion and obese adults were 650 million throughout the world [22]. Simultaneous occurrence of obesity and hypertension in the same individual doubles the risk of cardiovascular deaths [23]. Obesity and its associated cardiovascular and renal disorders are major threat to global health [20, 24, 25]. The problem is nearly doubled since 1980 and tripled since 1975 [26].
The above mentioned facts indicate that obesity, diabetes, hypertension and CVD are inter-related non-communicable diseases. In some studies it was noted that hypertension, diabetes, body mass index , intake of excess fatty acid and salty food, age, gender, occupation, family income and expenditure , lifestyle related factors, sedentary activity, physical inactivity, non-adherence to antihypertensive treatment, family history of the disease, were associated with CVD [1, 11, 27, 28, 29, 30, 31, 32].
Keeping the above mentioned facts and information the plan was formulated to identify the socioeconomic variables responsible for hypertensive heart disease among Bangladeshi adults.
According to the objective of the study the data were recorded from 995 adults of age 18 years and above by quota sampling plan to cover males and females in the ratio 50.1: 49.9 as this ratio is prevailed in the national level of population of Bangladesh [33]. Out of 995 respondents 498 were males and 497 were females and they were the residents of both urban and rural localities. As the adults were investigated from diagnostic centre, most (67%) of them were found diabetic patients.
The data were collected during the session 2018-19 by some nurses with the help of medical assistants working in some diagnostic centres. The centres were selected from urban and semi-urban areas by convenience sampling plan. The information of different socioeconomic variables of each selected respondent were recorded through a pre-designed and pre-tested questionnaire which contains different questions related to residence, religion, gender, marital status, age, education, occupation, family income, etc. Beside these personal data, other information were on life-style, and prevalence of any of the non-communicable diseases, duration of diabetes, and the stages of treatment of the disease along with the information of family income and family expenditure. Some of the variables were qualitative and some were quantitative in nature, but all the variables were recorded in nominal scale for ease of analysis. The data of weight ( in kg ) divided by height ( in metre2) was used to measure the value of body mass index (BMI) to identify obese adults (if BMI ≥ 27.5; underweight ,if BMI< 18>
To fulfil the objective of the study, the association of each of socioeconomic variable with simultaneous prevalence of hypertensive heart disease was investigated, where significant association was decided if p-value of any was ≤ 0.05. Irrespective of significant or insignificant association, the risk ratio and its confidence interval was calculated for adults for whom prevalence of hypertensive heart disease was noted in higher rate for a particular level of a socioeconomic variable. Finally, discriminant analysis was done to discriminate the adults of hypertensive heart disease from other adults. In discriminating the respondents the identification of some variables were done which were responsible for this discrimination. The responsible variables were identified by the higher absolute values of correlation coefficients with discriminant function score and variable values [36, 37, 38]. All the calculations were done using SPSS Version 25.
The respondents were classified by prevalence of non-communicable disease and level of blood pressure. Among the respondents 60.9% were free of any non-communicable disease except diabetes. The other 39.1% had different types of health hazard. Their percentages were shown in Table 1.

It was seen that 5.9% people were hypertensive and 30.5% of them had heart problem. The level of blood pressure and type of disease of the respondents were significantly associated [X2=133.365,p-value=0.000]. In the sample 18 (1.8%) adults were the patients of hypertensive heart disease and the remaining 977 respondents were free of this health problem. Hence we had two groups of respondents and these two groups were classified by different levels of socioeconomic variables and the association of each of the socioeconomic variable with prevalence of hypertensive heart disease was investigated.
The sample contained 46.4% urban adults and 2.4% of them were patients of hypertensive heart disease [Table 2]. They had 80% more chance of affecting by the disease compared to the chance of rural adults [R.R=1.80, C.I{0.704,4.603]. But hypertensive heart disease was independent of residence as was observed by Chi-square test [X2= 1.544, p-value=0.214]. The percentage of male respondents was 50.1 and 2.2% of them were facing the problem of hypertensive heart disease. For them the risk of the disease was 57% more than that of females [R.R.=1.57, C.I.{0.618,9.025}]. However, prevalence of hypertensive heart disease was not significantly different for gender variation [X2= 0.897, p-value= 0.344]. Non-Muslim adults were only 14.8% but 2.7% of them were affected by this health hazard and they had 65% more chance to face this problem as it was in Muslim adults [R.R= 1.65, C.I.{0.583, 4.672}]. Rate of prevalence of hypertensive heart disease was not significantly different for both the religious groups [X2= 0.808, p-value=0.369]. The chance of prevalence of hypertensive heart disease among married adults (93.1%) was 22% more as it was in others [R.R.=1.22,C.I.{0.165,9.025}]. However, marital status was not associated with prevalence of hypertensive heart disease
[X2= 0.054, p – value=0.816].
Age was significantly associated with prevalence of hypertensive heart disease [X2= 14.054,p-value=0.007].The rate of prevalence was in increasing trend with the increase in age.
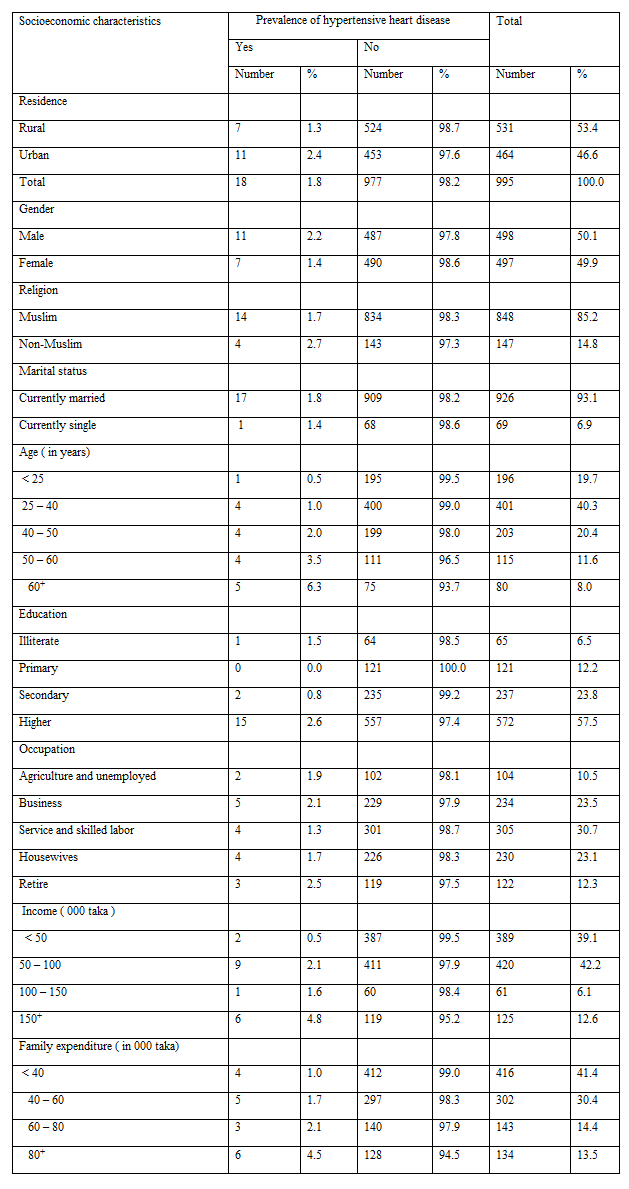
The percentage of adults of age 60 years and above was 8.0 and 5.3% of them were patients of hypertensive heart disease. For them the chance of affecting by the problem was 4.40 times as it was for other adults [R.R.=4.40,C.I.{ 1.610,11.951}]. The sample higher educated adults were 57.5% and 2.6% of them were suffering simultaneously from hypertension and heart disease. This group of adults had 2.70 times more chance of affecting by this health hazard compared to the chance of others [ R.R.= 3.70, C.I.{ 1.308,12.695}].There was no significant trend in the rate of prevalence of hypertensive heart problem with the increase in level of education [X2=5.629, p-value= 0.131]. In the sample there were 12.3% retired persons and 2.3% of them were the patients of hypertensive heart problem. They had 43% more chance of facing this health problem compared to the chance of other professionals [R.R.=1.43,C.I.{ 0.420,4.868}]. Prevalence of hypertensive heart disease was not significantly associated with occupation [X2=0.871, p-value=0.929]. The percentage of adults not involved in physical labour was 51.7% and 2.5% of them were the patients of hypertensive heart disease. Their chance of affecting by the problem was 2.43 times as it was for others [R.R.=2.43,C.I.{ 0.874,6.760}]. However, prevalence of hypertensive heart disease was not statistically associated with involvement in physical labour [X2= 3.104,p –value= 0.078]. The percentage of respondents involved in sedentary activity was 44.4 and 2.9% of them were the patients of hypertensive heart disease. Among them the chance of prevalence of the problem was 3.25 times as it was in others [R.R.=3.25,C.I.{1.168,9.041}]. The prevalence of this health hazard was significantly associated with the utilization of time by the adults [X2= 5.738, p –value = 0.017].
The percentage of adults coming from highest income group of families was 12.6 and 4.8% of them were the patients of hypertensive heart problem. For them the chance of facing the problem of hypertensive heart disease was 3.48 times as it was in others [ R.R.=3.48, C.I.{ 1.329,9.110}]. Though there was no increasing trend in the rate of prevalence of hypertensive heart disease with the increase in level of family income , yet level of family income was significantly associated with prevalence of this health hazard [X2=10.241, p-value=0.014]. However, family expenditure was not statistically associated with the prevalence of this health problem [X2=7.161, p –value= 0.067]. But adults belonged to families spending highest amount of money as family expenditure was worst sufferers (4.5%) from the problem. In this group there were 13.5
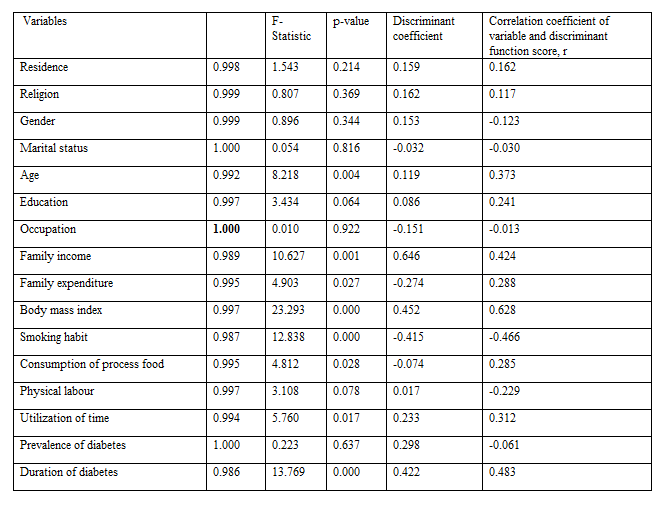
It was seen that some of the socioeconomic variables were significantly associated with prevalence of hypertensive heart disease and particular level of a variable was the risk factor for this health problem. But no variable was identified as the most responsible one for the prevalence of this health hazard. The responsible variable was identified in discriminating the hypertensive heart problem patients from other group. For discrimination the variables included were residence, religion, gender, marital status, age, education, occupation, family income and expenditure, body mass index, smoking habit, consumption of process food, physical labour, utilization of time, prevalence of diabetes and duration of diabetes. Out of these variables age, family income and family expenditure, body mass index, smoking habit, consumption of process food, and utilization of time and duration of diabetes were significantly different for two groups of adults. The most responsible variable in discriminating the groups was body mass index followed by duration of diabetes, smoking habit, family income, age, utilization of time, etc. The results were shown in Table 3. The two groups of adults were significantly discriminated [X2= 0.944,X2=56.937, p-value=0.000].
Hypertension is the most common modifiable risk factor for cardiovascular diseases and often prevails with other major health hazard [39]. The risk of hypertension and heart disease are strongly associated with obesity [40]. Impact of longer duration of hypertension and chronic blood pressure leads to heart failure [7, 39]. Other risk factors of hypertensive heart disease are older age, consumption of high sodium and fatty food, occupation without physical labour, sedentary activity, longer duration of diabetes, family history of heart disease, non-adherence to control high blood pressure and antihypertensive treatment [8, 11, 27 – 32, 41-42].
Most of the risk factors for hypertensive heart disease are socioeconomic and socio-demographic except clinical aspects. In this paper, an attempt was made to identify some of the responsible factors in discriminating 18 hypertensive heart patients from the remaining 977 respondents. Out of total 995 investigated respondents 46.4% were from urban areas, 14.8% were non-Muslims, 50.1% were males. For these three groups of adults the risks of hypertensive heart disease were 80%, 65% and 57%, respectively more than those of others. But these 3 demographic characteristics were not important in discriminating the hypertensive heart patients from other group. Another demographic characteristic was marital status but the risk of the diseases were almost similar for single and married adults. There were only 8% elderly people and 57.5% higher educated people. For these two groups the risks of the disease were 4.40 and 3.70 times as these were for others. Out of these two variables, age was important in discriminating two groups of adults. The risks of the disease for retired persons, physically inactive persons and persons involved in sedentary activity were 1.43, 2.43 and 3.35 times compared to those of their counter parts. But except sedentary activity the other variables had little influence in discriminating the two groups of adults.
The lifestyle factors are family income and expenditure, smoking habit and habit of taking process food [5]. These 4 variables were significantly different for two groups of adults. The risks of the disease for adults coming from highest income and highest family expenditure groups, process food consumers and smokers were 3.48, 3.21, 2.43 and 5.26, times, respectively than those of others. Out of these 4 characteristics, smoking habit and family income were the third and fourth responsible factors in discriminating the two groups of adults.
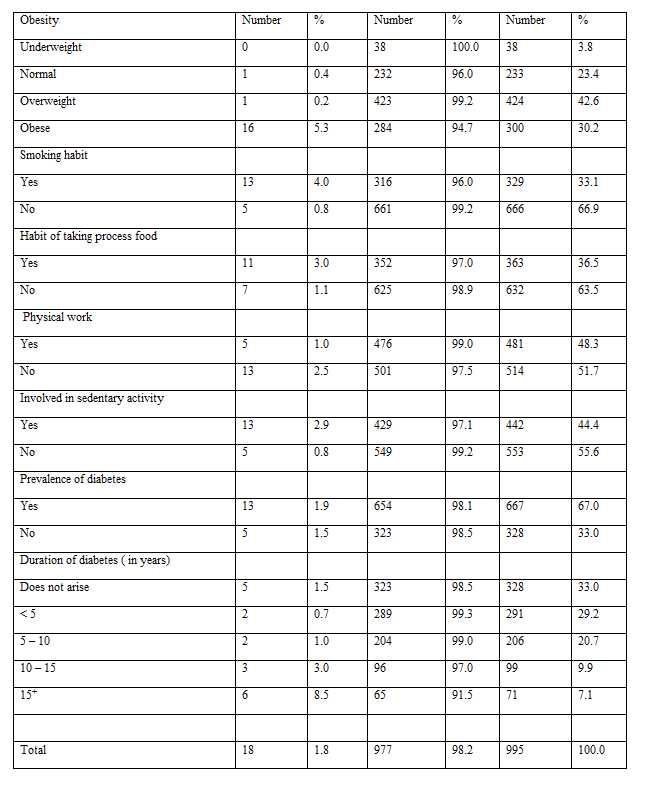
Obesity and diabetes are inter-related health problem for many adults. These were noted in many studies in both home and abroad [43-46]. These two health problems are also the sources of hypertensive heart disease [1, 11, 27]. The present study also indicated that obese and diabetic adults were at higher risk of facing the problem of hypertensive heart disease. The chance of prevalence of the problem among obese adults was 18.53 times compared to that of non-obese adults. The variable body mass index was the most responsible one to discriminate the two groups of adults. Longer duration of diabetes was another risk factor for this health problem. Those who were suffering for 15 years and above their risk of this health hazard was more than six times compared to the risk of others. Duration of diabetes was the second most responsible variable for discrimination.
The objective of the present study was to identify some responsible socioeconomic variables for hypertensive heart disease among Bangladeshi adults of 18 years and above. For the purpose, data were collected from 995 respondents of both urban and rural localities. The information presented here were the analytical results of the collected data from the investigated respondents. To identify the responsible variables discriminant analysis was performed. Before that, the risk ratio for adults belonged to a particular level of a socioeconomic variable was calculated.
Among the respondents 1.8% were the patients of hypertensive heart disease. These respondents were significantly different from others in respect of the variables body mass index, duration of diabetes, smoking habit, family income, age, utilization of time, etc. Out of these variables, the most responsible one was the body mass index. The second responsible one was duration of diabetes. These variables were identified depending on the absolute values of correlation coefficients of the variable and discriminant function scores. The other variables were presented here according to the decreasing values of correlation coefficient.
The sample obese respondents were 31.4% and for them the risk of the prevalence of the disease was 18.53 times compared to the risk of non-obese adults. Around seven per cent (7.1%) adults were suffering from diabetes for 15 years and above. For them the risk of prevalence was 6.01 times as it was in others. Smoker respondents were 31.4%, their risk of prevalence was 5.26 times as it was in non-smokers. The percentage of adults of highest income group of families was 12.6. Their risk of prevalence was 3.34 times compared to the risk of other adults. There were 8% elderly people, for them the risk was 4.40 times as it was for adults of ages below 60 years. Those who were involved in sedentary activity (44.4%) their risk of facing the problem of hypertensive heart disease was 3.25 times compared to the risk of others.
The risks of prevalence were also more for urban people, non-Muslim adults, males, married people, higher educated people, retired persons, process food consumers, and physically inactive adults. Out of these variables, only process food consumption and prevalence of hypertensive heart disease were significantly associated.
Due to upward movement towards economy and social status lifestyle has been changing. As a result, obesity, diabetes, hypertension and impacts of these cannot be avoided. One of the major impact is heart disease. Thus there is every possibility of increasing trend of hypertensive heart disease unless precaution is not adopted to control obesity, diabetes and hypertension. As a precautionary measure the following steps can be taken:
Rural and urban health workers can suggest the people to follow the above steps.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
